Download presentation
Presentation is loading. Please wait.

1
Surveillance: The Public Health Version of CSI March 2006 Connie Austin and Judy Conway Illinois Department of Public Health

3
Outline of Surveillance Talk Basics of Surveillance Uses of Surveillance Limitations of Surveillance Future of Surveillance Examples of Surveillance in Action in Illinois Infectious Disease Quiz

4
Public Health Surveillance Systematic, ongoing Collection “get data” Analysis & Interpretation turn data into information” Dissemination “route to those who need it” Link to public health practice “do something about it”

7
Building Block of Surveillance All surveillance starts with the single case who is brought to the attention of public health by a laboratory, HCP or other party and who’s risk factors are investigated by the LHD CD investigator

8
Three Main Features of Surveillance Systematic Collection Consolidation and Evaluation of Data Prompt Dissemination of Results to Those Who Can Take Action

9
Public Health Approach ProblemResponse Surveillance: What is the problem? Risk Factor Identification: What is the cause? Intervention Evaluation: What works? Implementation: How do you do it?

10
Legal Authority For Conducting Surveillance Diseases and conditions to be reported Who is responsible for reporting What information is required for each case How, to whom and how quickly must cases be reported Control measures to be taken for specific diseases

12
IDPH LHD

13
Reportable Infectious Diseases, 2006 67 reportable infectious diseases in Illinois 56 diseases/conditions are nationally notifiable to CDC 3 are reportable to WHO

14
Primary Data Sources for Surveillance Lab reports Health care providers Death certificates Animals/insects

15
Modes of Surveillance Passive Surveillance: Wait for reports Enhanced Passive surveillance: Health alerts to encourage rapid reporting Communication and relationship building with hospitals and clinicians Active surveillance: Actively querying or auditing clinical sites for cases; expensive and more often part of “ramping up”

16
The Public Health Team Health care providers Other Experts Epidemiologists Communicable Disease Investigators IT persons Support staff

17
Allied Surveillance Useful to Infectious Disease Surveillance Biowatch-environmental monitoring for BioT agents in big cities Biosense

18
Uses of Surveillance Identify cases for investigation and followup Estimate magnitude of the problem Determine trends in incidence and distribution Detect sudden increases in disease- Outbreak detection

19
Uses of Surveillance (cont) Generate hypotheses, stimulate research Evaluate prevention and control measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning
 Generate hypotheses, stimulate research Evaluate prevention and control measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning")
20
Uses of Surveillance Identify cases for investigation and followup Estimate magnitude of the problem Determine geographic distribution of disease Detect sudden increases in disease- Outbreak detection

21
Situations Requiring Prophylaxis of Contacts

22
Uses of Surveillance Identify cases for investigation and followup Estimate magnitude of the problem Determine trends in incidence and distribution Detect sudden increases in disease- Outbreak detection

23
Enterics in Illinois, 2001-2003

24
Uses of Surveillance Identify cases for investigation and followup Estimate magnitude of the problem Determine trends in incidence and distribution Detect sudden increases in disease- Outbreak detection

25
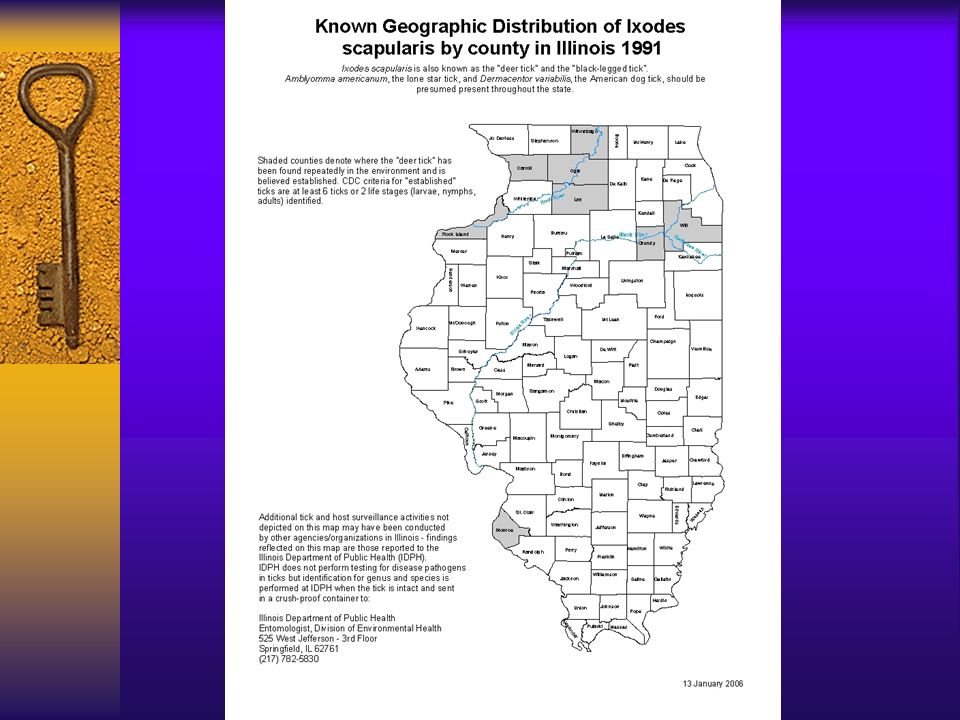
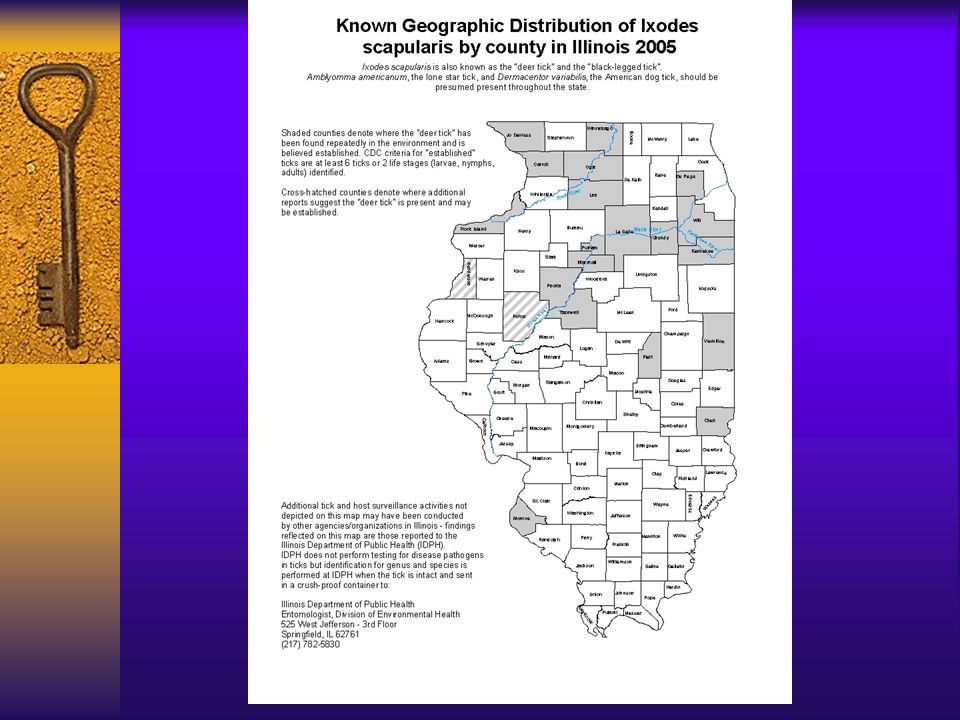
Lyme Disease Cases Reported in Illinois, 1995-2005

26
Lyme Disease Exposures in 3 Counties in Illinois, 1995-2005

29
Uses of Surveillance Identify cases for investigation and followup Estimate magnitude of the problem Determine trends in incidence and distribution Detect sudden increases in disease- Outbreak detection

30
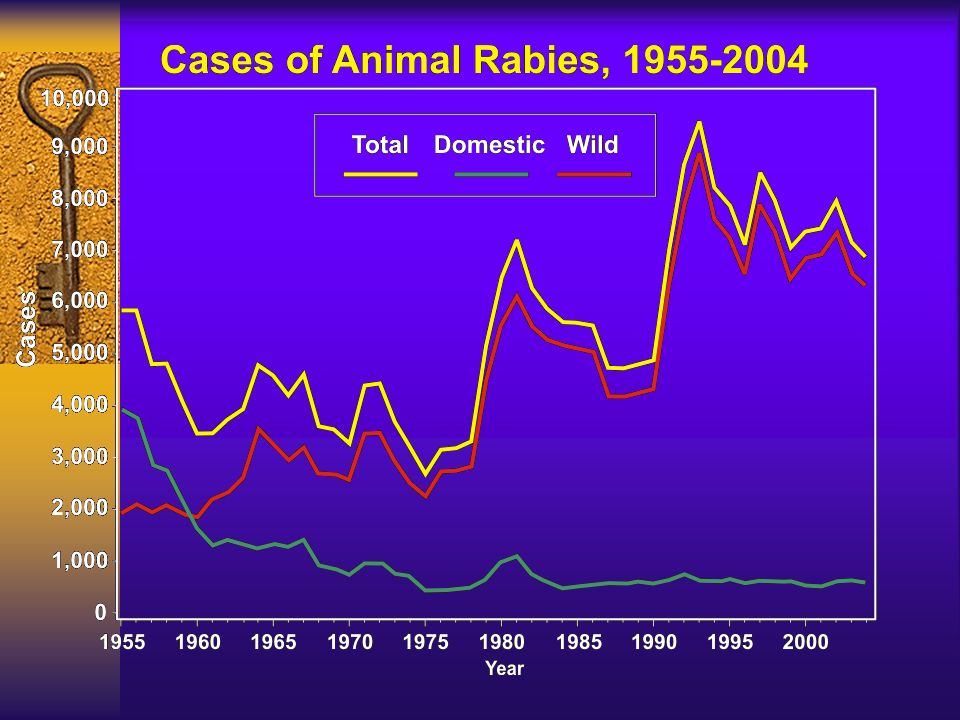
Surveillance-Outbreak Identification S. enteritidis, Kankakee, 2002 Histoplasmosis, Iroquois County, 2003 Rabies, 2004&2005

31
Uses of Surveillance Generate hypotheses, stimulate research Evaluate control and prevention measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning

32
TOXIC SHOCK SYNDROME (TSS) United States, 1983-1998 TOXIC SHOCK SYNDROME (TSS) United States, 1983-1998 *Includes cases meeting the CDC definition for confirmed and probable cases for staphylococcal TSS. 1983 1984 1985 198619871988 1989 19901991 1992 199319941995199619971998 National Center for Infectious Diseases (NCID) data* National Electronic Telecommunications System for Surveillance (NETSS) data 0 2020 4040 6060 8080 10 0 12 0 14 0 16 0 Year (Quarter) Reported Cases
 data* National Electronic Telecommunications System for Surveillance (NETSS) data Year (Quarter) Reported Cases.")
33
Reported Toxic Shock Syndrome in Illinois, 1980-2004

34
Investigation leads to prevention

35
Uses of Surveillance Generate hypotheses, stimulate research Evaluate control and prevention measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning

36
Poliomyelitis (Paralytic) NOTE: Inactivated vaccine was licensed in 1955. Oral vaccine was licensed in 1961. Year 0 0 5 5 10 15 20 25 30 35 40 45 50 55 60 1968 1973 1978 1983 1988 1993 1998 Reported Cases Source: CDC. Summary of notifiable diseases. 1998. Rate/100,000 Population Year Inactivated Vaccine Oral Vaccine United States, 1968-1998

37
Rabies, potential human exposure 15% of rabies PEP unnecessary Improper timing of rabies PEP in 1/3 of cases Improper location for injections in 1/3 of cases Given properly in 43% of cases

38
Uses of Surveillance Generate hypotheses, stimulate research Evaluate control and prevention measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning

40
Brucellosis in Humans and Cattle in Illinois, 1951-2004

41
Trends in Pertussis in Illinois by Age Group (1998 through December 2004)
")
42
Uses of Surveillance Generate hypotheses, stimulate research Evaluate control and prevention measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning

43
Examples of Changes in Health Practices

44
Uses of Surveillance Generate hypotheses, stimulate research Evaluate control and prevention measures Monitor long-term changes/trends in infectious agents Detect changes in health practices Facilitate planning

45
What Diseases Should be Under Surveillance? Cause serious morbidity and/or mortality Have the potential to affect additional people beyond the initial case Can be controlled or prevented with an intervention Any outbreak or unusual increase in a disease Any unusual case/cluster

46
Competing Interests CDC State Health Department Local Health Departments Citizens and action groups Health Care providers Politicians

48
Types of Infectious Diseases Under Surveillance Diseases transmitted from food/drinking water Diseases requiring contact tracing for prophylaxis Vaccine preventables Diseases requiring environmental control measures New/emerging/unusual infections

49
Diseases transmitted from food/drinking water Enterics-Salmonella, E. coli O157:H7 Other-botulism, Listeria etc PH responses –Restrict foodhandlers –Remove contaminated foods from commerce –Find problem in manufacturing process

50
Examples of diseases requiring contact prophylaxis Hepatitis A N. meningitidis Rabies Exposures

51
Vaccine Preventables Examples: H. influenzae, Hepatitis A and B, pertussis, chickenpox, influenza PH Response –Increasing vaccination rates in risk groups

52
Diseases Requiring Environmental Control Measures Examples: outbreaks of legionellosis, leptospirosis, histoplasmosis, cryptosporidiosis, arboviruses PH Response –Recommendations on how to decrease exposure to organism and prevent further cases

53
New/Emerging/Unusual Examples: monkeypox, bioterrorism agents

56
Limitations of Surveillance System Underreporting

57
Limitations (continued) Representativeness Timeliness Inconsistency of case definitions
 Representativeness Timeliness Inconsistency of case definitions")
58
Characteristics of Good Public Health Surveillance Qualified and dedicated personnel Teamwork approach to investigations Strong relationships with reporters Strong relationships with partners-other LHDs, state and federal partners

59
Characteristics of Good Public Health Surveillance (cont) Templates and database resources available on hand 24/7/365 availability Always stay alert/open minded
 Templates and database resources available on hand 24/7/365 availability Always stay alert/open minded")
60
Ways to Improve Surveillance Improve awareness of reporters Simplify reporting Frequent feedback Active surveillance

61
What’s Up in the Future for Infectious Disease Surveillance in Illinois??? INEDSS –Faster reporting –LHDs have access to their own data Electronic Reporting from labs Electronic death certificate data? IDPH-Intranet resources for each reportable disease, A-Z

62
Surveillance/Epi Response overview “Signal” –Call from clinician/hospital –Syndrome threshold/trigger –Environmental trigger Early Epi Investigation –Targeted questions for MD, Patient –Laboratory work up –Environmental investigation –Cross-Evaluation data from all systems –Enhance surveillance/ Actively look for more cases Outbreak investigation

63
Examples of Surveillance in Action in Illinois

64
PIAPO-Assessing Surveillance Data Problem? Investigation needed? Assessment of the situation Plan of Action Over?

65
Example 1 CDC’s BioSense Crimean hemorrhagic fever

66
Biosense Reports On the following dates there were reports of Crimean Hemorrhagic Fever cases from Illinois VA or DOD facilities: 10/5, 10/6, 10/28, 11/1, 11/1, 11/2,12/2,12/13

67
Example 2 Meningococcal disease

68
Wednesday, October 14

69
Friday, October 17

70
Investigation? Information to be gathered?

71
Meningococcal Disease Clusters Vaccine available for serogroup A/C/Y/W-135. No vaccine for serogroup B. Cluster requiring vaccination –3 or more probable or confirmed cases of serogroup C in < 3 months –Attack rate of >=10 per 100,000 population

72
Saturday, October 18

73
Information gathered All six cases are male Ages range from 27 to 42 years of age Residents of the north side of City A All 4 confirmed cases are SG C 3 of 6 cases were fatal

74
Assessment What is your assessment?

75
Action Plan Health care providers were notified Public has been notified Vaccination clinics

76
Vaccination Campaign Began Oct 19 with 5 vaccination sites Recommendations for vaccination Flow of persons Time frame

77
Example 3

78
Single Case?

79
Positive Rabies Test You receive a call from a physician who reports a patient has tested positive for rabies What do you do?

80
Additional Information Gathered Test was an ELISA test for rabies, not approved for diagnosis of human rabies; test was equivocal Person visited Mexico, returned and has been hospitalized for a month and is on a ventilator but can watch TV and is alert.

81
Assessment?

82
Plan of Action

83
Example 4. Is this a problem?

84
Further Information from Investigation Bitten by a sheep 3 weeks prior while preparing sheep for a county fair

85
Assessment and Plan?

86
Example 5

87
Campylobacter cluster 3 cases of Campylobacter come thru from a provider into your in-box in INEDSS on the same day

88
Assessment and Plan?

90
Example 6 Problem?

91
Investigation?

92
Information Obtained 2 persons were from same household Family had purchased a hooded rat from a chain pet store Rat became ill

93
Purchase rat Onset of rat illness Onset of mother’s illness Onset of daughter’s illness Death of rat

94
Traceback of rat Rats purchased by pet store from Distributor A in Arkansas This distributor was also implicated in other states

95
November 3, 2004 Report Pet Store Chain in Illinois calls to report they had a hamster that died suddenly and was culture positive for S. ser. Typhimurium

96
Findings Hamster purchases IDPH laboratory testing U.S. summary Rodents-antimicrobials

97
Plan of Action

98
Example 7

99
Background On August 12, a LHD was alerted to 5 lab-confirmed Cryptosporidium cases Problem?

100
Problem? Crypto cases reported per year in this jurisdiction: 4

101
Investigation?

102
Investigation Upon investigation, all confirmed cases reported swimming in the municipal facility prior to illness

103
Investigation? Is this enough information to take action?

104
Action Steps

105
Laboratory Investigation 12 persons had laboratory-confirmed cryptosporidiosis The pools had been hyper-chlorinated; no water samples were available for testing

109
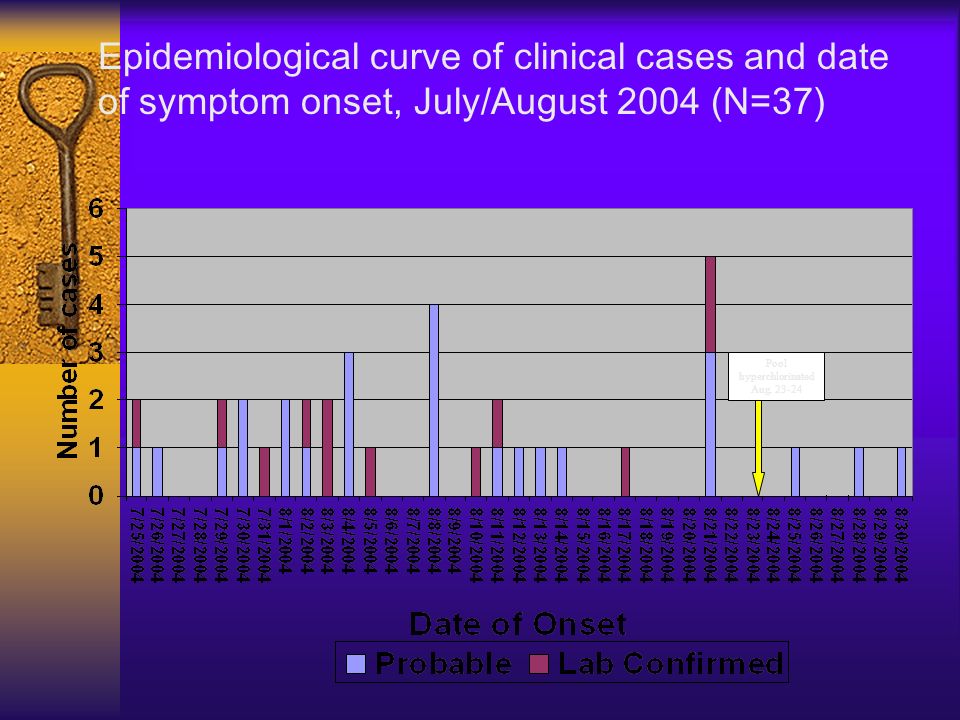
Epidemiological curve of clinical cases and date of symptom onset, July/August 2004 (N=37) Pool hyperchlorinate d Aug. 23-24
110
Conclusions A visit to the pool facility was linked to becoming ill with cryptosporidiosis The wading pool was a likely source of infection though other explanations are possible Improved fecal accident response may reduce risk of disease transmission Cryptosporidium remained in the pool water even though chlorine levels were generally adequately maintained

111
Example 8

112
Background IDPH notified by the LHD on March 25 about an outbreak of GI illness in two groups eating food from a single caterer on February 25

115
Investigation

116
Do you cancel your catered luncheon from this facility?

117
Caterer inspection No major problems Obtained invoice information Employees were ill –Problem?

118
Epi Findings Cases included 14, 17, 19 and 2 from the four groups, respectively Group 1-13 of 14 ills ate pasta salad and/or tuna salad Group 2-pasta salad Group 3-multiple including tuna sandwich and pasta salad Group 4-tuna salad sandwiches and mixed green salad

119
Epi continued

120
1970 Surgeon General Statement “it was time to close the book on infectious diseases, declare the war against pestilence won, and shift national resources to such chronic problems as cancer and heart disease”

123
Pets

Similar presentations