Download presentation
Presentation is loading. Please wait.

1
RHEMATOID ARTHRITIS DR MUZAMIL SHAHZAD PROFESSOR OF MEDICINE

2
Rheumatoid arthritis (RA) is the most common persistent inflammatory arthritis, occurring throughout the world and in all ethnic groups.
 is the most common persistent inflammatory arthritis, occurring throughout the world and in all ethnic groups.")
3
female to male ratio of 3:1. The clinical course is prolonged, with intermittent exacerbations and remissions. Patients with RA have an increased mortality when compared with age- matched controls, primarily due to cardiovascular disease.

4
Pathophysiology Both genetic and environmental factors appear to be involved in the pathogenesis of RA

5
RA is characterised by infiltration of the synovial membrane with lymphocytes, plasma cells and macrophages. CD4+ T cells play a central role by interacting with other cells in the synovium

6
Clinical features Criteria for diagnosis of rheumatoid arthritis* Diagnosis of RA is made with four or more of the following: Morning stiffness (> 1 hr) Arthritis of three or more joint areas Arthritis of hand joints Symmetrical arthritis Rheumatoid nodules Rheumatoid factor Radiological changes Duration ≥ 6 wks
 Arthritis of three or more joint areas Arthritis of hand joints Symmetrical arthritis Rheumatoid nodules Rheumatoid factor Radiological changes Duration ≥ 6 wks")
7
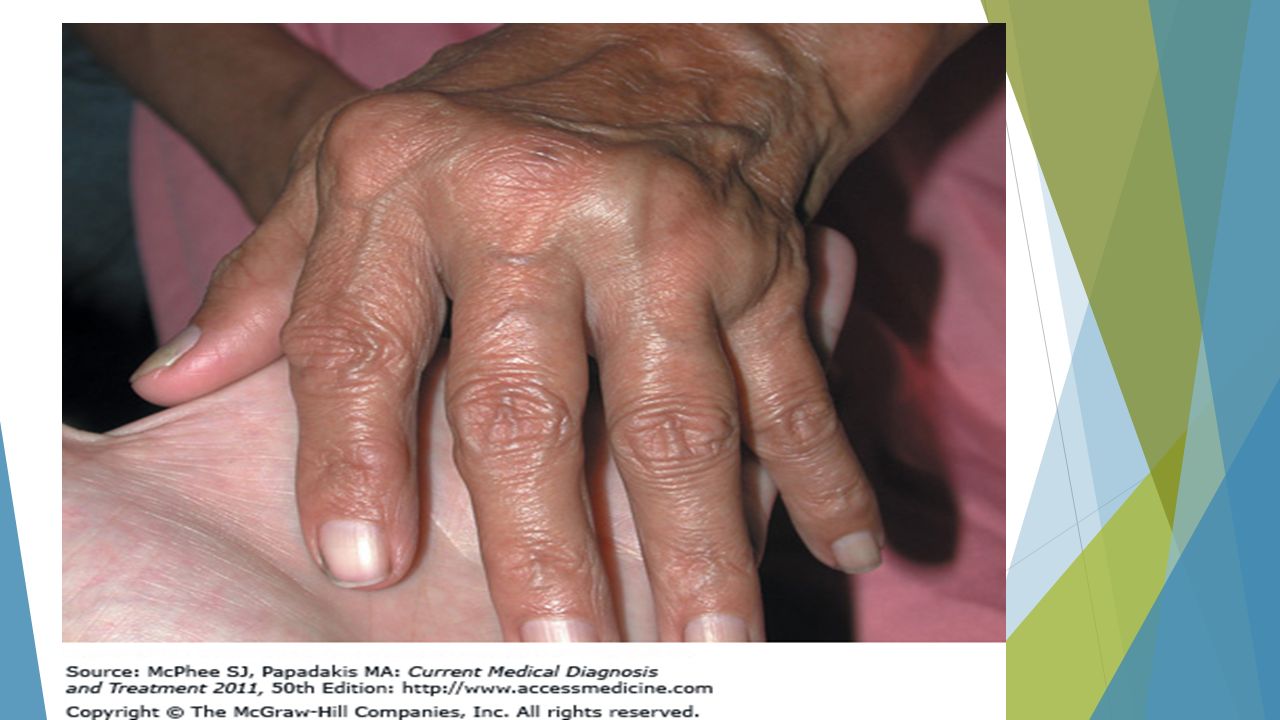
The typical presentation is with pain, joint swelling and stiffness affecting the small joints of the hands, feet and wrists. Large joint involvement, systemic symptoms and extra- articular features may also occur

8
Examination of the hands often provides a good reflection of overall disease activity. The typical features are symmetrical swelling of the metacarpophalangeal (MCP) joints and proximal IPJs. These and other joints are actively inflamed if they are tender on pressure, and have stress pain on passive movement or effusion/soft tissue swelling
 joints and proximal IPJs. These and other joints are actively inflamed if they are tender on pressure, and have stress pain on passive movement or effusion/soft tissue swelling.")
9
Characteristic deformities develop with long-standing disease, including 'swan neck' deformity, the boutonnière or 'button hole' deformity, and a Z deformity of the thumb

10
Sometimes RA has a very acute onset, with florid morning stiffness, polyarthritis and pitting oedema. This occurs more commonly in old age

11
Occasionally, the onset is palindromic, with relapsing and remitting episodes of pain, stiffness and swelling which last only for a few hours or days

12
Dorsal subluxation of the ulna at the distal radio-ulnar joint is common and may contribute to rupture of the fourth and fifth extensor tendons. Triggering of fingers may occur because of nodules in the flexor tendon sheaths.

13
In the foot, dorsal subluxation of the MTP joints may result in 'cock- up' toe deformities. This causes pain on weight-bearing on the exposed MTP heads and development of secondary adventitious bursae and callosities

25
Anorexia, weight loss and fatigue are common and may occur throughout the disease course. Generalised osteoporosis and muscle- wasting (sarcopenia) result from systemic inflammation.
 result from systemic inflammation..")
26
Popliteal ('Baker's') cysts usually occur in combination with knee synovitis, where synovial fluid communicates with the cyst but is prevented from returning to the joint by a valve-like mechanism. Rupture, often induced by knee flexion in the presence of a large effusion, leads to calf pain and swelling

27
Extra-articular features are most common in patients with long-standing seropositive erosive disease but may occasionally occur at presentation, especially in men. Most are due to serositis, granuloma/nodule formation or vasculitis

28
Cutaneous and vascular features Rheumatoid nodules occur almost exclusively in seropositive patients, usually at sites of pressure or friction such as the extensor surfaces of the forearm, sacrum

30
Rheumatoid vasculitis usually occurs in older seropositive patients in the context of systemic symptoms and multiple extra-articular features. Vasculitis can vary from the relatively benign nail-fold infarcts to widespread cutaneous ulceration and skin necrosis. Involvement of medium-sized arteries can lead to mesenteric, renal or coronary artery occlusion

31
Extra-articular manifestations of rheumatoid disease

32
Systemic Fever Weight loss Fatigue Susceptibility to infection

33
Musculoskeletal Muscle-wasting Tenosynovitis Bursitis Osteoporosis

34
Haematological Anaemia Thrombocytosis Eosinophilia

35
Lymphatic Felty's syndrome Splenomegaly

36
Nodules Sinuses Fistulae

39
Ocular Episcleritis Scleritis Scleromalacia Keratoconjunctivitis sicca

46
Vasculitis Digital arteritis Ulcers Pyoderma gangrenosum Mononeuritis multiplex Visceral arteritis

47
Cardiac Pericarditis Myocarditis Endocarditis Conduction defects Coronary vasculitis Granulomatous aortitis

48
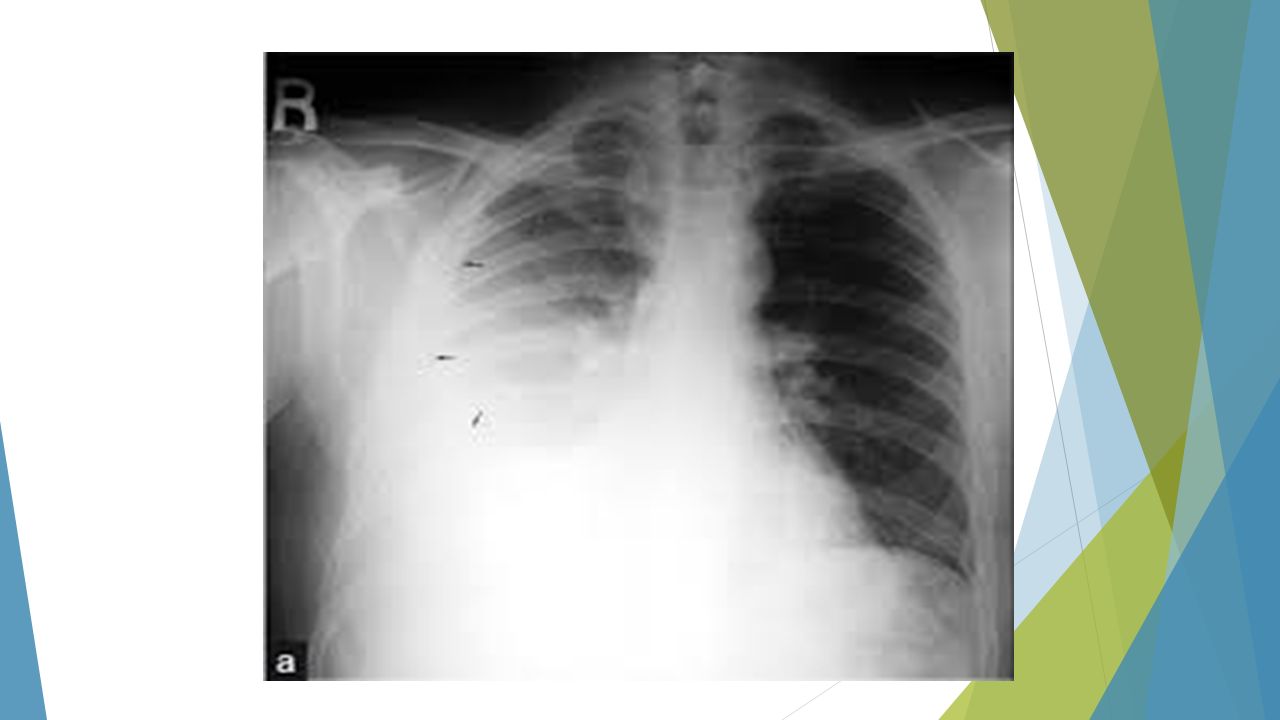
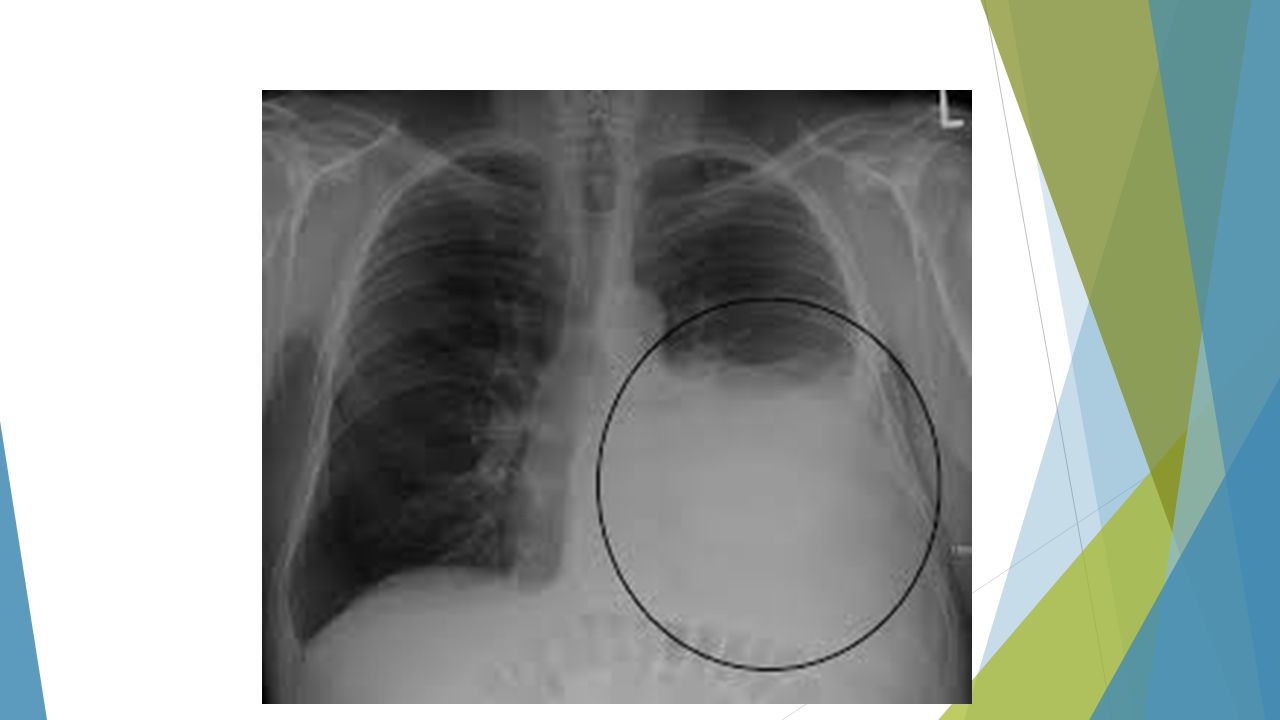
Pulmonary Nodules Pleural effusions Fibrosing alveolitis Bronchiolitis Caplan's syndrome

53
Neurological Cervical cord compression Compression neuropathies Peripheral neuropathy Mononeuritis multiplex

55
Amyloidosis

56
INVESTIGATIONS ESR and CRP are usually raised (acute phase response), but may not be in patients with isolated small joint arthritis. RF and anti-CCP antibodies are detected in 60- 80% of patients but their absence does not exclude the diagnosis. A positive anti-CCP antibody is highly specific for RA and can occur before clinical onset of the disease.

57
RF is non-specific; low titres are found in about 10% of the normal population and in other diseases (

58
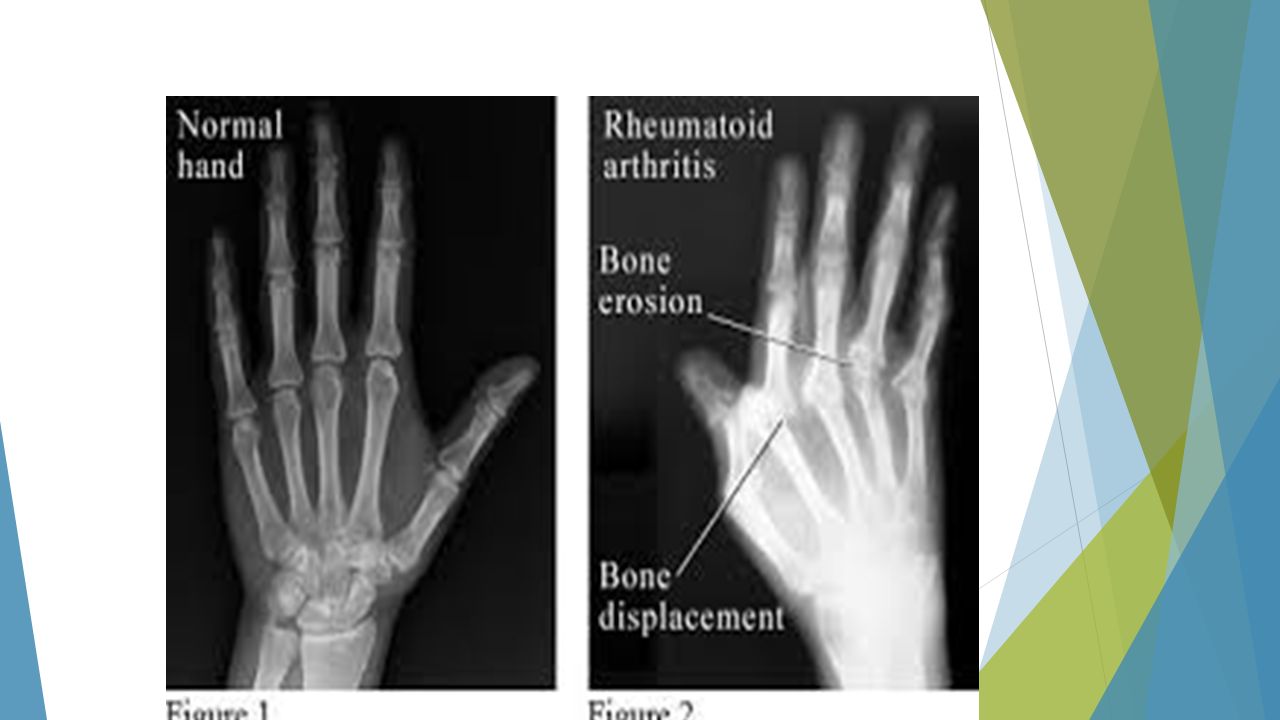
Plain X-rays of the hands, wrist and feet are useful. Periarticular osteoporosis is common during the early stages of disease and may be present within 6 months of onset. Non-proliferative marginal joint erosions on X-ray are characteristic, but uncommon within the first year

64
Ultrasound and MRI are more sensitive than X-rays at detecting early erosions. Patients who are suspected of having atlanto-axial disease should have lateral X-rays taken in flexion and extension, and the degree of cord compression should be established with MRI.

65
In patients with Baker's cyst, Doppler ultrasound and an arthrogram may be required to establish the diagnosis, since deep venous thrombosis (DVT) and Baker's cyst may coexist
 and Baker s cyst may coexist")
66
Management Physical rest, targeted anti-inflammatory therapy passive exercises are the mainstays, with the aim of relieving symptoms, suppressing inflammation, and conserving and restoring function in affected joints

67
A multidisciplinary approach is required, including doctors, nurses, physiotherapists and occupational therapists, and patient education and counselling play a key role.

68
During treatment, periodic assessment of disease activity, progression and disability is essential. In the vast majority, management is outpatient- based, but hospital admission can be helpful in patients with .

69
very active disease for a period of bed rest, multiple joint injections, splinting, regular hydrotherapy, physiotherapy and education

70
Nonsteroidal Anti- inflammatory Drugs NSAIDs provide some symptomatic relief in rheumatoid arthritis but do not prevent erosions or alter disease progression. They are not appropriate for monotherapy and should only be used in conjunction with DMARDs.

71
NSAIDs work in arthritis by the same mechanism that causes side effects: inhibition of COX, the enzyme that converts arachidonic acid to prostaglandins

72
Celecoxib, a selective COX-2 inhibitor, is FDA-approved for the treatment of osteoarthritis and rheumatoid arthritis.

74
Compared with traditional NSAIDs, COX- 2 inhibitors are as effective for treating rheumatoid arthritis but less likely in some circumstances to cause upper gastrointestinal tract adverse events (eg, obstruction, perforation, hemorrhage, or ulceration).
.")
75
Corticosteroids Low-dose corticosteroids (eg, oral prednisone 5–10 mg daily) produce a prompt anti- inflammatory effect in rheumatoid arthritis and slow the rate of bony destruction. However, their multiple side effects limit their long-term use.

76
Low-dose corticosteroids often are used as a "bridge" to reduce disease activity until the slower acting DMARDs take effect or as adjunctive therapy for active disease that persists despite treatment with DMARDs. No more than 10 mg of prednisone or equivalent per day is appropriate for articular disease

77
Intra-articular corticosteroids may be helpful if one or two joints are the chief source of difficulty. Intra-articular triamcinolone, 10–40 mg depending on the size of the joint to be injected, may be given for symptomatic relief, but not more than four times a year

78
Synthetic DMARDs Methotrexate Methotrexate is usually the initial synthetic DMARD of choice for patients with rheumatoid arthritis. It is generally well tolerated and often produces a beneficial effect in 2–6 weeks. The usual initial dose is 7.5 mg of methotrexate orally once weekly.

79
If the patient has tolerated methotrexate but has not responded in 1 month, the dose can be increased to 15 mg orally once per week. The maximal dose is usually 20–25 mg/wk. The most frequent side effects are gastric irritation and stomatitis. Cytopenia, most commonly leukopenia or thrombocytopenia but rarely pancytopenia, due to bone marrow suppression is another important potential problem

80
Hepatotoxicity with fibrosis and cirrhosis is an important toxic effect that correlates with cumulative dose and is uncommon with appropriate monitoring of liver function tests. Methotrexate is contraindicated in a patient with any form of chronic hepatitis.

81
Sulfasalazine This drug is a second-line agent for rheumatoid arthritis. It is usually introduced at a dosage of 0.5 g twice daily and then increased each week by 0.5 g orally until the patient improves or the daily dose reaches 3 g. Side effects, particularly neutropenia and thrombocytopenia, occur in 10–25% and are serious in 2–5%.

82
Leflunomide

83
Antimalarials

84
Biologic DMARDs Tumor necrosis factor inhibitors Five inhibitors are in use: etanercept, infliximab, adalimumab, golimumab, and certolizumab pegol.

85
Etanercept, a soluble recombinant TNF receptor:Fc fusion protein, is usually administered at a dosage of 50 mg subcutaneously once per week.

86
Infliximab, a chimeric monoclonal antibody, is administered at a dosage of 3–10 mg/kg intravenously; infusions are repeated after 2, 6, 10, and 14 weeks and then are administered every 8 weeks

87
Rheumatoid arthritis in old age 25.55 Rheumatoid arthritis in old age Presentation: may be atypical-for example, with an initial polymyalgic picture or with synovitis and marked peripheral oedema.

88
Increasing age and comorbidity (e.g. cardiac, renal, gastrointestinal tract disease): increase the risks of NSAID gastrotoxicity; comorbidity can also make overall management more difficult.
: increase the risks of NSAID gastrotoxicity; comorbidity can also make overall management more difficult..")
89
Corticosteroid-induced osteoporosis: increased risk in those aged > 65 yrs. Bisphosphonates should be co-prescribed in those on corticosteroid therapy for > 3 mths. DMARD and biologic therapy: age alone is not a contraindication

90
Surgery Synovectomy of the wrist or finger tendon sheaths of the hands may be required for pain relief or to prevent tendon rupture when medical interventions have failed. In later stages when joint damage has occurred, osteotomy, arthrodesis or arthroplasty may be required

Similar presentations



























 Immunomodulatory and immunosuppresive Xenobiotic – Gold salts – Azathioprine – Methotrexate Biological.>")




 25 th Nov 2013.>")







 M:F 1:3 Age range:>")





