Download presentation
Presentation is loading. Please wait.

1
Approach to the Patient With Chest Pain Eric J Milie D.O.

2
Objectives Establish a differential diagnosis for the patient with chest pain Recognize clues in the history and physical exam to rule in or rule out various etiologies of chest pain Outline a basic treatment strategy for the treatment of a patient’s chest pain

3
General Rule out most medically critical causes of chest pain first General appearance of the patient Look through the chart Good history

4
Differential Ischemia or infarction PE Pneumothorax Pericarditis Tamponade Pneumonia Aortic Dissection GERD Shingles Musculoskeletal

5
Myocardial Infarction/ Ischemia: History Pressure type pain (elephant on chest) Central to left sided pain, radiation to jaw Worse with activity, relieved with rest Relief with nitro Nausea, diaphoresis, syncope, SOB Enquire about risk factors: HTN, hyperlipid, diabetes, previous cardiac history, smoker, family history, etc “Pain within six feet of the chest in a diabetic is an MI until proven otherwise.”
 Central to left sided pain, radiation to jaw Worse with activity, relieved with rest Relief with nitro Nausea, diaphoresis, syncope, SOB Enquire about risk factors: HTN, hyperlipid, diabetes, previous cardiac history, smoker, family history, etc Pain within six feet of the chest in a diabetic is an MI until proven otherwise.")
6
Physical Appearance: Does the patient look ill? Levine’s sign Hypotension: cardiogenic shock Bradycardia: high grade block Tachycardia: sichemia related tachyarrhythmia Increased JVD, palpable liver, peripheral edema: Right sided heart failure Crackles, S3: left sided failure

7
Levine’s Sign 80% sensitive, but only 51% specific

8
Investigations EKG: Should be knee jerk response to any chest pain, SOB, etc CXR: Rule out heart failure, anatomical cause for pain Cardiac enzymes: Not always initially positive. CKMB will begin to rise within 6 hours, elevated for 48 hours, troponin rises within 12 hours, elevated for two weeks

9
Treatment Morphine Oxygen Nitro Aspirin Lasix (if failure) Inotropes (if shock) Streptokinase, TPA, Retaplase, or Integrillin if EKG criteria met (discuss with attending) Anticoagulate (heparin)
 Inotropes (if shock) Streptokinase, TPA, Retaplase, or Integrillin if EKG criteria met (discuss with attending) Anticoagulate (heparin)")
10
Pulmonary Embolus Sudden onset of sharp chest pain Worse with inspiration Anxious patient, sense of “impending doom” Risk factors: immobilization, venous insufficiency, trauma, known DVT, pregnancy, malignancy, clotting disorder

11
PE: Physical Anxious Tachycardia, tachypnea, hypoxia Hypotension and syncope possible Look for unilateral calf swelling

12
Investigations ABG: ↓PaO2 and PaCO2 CXR: Frequently normal EKG: nonspecific ST/T changes or sinus tachycardia most common (“classic” S1Q3T3 seen in less than 11% of known PE’s) D-Dimer: Sensitive but not specific; lag time of up to 24 hours here Spiral CT of the chest: quick, easy with good sensitivity and specificity
 D-Dimer: Sensitive but not specific; lag time of up to 24 hours here Spiral CT of the chest: quick, easy with good sensitivity and specificity")
13
Management Anticoagulate with wt based heparin, TPA only if hemodynamically unstable from large saddle embolus Supportive treatment with fluids, oxygen Intubate if unable to maintain oxygenation or patient fatiguing

14
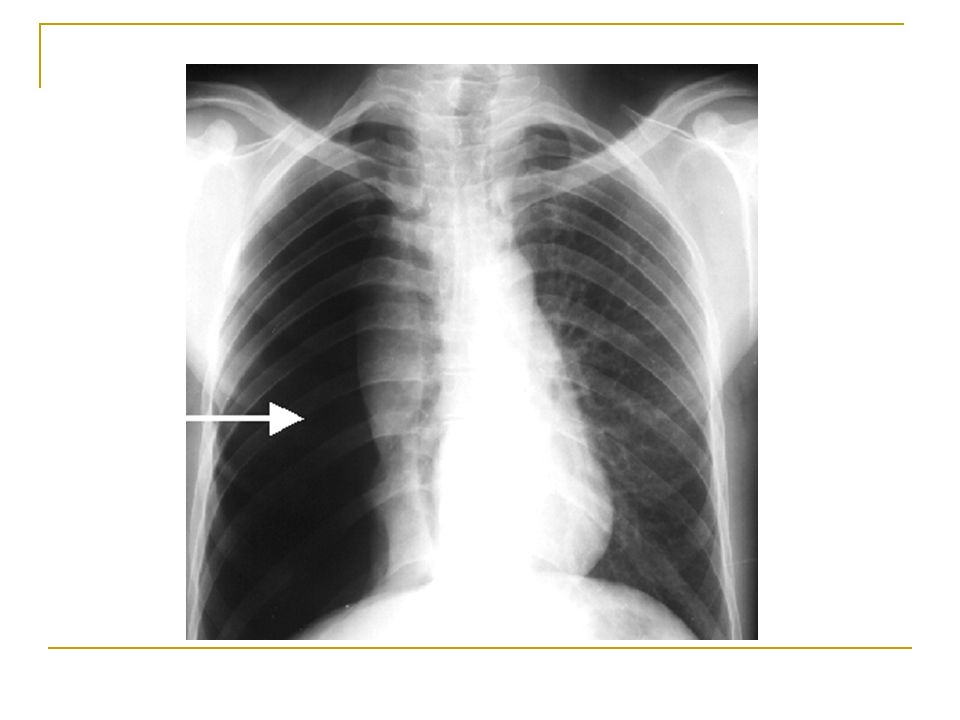
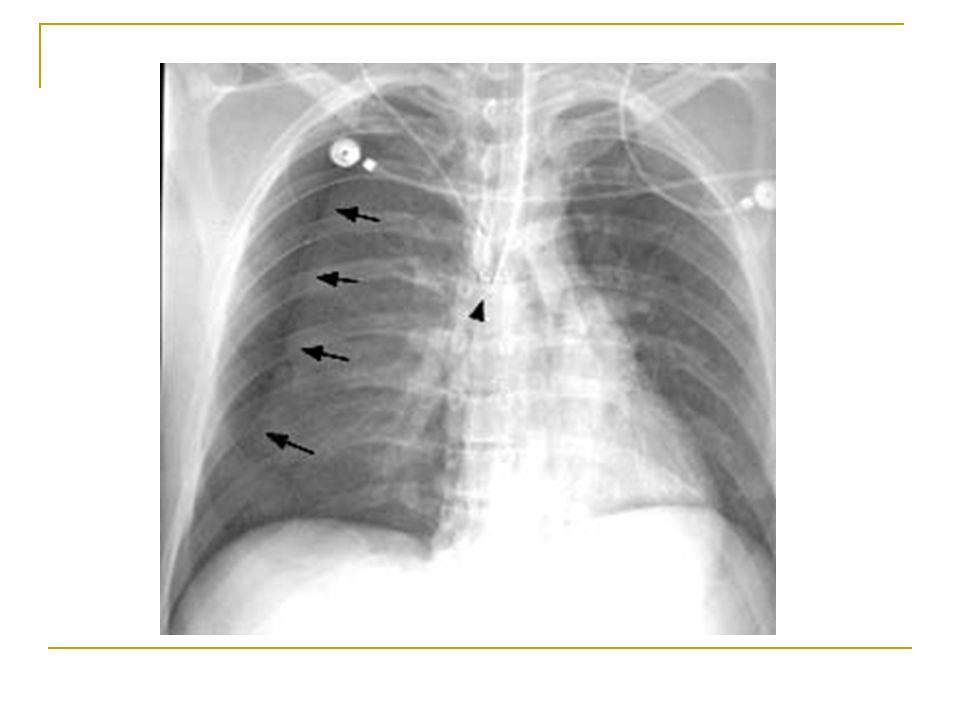
Pneumothorax: History Acute pleuritic chest pain or dyspnea Primary pneumo in young, healthy, tall, thin white males Secondary: procedures (CVP), ruptured bleb in COPD patient, barotrauma (bagging during code, improper vent settings), or necrotic neumonia/empyema
, ruptured bleb in COPD patient, barotrauma (bagging during code, improper vent settings), or necrotic neumonia/empyema")
15
Physical Decreased expansion of the chest Hyperresonnant percussion If tension pneumo, may see deviation of traches and progressive hypotension, decreased cardiac output- emergency

16
Investigation Chest x-ray

19
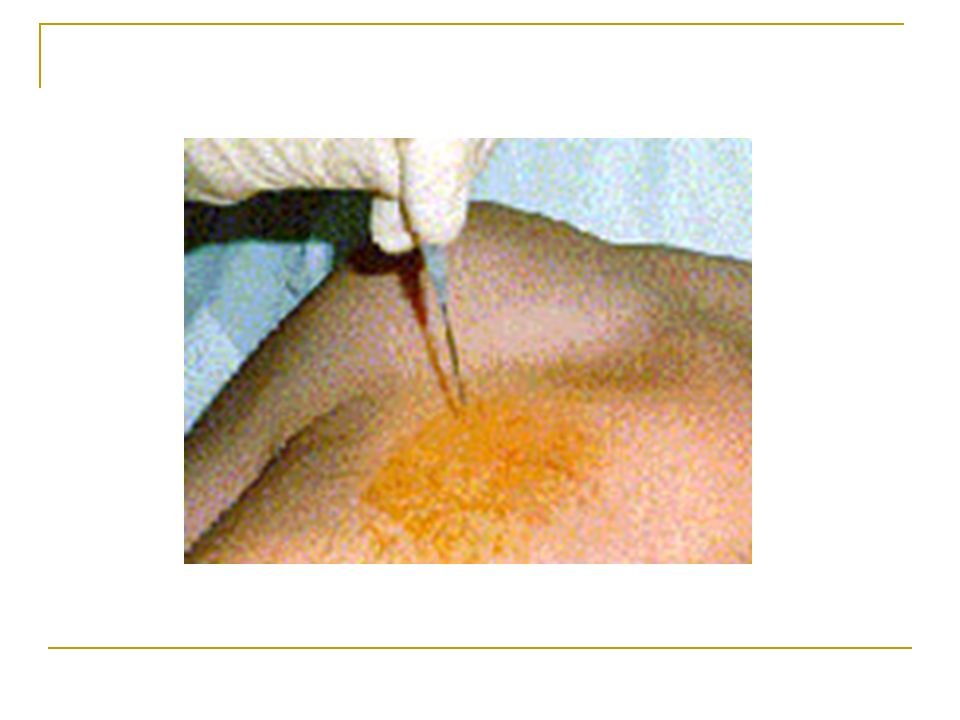
Management Watchful waiting for small, asymptomatic pneumo Chest tube for large, hemodynamically unstable Emergent: large bore needle to the 2 nd intercostal space, midclavicular line

Similar presentations







 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")

, FCCP>")






 Risk factors (associated diseases) Physical signs Investigations Complications and treatment.>")


) Dr. Walaa Nasr Lecturer of Adult Nursing Second year Second.>")