Download presentation
Presentation is loading. Please wait.

1
BIOE 301 Lung Cancer Warning: I have determined that cigarette smoke is dangerous to your health.

2
Lung Cancer: 2005 174,470 new cases in US, 2006
accounts for 13% of new cancer cases 162,460 deaths in US, 2006 and 29% of all cancer deaths each year in US Signs and Symptoms symptoms of lung cancer can take many years to develop which often leads to diagnosis at an advanced stage of this disease. Increase in volume of sputum Wheezing Change in color of sputum Blood in sputum Repeated episodes of pneumonia or bronchitis

3
Lung Cancer Risk Factors: -Smokers vs. Non-smokers
#1 Tobacco Use. -90% of lung cancer cases in men and 78% of lung cancer cases in women are caused by smoking tobacco. -Smokers vs. Non-smokers A smokers risk for developing lung cancer is 20 to 30 times greater than a non smoker Second Hand Smoke -Second hand (passive) tobacco smoke is carcinogenic and may increase the lung cancer risk by 20%. Radon Exposure -Radon is an invisible gas that occurs naturally in rock and soil. About 10% of lung cancer cases are due to excessive radon exposure. Asbestos Exposure Asbestos is a fibrous mineral used in many industries. Exposure increases ones risk of developing lung cancer by 3-4 times.
 tobacco smoke is carcinogenic and may increase the lung cancer risk by 20%. Radon Exposure. -Radon is an invisible gas that occurs naturally in rock and soil. About 10% of lung cancer cases are due to excessive radon exposure. Asbestos Exposure. Asbestos is a fibrous mineral used in many industries. Exposure increases ones risk of developing lung cancer by 3-4 times.")
4
Tobacco Use in the US, 1900-2000 Per capita cigarette consumption
Male lung cancer death rate Male lung cancer death rate Female lung cancer death rate The last set of slides describes at the prevalence of cancer risk factors, such as tobacco use and physical inactivity, and the prevalence of cancer screening, such as use of mammography. Tobacco use is a major preventable cause of death, particularly from lung cancer. The year 2004 marks the anniversary of the release of the first Surgeon General’s report on Tobacco and Health, which initiated a decline of per capita cigarette smoking in the United States. As a result of the cigarette smoking epidemic, lung cancer death rates showed a steady increase through 1990, then began to decline. The lung cancer death rate among US women, who began regular cigarette smoking later than men, has continued to increase, but at a slower rate since the early 1990s. *Age-adjusted to 2000 US standard population Source: Death rates: US Mortality Public Use Tapes, , US Mortality Volumes, , National Center for Health Statistics, Centers for Disease Control and Prevention, Cigarette consumption: US Department of Agriculture,

5
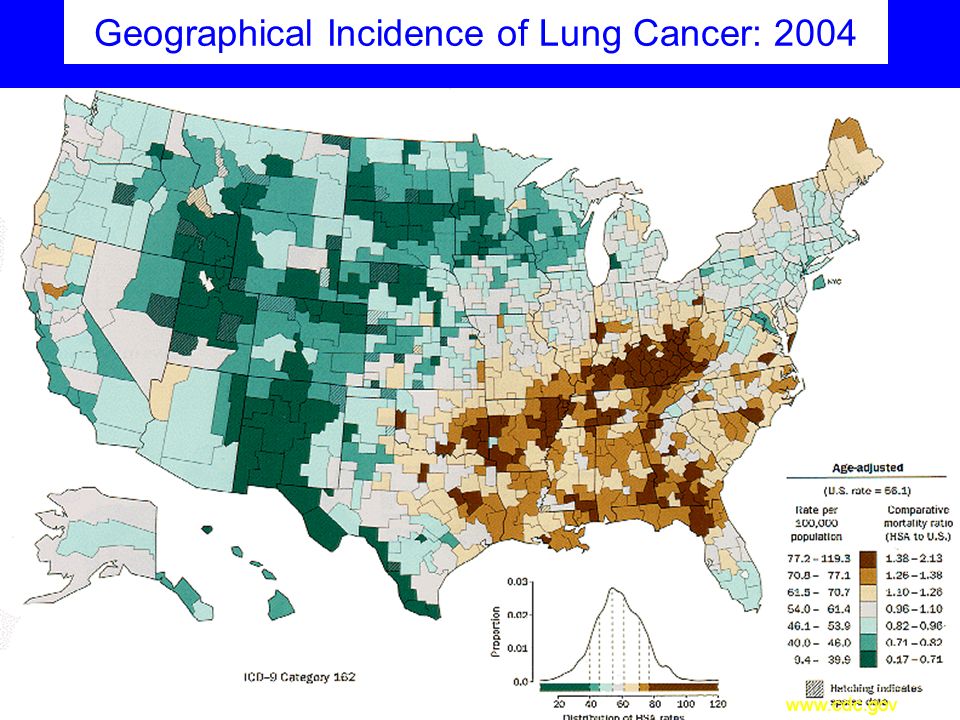
Geographical Incidence of Lung Cancer: 2004
6
Incidence & Mortality

7
Lung Cancer Around the World
Incidence: Lung cancer is the most common cancer worldwide, accounting for 1.2 million new cases annually Lung cancer accounts for 17.8% of all cancer deaths Half of all cases (49.9%) occur in the developing world The estimated numbers of lung cancer cases worldwide has increased by 51% since 1985 Highest incidence in: North America Europe (esp. Eastern Europe) Mortality: Most common cause of death from cancer, with 1.18 million deaths worldwide
 occur in the developing world. The estimated numbers of lung cancer cases. worldwide has increased by 51% since Highest incidence in: North America. Europe (esp. Eastern Europe) Mortality: Most common cause of death from cancer, with 1.18 million deaths worldwide.")
8
Lung Cancer Around the World
American Cancer Society Cancer Atlas Cancer Risks for Boys Cancer Risks for Girls Lung Cancer Around the World The above links take you to pdf’s from the American Cancer Society’s Cancer Atlas.Use the magnification tool to zoom in on different parts of the document. Cancer Risks for Boys: Upper Half: World map displays, country by country, the percentage of 15year old boys that smoke cigarettes. Lower Right: Bar chart displays the percentage of year old boys, in select African countries, that use other, non-cigarette tobacco products. Cancer risks for Girls: Upper Half: World map displays, country by country, the percentage of 15 year old girls that smoke cigarettes. Lower Right: Bar chart displays the percentage of year old girls in select African countries that use other, non-cigarette tobacco products. Lung Cancer Around the World: Upper Left: Chart displays the trends in lung cancer mortality for men and women in three countries: Spain, Hungry, and US. Trends in lung cancer mortality closely follow trends in tobacco usage for the given country. Lower Left: Chart displays trends in lung cancer mortality. Note that these have remained relatively constant over the last 30 years. The key to reducing lung cancer lies in prevention. Right Half: World maps display the incidence of lung cancer for men and women, country by country.

9
Incidence: Male v. Female
World Wide Incidence of Lung Cancer: Men vs. Women

10
A little Background: The Lungs

11
Initiation of Cellular Changes
Injurious inhalant Carcinogen Squamous Metaplasia Increasingly severe atypia Cancer in situ Normal Epithelium Persistent Squamous Metaplasia Squamous metaplasia is non-specific response to injury to the bronchiole epithelium. It does not always progress to carcinoma. Invasive Carcinoma

12
Progression of tissue changes leading to cancer
Normal epithelium of the bronchi Cellular Changes: Thickening of the epithelium =hyperplasia Loss of the ciliated columnar cells which are replaced by a squamous epithelium Proliferation of basal cells = dysplasia Development of abnormal cell structure and abnormal nuclei

13
Surface view: normal lung
Cross-section: normal lung Cross-section: cancerous lung Cross-section: normal lung Surface view: normal lung Surface view: normal lung Surface view: cancerous lung

14
Your CONFIDENTIAL Test Results have arrived….
Lung Cancer Screening Your CONFIDENTIAL Test Results have arrived….

15
Your CONFIDENTIAL Test Results
You can open now, or you can wait and learn more… Possible Outcome Cancer Diagnosis Automatic 100% on Exam 2 True Positive: You have cancer and the test correctly identified your condition. You will receive treatment. Lose 10 points on Exam 2 False Negative: You have cancer, but the test did not identify your condition. You will not receive treatment. Lose 1 point on Exam 2 False Positive: You do not have cancer, but the test says you do. You will undergo unnecessary, painful tests. No effect on Exam 2 score True Negative: You do not have cancer and the test correctly identified that you do not have cancer,

16
Who Should be Screened? According to the American Cancer Society, February 2006, no organization recommends screening for lung cancer in asymptomatic individuals. WHY? Inadequate evidence to determine whether or not screening truly reduces mortality.

17
Potential Risks of Screening
Knowing that you have cancer may not improve your health or help you live longer. False Negative Results False Positive Results Side effects of screening process (exposure to radiation) The following explanations are provided by the National Cancer Institute as to the potential risks of screening (bullet points above) Finding lung cancer may not improve health or help you live longer. Screening may not improve your health or help you live longer if you have advanced lung cancer or if it has already spread to other places in your body. Some cancers never cause symptoms or become life-threatening, but if found by a screening test, the cancer may be treated. It is not known if treatment of these cancers would help you live longer than if no treatment were given, and treatments for cancer may have serious side effects. False-negative test results can occur. Screening test results may appear to be normal even though lung cancer is present. A person who receives a false-negative test result (one that shows there is no cancer when there really is) may delay seeking medical care even if there are symptoms. False-positive test results can occur. Screening test results may appear to be abnormal even though no cancer is present. A false-positive test result (one that shows there is cancer when there really isn't) can cause anxiety and is usually followed by more tests (such as biopsy), which also have risks. A biopsy to diagnose lung cancer can cause part of the lung to collapse. Sometimes surgery is needed to reinflate the lung. Chest x-rays expose the chest to radiation. Radiation exposure from chest x-rays may increase the risk of developing certain cancers, such as breast cancer. Source:
 The following explanations are provided by the National Cancer Institute as to the potential risks of screening (bullet points above) Finding lung cancer may not improve health or help you live longer. Screening may not improve your health or help you live longer if you have advanced lung cancer or if it has already spread to other places in your body. Some cancers never cause symptoms or become life-threatening, but if found by a screening test, the cancer may be treated. It is not known if treatment of these cancers would help you live longer than if no treatment were given, and treatments for cancer may have serious side effects. False-negative test results can occur. Screening test results may appear to be normal even though lung cancer is present. A person who receives a false-negative test result (one that shows there is no cancer when there really is) may delay seeking medical care even if there are symptoms. False-positive test results can occur. Screening test results may appear to be abnormal even though no cancer is present. A false-positive test result (one that shows there is cancer when there really isn t) can cause anxiety and is usually followed by more tests (such as biopsy), which also have risks. A biopsy to diagnose lung cancer can cause part of the lung to collapse. Sometimes surgery is needed to reinflate the lung. Chest x-rays expose the chest to radiation. Radiation exposure from chest x-rays may increase the risk of developing certain cancers, such as breast cancer. Source:")
18
Lung Cancer: Screening
2 Methods Available: Chest X-Ray Spiral CT

19
What are X-Rays??? X-Rays are a type of electromagnetic radiation
Both chest x-ray and spiral CT rely on same basic principle. Shorter Wavelengths, Higher Energy Longer Wavelengths, Lower Energy Electromagnetic waves are made up of discrete particles called photons

20
How Are X-Rays Produced?
X-Ray Tube Electrons produced at cathode accelerate towards anode. Electrons interact with Tungsten atoms producing X-rays via two modes of interaction: -Bremsstrahlung -Characteristic Radiation Anode Cathode electrons X-Rays are produced in the x-ray tube (animation above). The x-ray tube contains an anode (flat blue piece) made of a metal called Tungsten that is attached to the positive terminal of the power supply. The cathode (yellow coil) is attached to the negative terminal of the power supply. When the coil (cathode) is energized, it emits negatively charged electrons that accelerate across the voltage potential towards the positively charged anode (also called a target). As the electrons slam into the target, they interact with the Tungsten atoms. These interactions produce x-rays in two ways. The first, and most common interaction, is called Bremsstrahlung (German for “braking radiation”). In Bremsstrahlung, the travelling electrons slow down and change direction as they near the nucleus of the tungsten atom. The change in kinetic energy before and after interacting with the nucleus is released as an x-ray photon. The second methods by which x-rays are produced is called characteristic radiation. Characteristic radiation is produced when a traveling electron displaces an electron from one of the electron shells surrounding the tungsten atom. When a tungsten electron of higher energy “drops down” into the lower energy shell, an x-ray photon is produced. This is called characteristic radiation because the energy of the x-ray is characteristic to the specific atom and shell.
. The x-ray tube contains an anode (flat blue piece) made of a metal called Tungsten that is attached to the positive terminal of the power supply. The cathode (yellow coil) is attached to the negative terminal of the power supply. When the coil (cathode) is energized, it emits negatively charged electrons that accelerate across the voltage potential towards the positively charged anode (also called a target). As the electrons slam into the target, they interact with the Tungsten atoms. These interactions produce x-rays in two ways. The first, and most common interaction, is called Bremsstrahlung (German for braking radiation ). In Bremsstrahlung, the travelling electrons slow down and change direction as they near the nucleus of the tungsten atom. The change in kinetic energy before and after interacting with the nucleus is released as an x-ray photon. The second methods by which x-rays are produced is called characteristic radiation. Characteristic radiation is produced when a traveling electron displaces an electron from one of the electron shells surrounding the tungsten atom. When a tungsten electron of higher energy drops down into the lower energy shell, an x-ray photon is produced. This is called characteristic radiation because the energy of the x-ray is characteristic to the specific atom and shell.")
21
How are X-Ray Images Produced?
X-Rays interact with the bone, tissues, and air in the body. These interactions cause a decrease in X-Ray energy called “attenuation.” The amount of X-Ray attenuation is related to the density of the material. Mass Attenuation Coefficients (μ/ρ) Dry Air cm2/g Lung Tissue cm2/g Bone cm2/g Values taken at X-Ray energy of 100keV: energy level typical of chest x-rays X-Rays produced by the x-ray tube enter the body where they interact with bone, air (lungs and digestive tract), and various tissues. Because these materials have different densities, they will attenuate (absorb) x-rays to a varying degree. The mass attenuation coefficient is a measure of how much the tissues will (or will not) attenuate the x-rays in units of cm^2/g. Increasing attenuation Source:
 Dry Air cm2/g. Lung Tissue cm2/g. Bone cm2/g. Values taken at X-Ray energy of 100keV: energy level typical of chest x-rays. X-Rays produced by the x-ray tube enter the body where they interact with bone, air (lungs and digestive tract), and various tissues. Because these materials have different densities, they will attenuate (absorb) x-rays to a varying degree. The mass attenuation coefficient is a measure of how much the tissues will (or will not) attenuate the x-rays in units of cm^2/g. Increasing attenuation. Source:")
22
How are Chest X-Ray Images Produced?
tumor Patient The diagram to the left shows the arrangement of the x-ray tube, patient, grid, and film. Looking at the chest x-ray on the right, the dark regions are areas of low attenuation (air in the lungs). A greater number of x-rays reach the film causing it to be exposed. The white or light regions of the film correspond to areas of higher attenuation (bones, tissues). Because fewer x-rays reach the film, these areas are not exposed. As X-rays pass through the patient, some are deflected causing “scatter”. Scatter is not desirable, as it is essentially false information that will clutter the image. The grid is made up of lead strips that help prevent the x-rays from reaching the film. Diagram of X-Ray Imaging Setup Image: Chest X-Ray
. A greater number of x-rays reach the film causing it to be exposed. The white or light regions of the film correspond to areas of higher attenuation (bones, tissues). Because fewer x-rays reach the film, these areas are not exposed. As X-rays pass through the patient, some are deflected causing scatter . Scatter is not desirable, as it is essentially false information that will clutter the image. The grid is made up of lead strips that help prevent the x-rays from reaching the film. pageid=48. Diagram of X-Ray Imaging Setup. Image: Chest X-Ray.")
23
Setup of the Chest X-Ray

24
Limitations of Chest X-Rays
Details of soft tissues are hard to resolve Some structures (cancers) are too small to be detected. Subject to human interpretation (and error).
 are too small to be detected. Subject to human interpretation (and error).")
25
A New Kind of X-Ray: Low Dose CT (LDCT)
LDCT (Low Dose Computed Tomography also called Spiral CT) relies on the same basic principles described for the chest x-ray above. Instead of one x-ray tube and detector, it has several that rotate around the patient. The “spiral” comes from the fact that the patient is moved through the center of the machine as the x-rays tubes and detectors rotate around them. A computer is used to reconstruct the images from the various angles to create a cross sectional image like the one shown above.
 relies on the same basic principles described for the chest x-ray above. Instead of one x-ray tube and detector, it has several that rotate around the patient. The spiral comes from the fact that the patient is moved through the center of the machine as the x-rays tubes and detectors rotate around them. A computer is used to reconstruct the images from the various angles to create a cross sectional image like the one shown above. image=chest-ct-lungs.jpg&&pg=chestct.")
26
Limitations of LDCT Scans
Motion can lessen the quality of the image Requires patient to hold their breath for 20 seconds. Improved soft tissue detail over conventional X-Ray, but still not great.

27
Is CT Screening Cost Effective?
Some scenarios…. Annually screen 100,000, 60 yr. old smokers -1 QALY costs $116,300 2) Annually screen 100, yr. old smokers in the process of quitting. -1 QALY costs $558,600 3) Annually screen 100,000, 60 yr. old former smokers (quit in last 5 years) -1 QALY costs $2.3 million! Source: “Little Value Seen in CT Scans For Lung Cancer Screening.” Science Daily. Jan. 15, Accessed 07/25/06. Available: daily.com/release/2003/01/
 Annually screen 100, yr. old smokers in the process of quitting. -1 QALY costs $558,600. 3) Annually screen 100,000, 60 yr. old former smokers (quit in last 5 years) -1 QALY costs $2.3 million! Source: Little Value Seen in CT Scans For Lung Cancer Screening. Science Daily. Jan. 15, Accessed 07/25/06. Available: daily.com/release/2003/01/")
28
How does a chest X-ray compare to a LDCT?
National Cancer Institute Randomized Controlled Trial: The Lung Screening Study 3318 Participants 30 pack-year history 1 Pack a day for the last 30 years, 2 packs a day for last 15 years, 3 packs a day for last 7.5 years, etc... Participants randomized to receive either a LDCT scan or a Chest X-Ray. In short, we don’t really know yet. The lung screening study was a short term feasibility study for a much larger trial (50,000 participants over 8 years). It provided a base line of numbers comparing the two screening methods, but does not offer any information regarding whether or not screening improves lung cancer mortality rates. Gohagan,J. Marcus,P. Fagerstrom,R. Pinsky,P. Kramer,B. and Prorok P. Baseline findings of a randomized feasability trial of lung cancer screening with spiral CT scan vs chest radiograph: the lung screening study of the National Cancer Institute Chest.126:
. It provided a base line of numbers comparing the two screening methods, but does not offer any information regarding whether or not screening improves lung cancer mortality rates. Gohagan,J. Marcus,P. Fagerstrom,R. Pinsky,P. Kramer,B. and Prorok P. Baseline findings of a randomized feasability trial of lung cancer screening with spiral CT scan vs chest radiograph: the lung screening study of the National Cancer Institute Chest.126:")
29
Study Results: CXR vs. LDCT
# of Participants 1550 1586 # of positive screens 152 (9.8%) 325 (20.5%) # of people with positive screens that had an additional invasive procedure 15 (10%) 55 (17%) # diagnosed with cancer 7 (0.45% of total) 30 (1.9% of total) # of false positives 145 (9%) 295 (19%)
 325 (20.5%) # of people with positive screens that had an additional invasive procedure. 15 (10%) 55 (17%) # diagnosed with cancer. 7 (0.45% of total) 30 (1.9% of total) # of false positives. 145 (9%) 295 (19%)")
30
Ongoing Trials National Cancer Institute: National Lung Screening Trial 50,000 participants (former and heavy smokers) 8 years long (scheduled to end in 2009) Compare risks and benefits of standard chest x-ray to LDCT Should Produce more definitive screening recommendations Local Connection: MD Anderson is one of 30 hospitals participating in this trial. The Lung Screening Study was not designed to establish whether or not CXR or LDCT screening reduces lung cancer mortality.
 Compare risks and benefits of standard chest x-ray to LDCT. Should Produce more definitive screening recommendations. Local Connection: MD Anderson is one of 30 hospitals participating in this trial. The Lung Screening Study was not designed to establish whether or not CXR or LDCT screening reduces lung cancer mortality.")
31
Your CONFIDENTIAL Test Results
Second Chance, do you want to choose to be screened?

Similar presentations











. Approximately.>")







