Download presentation
Presentation is loading. Please wait.

2
Introduction: AP is a common diagnosis. > 240,000/year reported annually in US. Gallstone, the most common cause, 50%. The outcome depends on the severity of the disease. Most patients present with mild disease & benign course & recover quickly with conservative therapy. Severe pancreatitis associated with clinically significant complications develops in a subgroup of patients. To predict the severity & assist in triage (admission to ward or to ICU), several systems used like Ranson criteria. Because of the relatively low prevalence of severe disease, the clinical predictors have a low positive predictive value (43 - 49%) for the development of organ failure or serious complications.
, several systems used like Ranson criteria. Because of the relatively low prevalence of severe disease, the clinical predictors have a low positive predictive value ( %) for the development of organ failure or serious complications..")
3
Epidemiology: Mortality is 5% among all patients& 20 -30% among those with severe cases, although declining. Patients with progressive multisystem organ dysfunction are at highest risk for death, > 50%. Deaths within the first 2 weeks usually due to the systemic inflammatory response syndrome&multisystem organ failure, Deaths that occur later are typically attributable to complications of necrotizing pancreatitis.

4
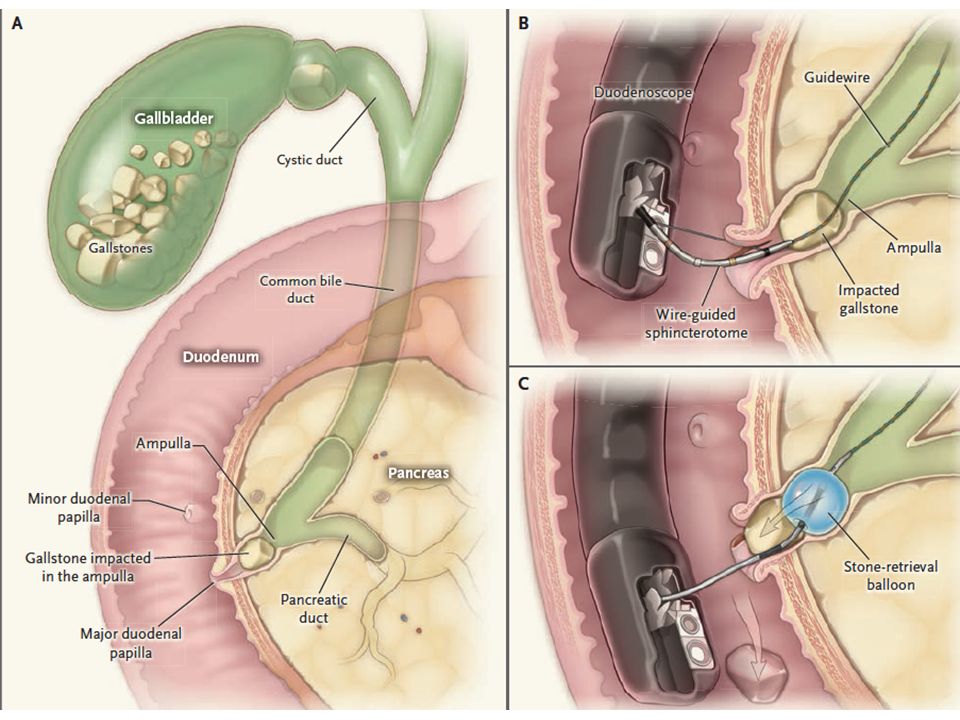
Pathophysiology: Gallstone may compress the septum between the distal biliary & pancreatic ducts, or common channel (ampulla of Vater), resulting in obstruction of the pancreatic duct & increased pressure in the pancreatic duct, resulting in reflux of bile into the pancreatic duct The sequelae of pancreatic-duct obstruction (reflux of pancreatic &biliary secretions, pancreatic-duct hypertension, aberrant secretion of acinar cells) result in pancreatic-duct injury, with the release of pancreatic enzymes into the glandular interstitium causing pancreatic autodigestion triggering acute pancreatitis. Acute ductal obstruction is important, since not all patients with chronic pancreatitis &obstructed pancreatic duct &few patients with pancreatic cancer develop AP.

5
Pathophysiology:evidences At least 50% are due to the passage of small stones, 5 mm or less. Gallstones recovered in stool from 85-95% of patients with acute pancreatitis, compared with a 10% among patients who have symptomatic cholelithiasis without pancreatitis. A high prevalence of bile-duct stones & impacted ampullary stones (63 - 78%) in patients who underwent surgery within 48 hours after admission to the hospital. Early ERCP with biliary sphincterotomy & removal of the obstructing stone might ameliorate the course of pancreatitis.
 in patients who underwent surgery within 48 hours after admission to the hospital. Early ERCP with biliary sphincterotomy & removal of the obstructing stone might ameliorate the course of pancreatitis..")
6
Clinical evidence: The consensus is that in the absence of cholangitis& biliary obstruction, performance of early ERCP (within 24-72 hours after admission to the hospital) does not lead to a reduction in mortality or in local or systemic complications. The results are not dependent on the predicted severity of pancreatitis. Data provide support for the performance of ERCP in patients with biliary obstruction or cholangitis.

7
Clinical use: Most patients with biliary pancreatitis, regardless of the predicted severity, do not benefit from ERCP, with or without sphincterotomy Indications: ERCP indicated within 24- 48 hours after presentation in patients with acute disease & symptoms or signs of coexisting cholangitis (e.g., fever, jaundice, sepsis) or persistent biliary obstruction (a conjugated bilirubin>5 mg/ deciliter ERCP considered in patients who have clinical deterioration (e.g., worsening pain, leukocytosis, a change in vital signs) & increasing liver-enzyme levels if radiologic imaging such as abdominal U/S or CT shows a stone in the CBD.
 or persistent biliary obstruction (a conjugated bilirubin>5 mg/ deciliter ERCP considered in patients who have clinical deterioration (e.g., worsening pain, leukocytosis, a change in vital signs) & increasing liver-enzyme levels if radiologic imaging such as abdominal U/S or CT shows a stone in the CBD.")
8
Contraindications: Absolute contraindication: Conditions that precludes safe moderate sedation. Relative contraindications: Altered postsurgical anatomical features that prevent endoscopic access to the major papilla Clinically significant coagulopathy; INR 75000.

10
Before the procedure: Vitamin K given when there cholangitis or significant obstruction. IVF > 250 ml /hour for at least the initial 24 hours after admission Nothing by mouth; if enteral feeding has been used, it should be discontinued well in advance of the procedure (i.e., 6 - 8 hours before hand). Patients with biliary obstruction require antibiotic prophylaxis before ERCP; quinolone or cephalosporin.
. Patients with biliary obstruction require antibiotic prophylaxis before ERCP; quinolone or cephalosporin..")
11
Complications: Pancreatitis is the most common complication after ERCP, 2 - 8% among low-risk patients, such as those with uncomplicated choledocholithiasis. Bleeding(typically after sphincterotomy) Ductal or intestinal perforation Infection Cardiopulmonary events. When sphincterotomy is not performed, bleeding/ periampullary perforations should not occur. Perforations of the pancreatic duct, the bile duct, or both with wire as well as intestinal perforations due to trauma from the duodenoscope or another instrument (particularly in patients with anatomical alterations after surgery) can occur without a sphincterotomy. ? Increased incidence of respiratory failure in the ERCP.
 Ductal or intestinal perforation Infection Cardiopulmonary events. When sphincterotomy is not performed, bleeding/ periampullary perforations should not occur. Perforations of the pancreatic duct, the bile duct, or both with wire as well as intestinal perforations due to trauma from the duodenoscope or another instrument (particularly in patients with anatomical alterations after surgery) can occur without a sphincterotomy. Increased incidence of respiratory failure in the ERCP..")
12
Uncertainty areas: Biliary pancreatitis without jaundice, both EUS & MRCP are highly accurate in predicting persistent choledocholithiasis& allow for more appropriate use of ERCP& increasingly favored approach is to perform EUS followed by ERCP (while the patient is under the same sedation) only if bile-duct stones are detected. ? These imaging may obviate the need for intraoperative cholangiography during a subsequent cholecystectomy. ? Whether all with GSs & biliary pancreatitis should undergo elective cholecystectomy after a biliary sphincterotomy. We recommend lapchole in patients who are able to undergo surgery after clearance of the bile duct. If ERCP &sphincterotomy are not performed during the initial episode of pancreatitis, surgery should be performed once the acute symptoms have resolved. An intraoperative cholangiogram should be obtained during cholecystectomy, particularly if a preoperative sphincterotomy has not been performed.

13
Uncertainty areas: ? Perform ERCP in a patient who presents with acute biliary pancreatitis after cholecystectomy. If the patient continues to have abdominal pain& persistently elevated levels of liver enzymes, despite apparent resolution of the pancreatitis, proceeding directly to ERCP is reasonable. If the patient has recovered from the episode of pancreatitis with substantial improvement in (or normalization of) liver-enzyme levels, we perform an evaluation with either MRCP or EUS & proceed to ERCP only if choledocholithiasis is identified.
 liver-enzyme levels, we perform an evaluation with either MRCP or EUS & proceed to ERCP only if choledocholithiasis is identified..")
14
Guidelines : UK Guidelines, 2005, support early ERCP (within 72 hours after admission) in all patients with predicted or actual severe biliary pancreatitis. Subsequent studies have shown a benefit only in patients with coexisting cholangitis. In 2007 AGA: the role of routine ERCP in severe biliary pancreatitis remains controversial. Urgent ERCP (within 24 hours) was recommended, however, in patients with cholangitis& early ERCP (within 72 hours) was recommended if suspicion of persistent bile-duct stones remained high. Recent ACG guidelines suggest that urgent ERCP (within 24 hours) is indicated in patients with biliary pancreatitis who have concurrent acute cholangitis, but it is not needed in most patients who do not have evidence of ongoing biliary obstruction.
 was recommended, however, in patients with cholangitis& early ERCP (within 72 hours) was recommended if suspicion of persistent bile-duct stones remained high. Recent ACG guidelines suggest that urgent ERCP (within 24 hours) is indicated in patients with biliary pancreatitis who have concurrent acute cholangitis, but it is not needed in most patients who do not have evidence of ongoing biliary obstruction..")
15
Case management : A 74-yearold man presenting with acute pancreatitis. The combination of a ALT of 295 U/ liter ( * 7 times normal)& cholelithiasis on abd U/S is highly suggestive of a biliary cause. The clinical picture presented is not suggestive of coexisting ascending cholangitis or biliary obstruction (i.e., TSB normal/ CBD normal in diameter). This patient should be treated conservatively (not routinely proceed with early ERCP within 72 hours after admission) with aggressive IVF, IV analgesics, antiemetics. ERCP would be considered if the patient’s clinical condition deteriorated, particularly if he had increasing levels of serum liver enzymes& a biliary sphincterotomy would be performed if a stone in the CBD was identified. To reduce the risk of future biliary events, we would recommend cholecystectomy during this same hospital stay if the patient was not at high surgical risk once his pancreatitis resolved.
& cholelithiasis on abd U/S is highly suggestive of a biliary cause. The clinical picture presented is not suggestive of coexisting ascending cholangitis or biliary obstruction (i.e., TSB normal/ CBD normal in diameter). This patient should be treated conservatively (not routinely proceed with early ERCP within 72 hours after admission) with aggressive IVF, IV analgesics, antiemetics. ERCP would be considered if the patient’s clinical condition deteriorated, particularly if he had increasing levels of serum liver enzymes& a biliary sphincterotomy would be performed if a stone in the CBD was identified. To reduce the risk of future biliary events, we would recommend cholecystectomy during this same hospital stay if the patient was not at high surgical risk once his pancreatitis resolved..")
18
BO5s: 1 The positive predictive value of clinical predictors for organ failure & serous complications of acute pancreatitis is: A. Low. B.High. C. Medium. D. Very High. E. Very low.

19
BO5s: 1 The positive predictive value of clinical predictors for organ failure & serous complications of acute pancreatitis is: A. Low. B. High. C. Medium. D. Very High. E. Very low.

20
BO5s: 2 Multi-organ failure in acute pancreatitis usually occur : A. After the first month. B. In the first 2 week. C. After the 1st 2 weeks. D. After the 1 st 2 months. E. None of the above.

21
BO5s: 2 Multi-organ failure in acute pancreatitis usually occur : A. After the first month. B. In the first 2 week. C. After the 1st 2 weeks. D. After the 1 st 2 months. E. None of the above.

22
BO5s: 3 The definite indication for ERCP in gall stone pancreatitis is: A. Evidence of biliary obstruction or cholangitis. B. Evidence of biliary obstruction or cholangitis C. High clinical predicted severity.. D. All of the above. E. None of the above.

23
BO5s: 3 The definite indication for ERCP in gall stone pancreatitis is: A. Evidence of biliary obstruction and cholangitis. B. Evidence of biliary obstruction or cholangitis. C. High clinical predicted severity.. D. All of the above. E. None of the above.

24
BO5s: 4 Indication for ERCP in gall stone pancreatitis include all except: A. Evidence of biliary obstruction. B. Evidence cholangitis. C. Clinical deterioration. D. Increasing liver enzymes. E. Severe pancreatitis.

25
BO5s: 4 Indication for ERCP in gall stone pancreatitis include all except: A. Evidence of biliary obstruction. B. Evidence cholangitis. C. Clinical deterioration. D. Increasing liver enzymes. E. Severe pancreatitis.

26
BO5s: 5 The ideal time of performing indicated ERCP in gall stone pancreatitis is within: A. 3 days. B. 3 weeks. C. 3 months. D. First few hours. E. None of the above.

27
BO5s: 5 The ideal time of performing indicated ERCP in gall stone pancreatitis is within: A. 3 days. B. 3 weeks. C. 3 months. D. First few hours. E. None of the above.

Similar presentations







>")




![GI Endoscopy ~ BASIC ~ ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS IN CHILDREN [LECTURE] EOSINOPHILIC.](/20/5943603/big_thumb.jpg "GI Endoscopy ~ BASIC ~ ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS IN CHILDREN [LECTURE] EOSINOPHILIC.>")








