Download presentation
Presentation is loading. Please wait.

1
Venous Thromboembolism: Diagnosis and Managament
R. Cavalcanti and B. Laluck April, 2007

2
Learning objectives Review factors affecting risk of VTE
Understand an approach to diagnosis of VTE Review aspects of treatment of VTE

3
Outline Cases Diagnostic algorithm Prophylaxis
Type and duration of anticoagulation IVC filters

4
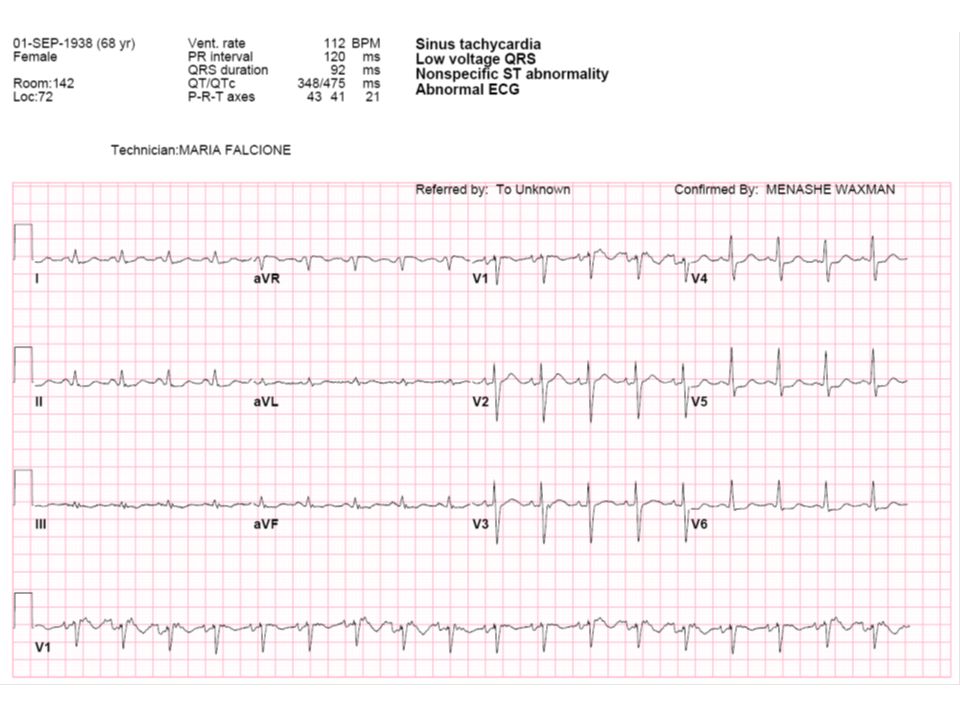
Case 1 68F Post op day #2 after R TKR Referred for fever + SOB
PMHx: HTN, osteoporosis, 40pyr smoker Meds: Alendronate, Atenolol/HCTZ, Dalteparin 5000, Moxifloxacin Over 2 d has needed increasing O2

5
Case 1 (cont) Inv: OE: CBC: 98 11.7 318 Lytes 138 104 3.5 26
HR110 RR24 BP90/50 SPO2 90% on 50%FM T 38.5 CVS N hs; JVP 4-5 cm ASA Chest: Fine crackles over bases, long expiratory time Inv: CBC: Lytes ABG: on FiO2 0.5

8
CT Angio Chest No PE Diffuse interstitial changes consistent with pulmonary edema Left lower lobe opacity

9
Case 2 23 F presents with shortness of breath
OCP, smoker and recently flew in from Berlin Now requires 2L O2 NP for SpO2 96%

10
Case 3 83 F presenting with BRBPR Doppler US LE: Positive for DVT
C-Scope: large rectal tumour Unilateral R leg swelling Doppler US LE: Positive for DVT Management?

11
Tests for VTE Wells score: D-dimers: Venous Doppler US CT Angio Chest
VQ scan Conventional pulmonary angiography

12
Estimating risk

14
Risk of DVT

15
Wells Prediction Rule for Diagnosing Deep Venous Thrombosis: Clinical Evaluation Table for Predicting Pretest Probability of Deep Vein Thrombosis Clinical Characteristic Score Active cancer (treatment ongoing, within previous 6 months, or palliative) 1 Paralysis, paresis, or recent plaster immobilization of the lower extremities 1 Recently bedridden >3 days or major surgery within 12 weeks requiring general or regional anesthesia Localized tenderness along the distribution of the deep venous system 1 Entire leg swollen Calf swelling 3 cm larger than asymptomatic side (10 cm below tibial tuberosity) 1 Pitting edema confined to the symptomatic leg 1 Collateral superficial veins (nonvaricose) 1 Alternative diagnosis at least as likely as deep venous thrombosis –2 Note: Clinical probability: low 0; intermediate 1–2; high 3. In patients with symptoms in both legs, the more symptomatic leg is used. Reprinted from The Lancet, Vol 350, Wells PS, Anderson DR, Bormanis J, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management, pp 1795–1798, Copyright 2002, with permission from Elsevier.
 1. Paralysis, paresis, or recent plaster immobilization of the lower extremities 1. Recently bedridden >3 days or major surgery within 12 weeks requiring. general or regional anesthesia 1. Localized tenderness along the distribution of the deep venous system 1. Entire leg swollen 1. Calf swelling 3 cm larger than asymptomatic side (10 cm below tibial tuberosity) 1. Pitting edema confined to the symptomatic leg 1. Collateral superficial veins (nonvaricose) 1. Alternative diagnosis at least as likely as deep venous thrombosis –2. Note: Clinical probability: low 0; intermediate 1–2; high 3. In patients with symptoms in both legs, the more symptomatic leg is used. Reprinted from The Lancet, Vol 350, Wells PS, Anderson DR, Bormanis J, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management, pp 1795–1798, Copyright 2002, with permission from Elsevier.")
16
Adapted from Wells, Thromb Hemost 2000

17
Diagnostic approach

18
Diagnostic approach Assess risk D-dimer Lung Imaging Leg imaging
CT angiography of Chest VQ Scan Leg imaging CT venography Venous doppler US

19
First step Assess risk Wells prediction rule
Validated in number of studies (17 DVT / 3 PE) Induvidual features low predictive value Works best for younger patients without comorbitidies or a history of VTE Clinical judgement should be used in older patients with co-morbidities
 Induvidual features low predictive value. Works best for younger patients without comorbitidies or a history of VTE. Clinical judgement should be used in older patients with co-morbidities.")
20
D-dimer Usefulness depends on number factors When used alone
Sensitivity (must be high or 3rd generation) Other reason for + Any trauma, surgery enough to get blood to clot will elevate D-dimer Probability of disease When used alone In patient’s with comorbidity, older age, longer duration of symptoms in low to moderate risk Only 40 – 50% specificities
 Other reason for + Any trauma, surgery enough to get blood to clot will elevate D-dimer. Probability of disease. When used alone. In patient’s with comorbidity, older age, longer duration of symptoms in low to moderate risk. Only 40 – 50% specificities.")
21
Wells + D-dimer If you have a patient with low pretest probability of DVT / PE and a HIGH – sensitivity D-dimer is negative 0.5% incidence of in 3 months of DVT No need for further imaging If you have a patient with mod to high pretest probability of DVT / PE and a HIGH – sensitivity D-dimer is negative 3.5% and 21.4% DVT risk within 3 months Further imaging needed

22
Leg Ultrasound performance depends on symptoms
NO SYMPTOMS Proximal DVT positive test rules in negative test DOESN’T rule-out sensitivity 60% specificity 90-95% SYMPTOMS PRESENT Proximal DVT positive test rules in negative test rules out sensitivity 90-95% specificity 95% Distal DVT negative test DOESN’T rule out sensitivity 60%; specificity 90-95%

23
PIOPED II CT Angio chest CT Angio chest + CT Venography Sn 83% Sp 96%

24
Prevalence of PE by CT Angio Results and Wells Score
High Interm. Low Total CT + 99% 89% 38% 86% CT - 39% 7% 0.5% 5% PIOPED II NEJM 06

25
Controversy Are the next generation multidetector CTs better
To what level does the study see clots (segmental, subsegmental?) What should come first Leg doppler vs CTA? In a patient with a high pretest probability for PE Is CTA sufficiently sensitive?
 What should come first. Leg doppler vs CTA In a patient with a high pretest probability for PE. Is CTA sufficiently sensitive")
26
Treating medical and surgical patients at high risk of developing DVT
VTE Prophylaxis Treating medical and surgical patients at high risk of developing DVT

27
VTE Prophylaxis - non pharmacological
Mobilization If possible Graduated compression stockings (GCS) TEDS Intermittent pneumatic compression (IPC) For surgical patients
 TEDS. Intermittent pneumatic compression (IPC) For surgical patients.")
28
VTE Prophylaxis - Rx Low dose unfractionated heparin (LDUH)
5000 u sc q12h or q8h Low molecular weight heparin intermediate dose (LMWH) Enoxaparin 30 mg bid or 40 mg od Dalteparin 5000 u od Fondaparinux 2.5 mg sc od
 Enoxaparin 30 mg bid or 40 mg od. Dalteparin 5000 u od. Fondaparinux 2.5 mg sc od.")
29
VTE Treatment

30
VTE Treatment - Rx High dose unfractionated heparin (UFH)
IV Titrated drip Low molecular weight heparin treatment dose (LMWH) Enoxaparin Tinzaparin Dalteparin and others Fondaparinux Coumadin (INR 2 – 3) With at least 4-5 days of heparin Direct thrombin inhibitors For patients with HIT (done via hematology)
 Enoxaparin. Tinzaparin. Dalteparin and others. Fondaparinux. Coumadin (INR 2 – 3) With at least 4-5 days of heparin. Direct thrombin inhibitors. For patients with HIT (done via hematology)")
31
VTE Treatment Heparin vs LMWH Safety and efficacy Multiple studies
LMWH superior for treatment Less mortality and major bleeding Magnitude not very large LMWH at least as effective as UFH

32
VTE Treatment Outpatient vs Inpatient Treatment Number of studies
Likely that LMWH at home is as least as safe as inpatient treatment for DVT In appropriately chosen patients with required supports in place

33
VTE Treatment duration
If OR is only RF - reversible Recommeded duration 3 months If ongoing RF At least 6 months For ongoing malignancy LMWH (CLOT trial)
")
34
IVC Filters Limited evidence: no RCTs
Retrievable filters are available Can be removed up to 6 weeks Recent case series: 91% retrievable Risk of migration Can be adjunctives in patients with existing recent DVT in which anticoagulation contraindicated

Similar presentations



 The Patient Journey>")














 Prophylaxis Policy Mary-Anne Davies Patient Safety Specialist Accreditation Coordinator.>")

 IPC/GCS or, UFH 5000 SQ q 12 hrs or, Enoxaparin 40mg SQ daily IPC/GCS or, UFH 5000.>")
