Download presentation
Presentation is loading. Please wait.

1
ENFECTIVE ENDOCARDITIS M.RASOOLINEJAD, MD DEPARTMENT OF INFECTIOUS DISEASE TEHRAN UNIVERSITY OF MEDICAL SCIENCE

2
INFECTIVE ENDOCARDITIS Infection of the endocardial surface

4
INFECTIVE ENDOCADITIS

7
INTRUDUCTION Clinical manifestations are so varied.Clinical manifestations are so varied. All of medical subspecialist must encounterAll of medical subspecialist must encounter Successful management Medical & Surgical.Successful management Medical & Surgical.

8
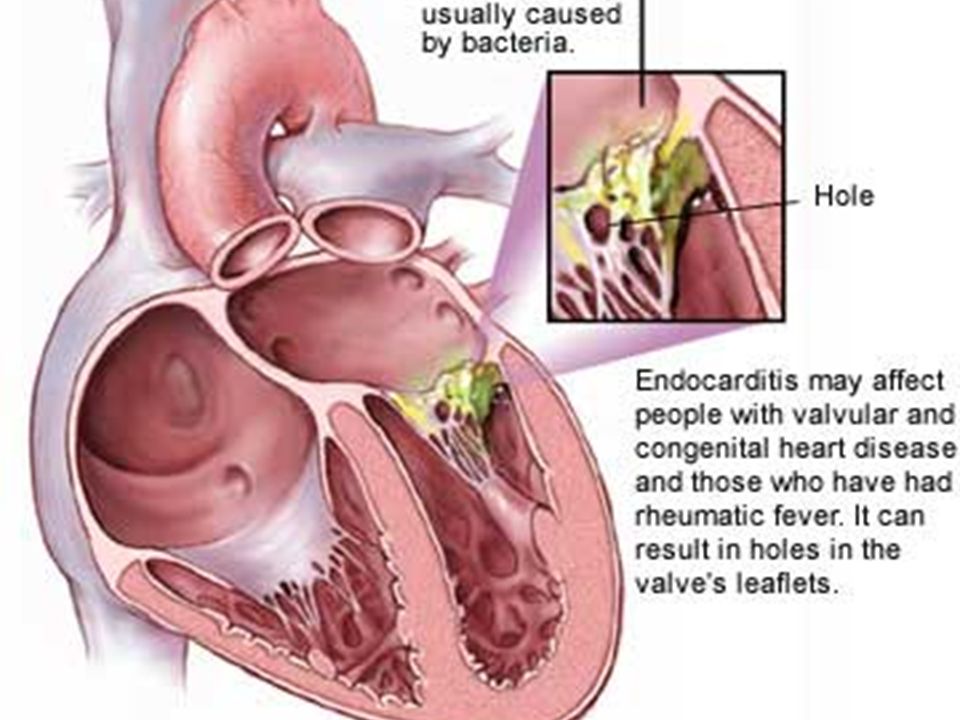
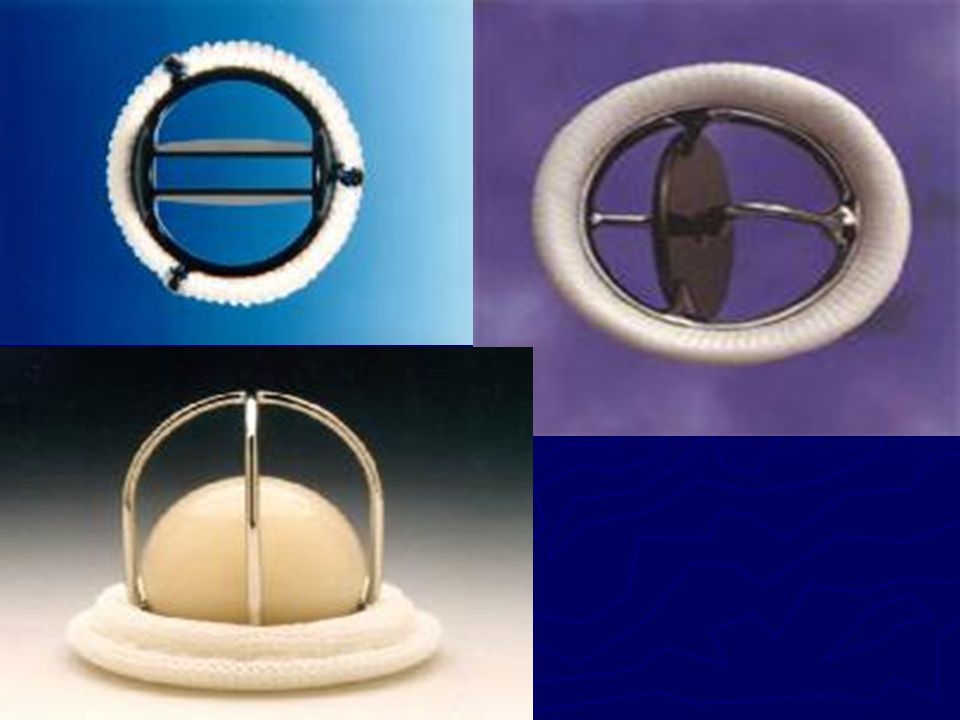
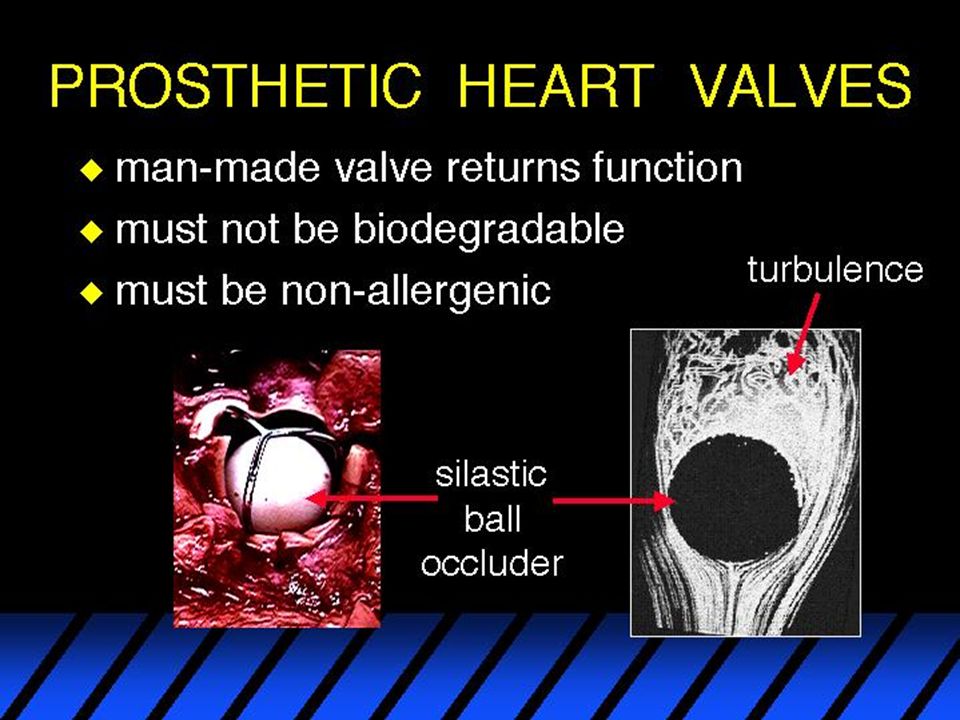
EPIDEMIOLOGY 20% of cases are categorized as definite Mean age of patients are increased Underlying heart disease Rheumatic heart disease Rheumatic heart disease Degenerative heart disease Degenerative heart disease Congenital heart disease Congenital heart disease Nosocomial endocarditis Nosocomial endocarditis Intracardiac prostheses Intracardiac prostheses Injection Drug Users ( IDU ) Injection Drug Users ( IDU )
 Injection Drug Users ( IDU )")
9
Endothelium Mucus membrane (Trauma, Turbulance, or (Trauma, Turbulance, or metabolic change ) Colonized tissue metabolic change ) Colonized tissue Plt - fib deposition Trauma Plt - fib deposition Trauma NBTE Bacteremia NBTE Bacteremia Adherence Adherence Colonization Colonization Mature Vegetation Mature Vegetation PATHOGENESIS Local factor Bacteriocins IgA protease Bacterial adherence Complement Antibody
 Colonized tissue metabolic change ) Colonized tissue Plt - fib deposition Trauma Plt - fib deposition Trauma NBTE Bacteremia NBTE Bacteremia Adherence Adherence Colonization Colonization Mature Vegetation Mature Vegetation PATHOGENESIS Local factor Bacteriocins IgA protease Bacterial adherence Complement Antibody")
10
PATHOGENESIS Nonbacterial Thrombotic Endocarditis (NBTA) Hemodynamic factor Transient Bacteremia Microorganisms Immunopathologic
 Hemodynamic factor Transient Bacteremia Microorganisms Immunopathologic")
11
ETIOLOGIC AGENTS Streptococci ( viridance, Fecalis,… ) 60 – 80 % Staphylococci ( +ve Or -ve coagolase ) 20 – 30 % Gram -ve bacteria 1.5 – 13% Fungi 2 - 4 % Culture negative 5 – 25 % Others 1 – 2 %
 60 – 80 % Staphylococci ( +ve Or -ve coagolase ) 20 – 30 % Gram -ve bacteria 1.5 – 13% Fungi % Culture negative 5 – 25 % Others 1 – 2 %")
12
CULTURE – NEGATIVE ENDOCARDITIS Subacute right – side infective endocarditis Chronic course > 3 months Uremia supervening chronic course Mural IE as in VSD Pacemaker wires infection

13
CULTURE - NEGATIVE ENDOCARDITIS HACEK* Brucella spp, Prior administration of antibiotics Rickettsiae, Chlamydia, Virus Noninfective endocarditis * Haemophilus spp, Actinobacillus spp, Cardiobacterium spp, Eikenella, Kingella

14
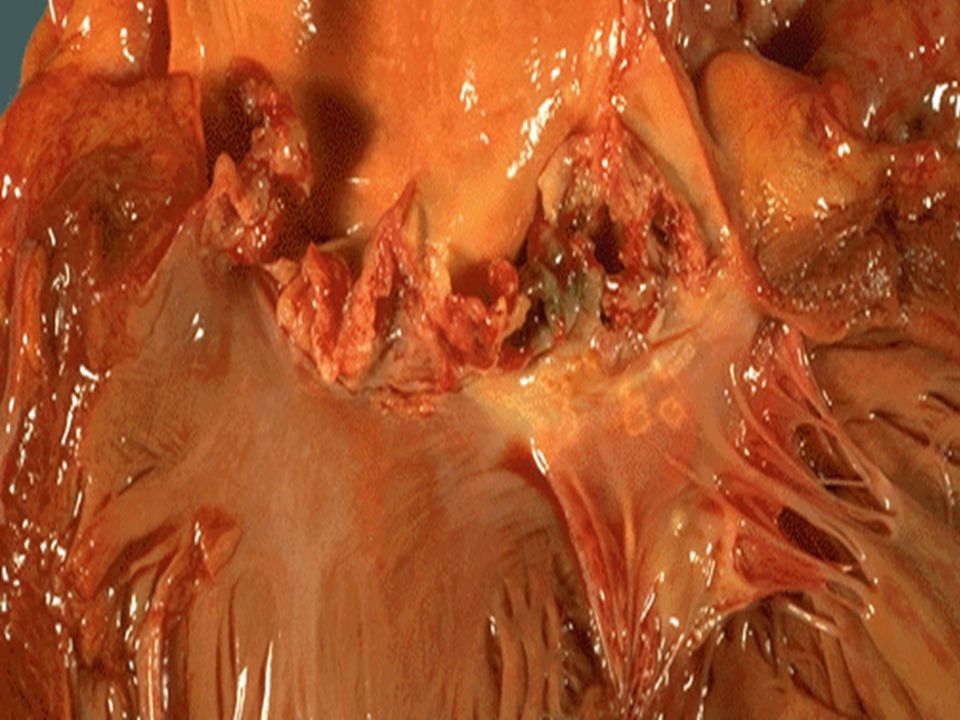
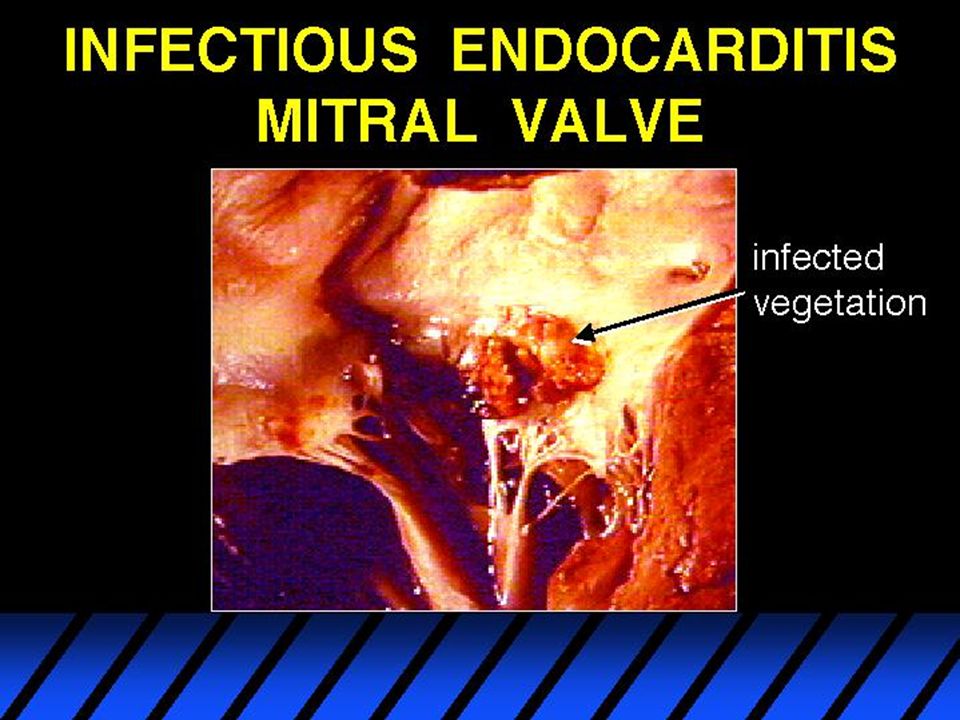
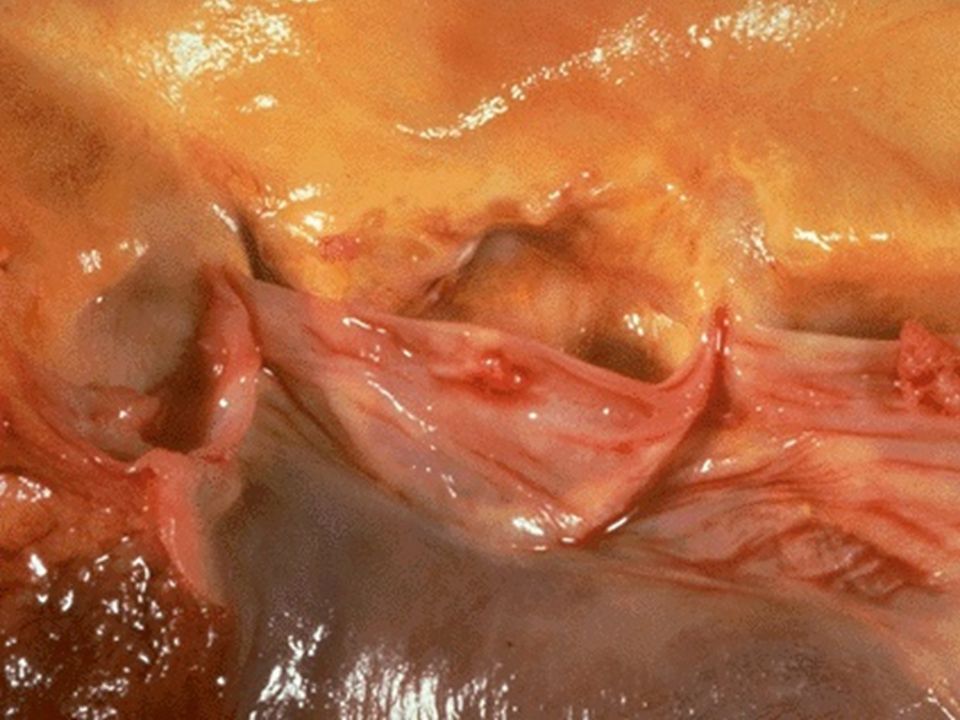
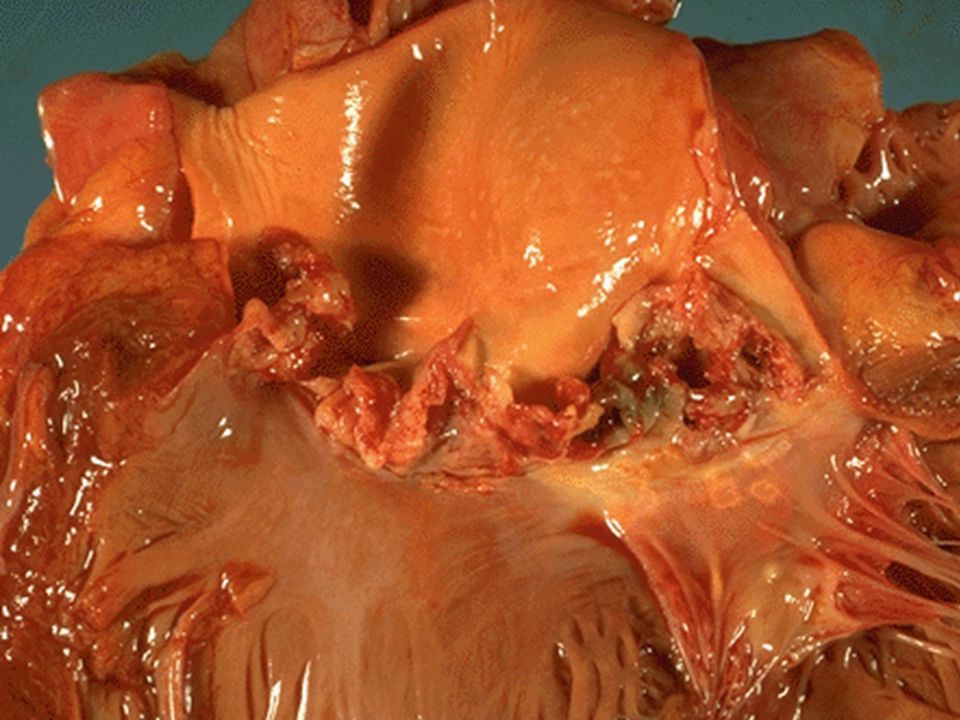
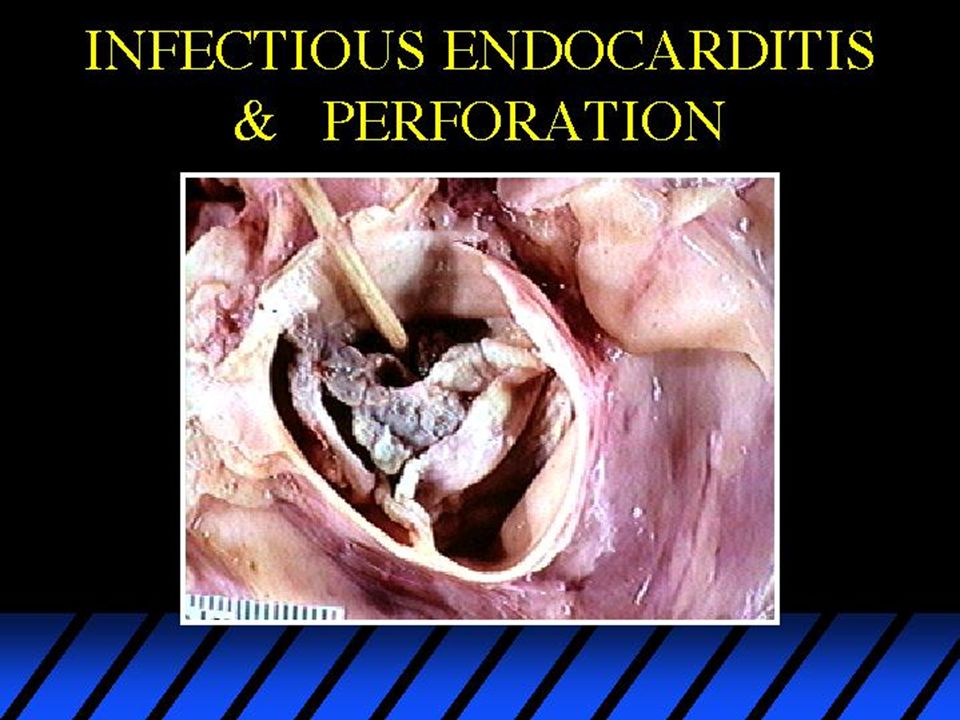
PATHOLOGY HEART: Vegetation ( fibrin, Plt, bacteria, PMN, RBC ) Valve change perforation. Rupture of chordae tendinae, septum and papillary muscle Ring abscess Valvular stenosis Valvular regurgitation Myocardial abscess Pericarditis, effusions Coronary emboli

15
PATHOLOGY RENAL Renal architecture is abnormal in all cases, Even in the absence of clinical or biochemical of renal disease

16
PATHOLOGY RENAL Focal glomerulonephritis Diffuse glomeruonephritis Membranoproliferative glomerulonephritis Renal infarction Renal abscess

17
PATHOLOGYCNS Emboli (middle cerebral artery ) Infarction Arteritis Abscess Mycotic aneurysms Hemorrhage: Intracerebral or Subarachnoid Encephalomalacia Meningitis
 Infarction Arteritis Abscess Mycotic aneurysms Hemorrhage: Intracerebral or Subarachnoid Encephalomalacia Meningitis")
18
PATHOLOGY MYCOTIC ANEURYSMS Usually during active IE Occasionally mons or years after successful treatment Direct bacterial invasion abscess Septic embolic to vasa vasorum Immun complex deposition Cerebral vessels, abdominal aorta, sinus of Valsalva Clinically silent until rupture

19
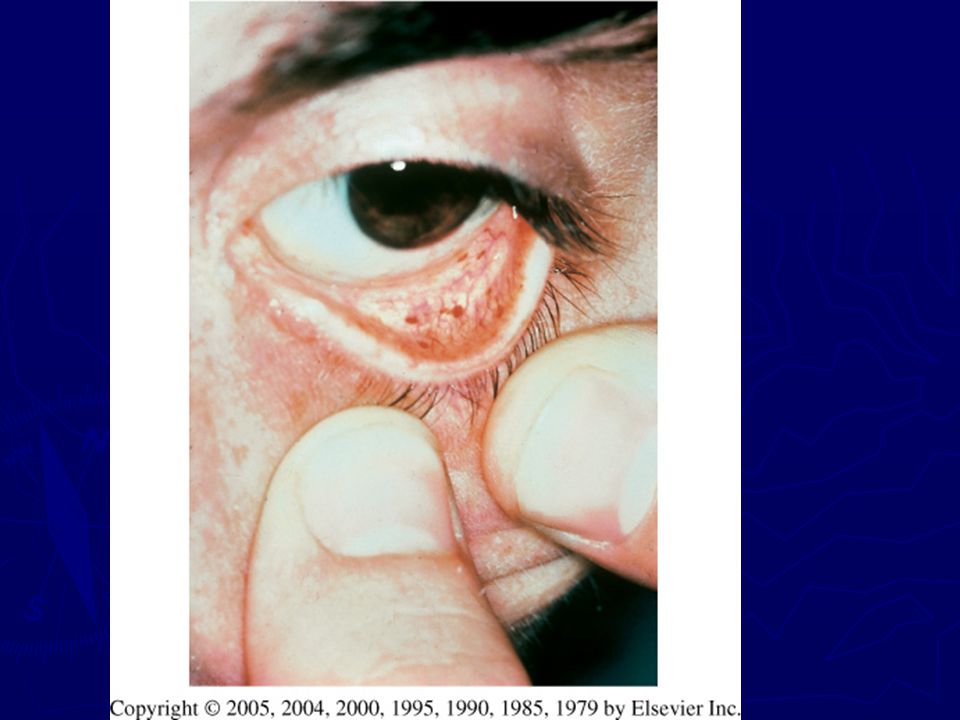
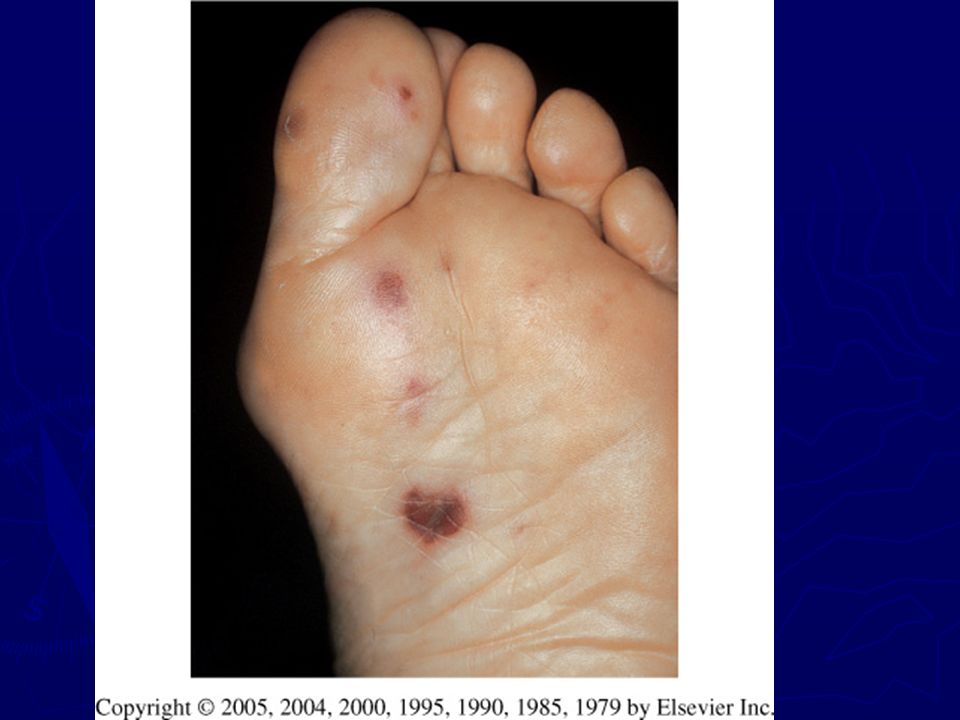
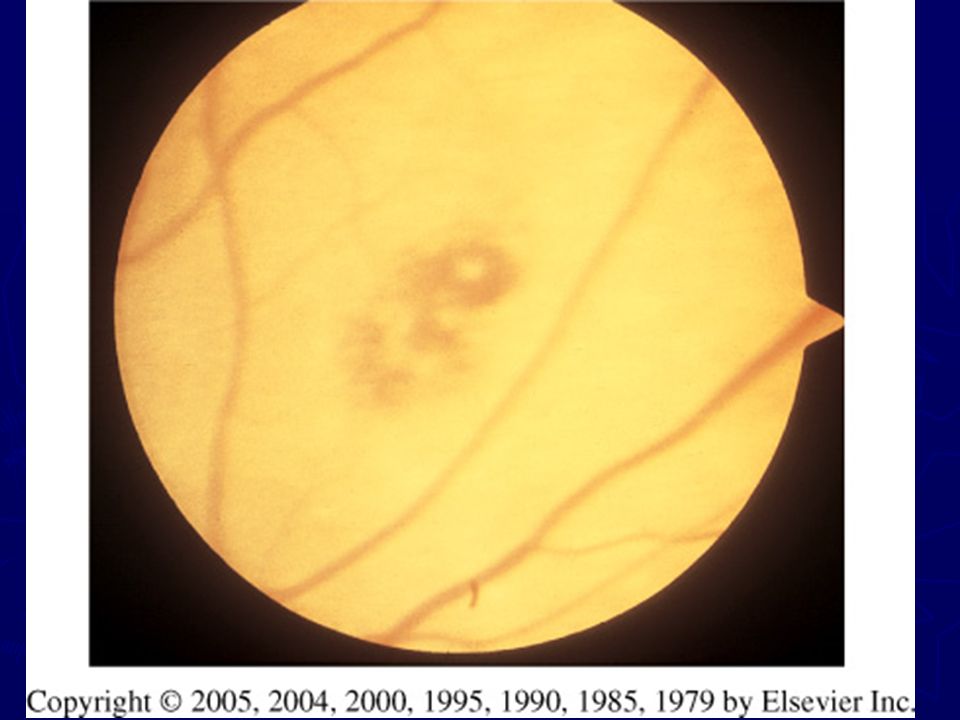
PATHOLOGY SPLEEN: LUNG: SKIN: EYE: Infarction, Abscess, Enlargement Emboli, Acute Pneumonia, Pleural Effusion Ptechiae, Osler node ( Arteriolar intimal proliferation ) Janeway lesions ( Becteria, Necrosis, PMN, Hemorrhage Janeway lesions ( Becteria, Necrosis, PMN, Hemorrhage) Roth spots ( Lymphocyte, Edema, Hemorrhage Roth spots ( Lymphocyte, Edema, Hemorrhage )
 Janeway lesions ( Becteria, Necrosis, PMN, Hemorrhage Janeway lesions ( Becteria, Necrosis, PMN, Hemorrhage) Roth spots ( Lymphocyte, Edema, Hemorrhage Roth spots ( Lymphocyte, Edema, Hemorrhage )")
20
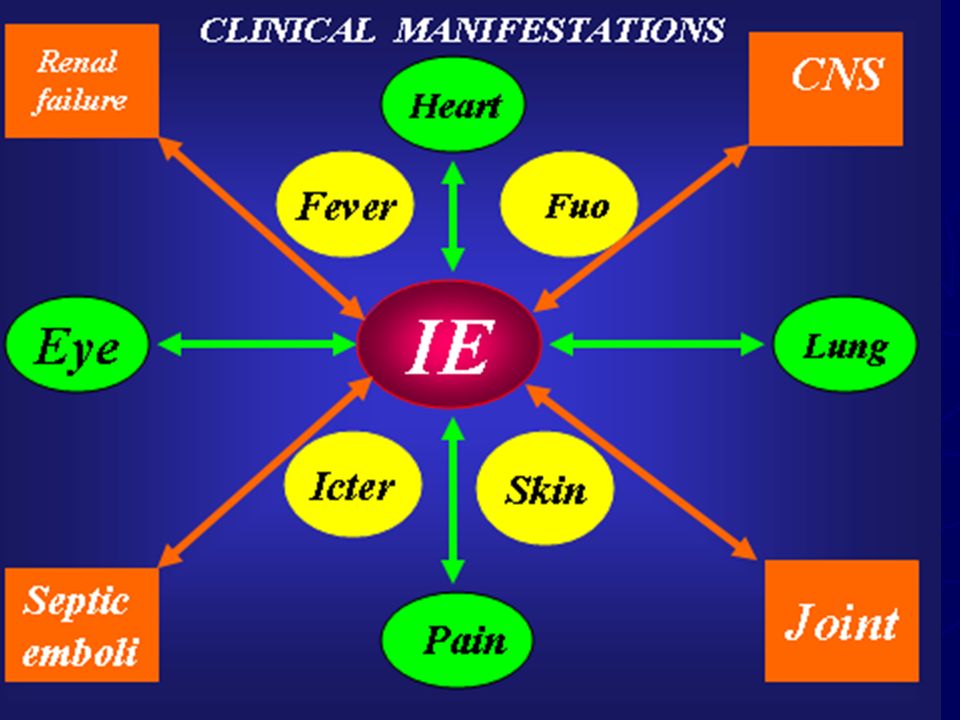
IE CNS KIDNEY LUNG HEART FEVER EYESKIN FUO ICTER SEPTICEMBOLI PAIN JOINTCLINICALMANIFESTATION

31
IE & IDU More common in cocain users Febrile IDU = IE No underlying heart disease More common in tricuspid valve Aortic > Aortic + Mitral > Mitral valve Pumonary septic emboli S aureous, P aueroginosa IDU & HIV / AIDS

32
IE & ELDERLY Increased incidence in elderly Prolonged survival with CVD, PHV in elderly, Intravascular monitoring devises, Surgical implant material. No specific symptoms & sings Strep faecalis & bovis are common. Diagnosis may be difficult. Prompt empirical therapy : Vancomycin + Gentamycin Cardiac complications : CHF, Conduction abnormality, Arrhythmias, Myocarditis, Myocardial abscess.

33
LAB FINDING Anemia ( normochromic, normocytic, Fe, IBC ) Thrombocytopenia ( 5 – 15 % ) Leucocyte count ( or or ) Large mononuclear cells ( histiocyte ) ESR ( mean 57 mm/hr ) Hypergammaglobulinemia Positive RF ( 40 – 50 % ) Complement ( 5 – 15 % ) Positive VDRL & positive CIC U/A ( protein,RBC, WBC ) Positive blood culture & Positive ECHO Serology & Teichoic acids antibody
 Thrombocytopenia ( 5 – 15 % ) Leucocyte count ( or or ) Large mononuclear cells ( histiocyte ) ESR ( mean 57 mm/hr ) Hypergammaglobulinemia Positive RF ( 40 – 50 % ) Complement ( 5 – 15 % ) Positive VDRL & positive CIC U/A ( protein,RBC, WBC ) Positive blood culture & Positive ECHO Serology & Teichoic acids antibody")
34
DIAGNOSIS Durack DT, Lukes AS, Bright DK, Criteria Definite ( Pathologic & Clinical Criteria ) Possible Rejected CLINICAL CRITERIA 2 2Major or 1 1Major & 3 Minor or 5 Minor
 Possible Rejected CLINICAL CRITERIA 2 2Major or 1 1Major & 3 Minor or 5 Minor")
35
MAJOR CRITERIA Positive blood culture Evidence of endocardial involvement MINOR CRITERIA Predisposing heart disease or IDU Fever > 38 Vascular phenomena Immunologic phenomena ECHO Microbiologic evidence

36
POSITIVE BLOOD CULTURE Typical microorganisms: ( S. viridance, S. bovis, HACEK, Entrococci, S. aureous in the absence of primary focus) Persistently positive blood cultures ( B/Cs drown more than 12 hr apart, or All of 3 or majority of 4 separate B/Cs with 1 st & last drawn at least 1 hr apart ) HACEK: Haemophilus spp, Actinobacillus spp, Cardiobacterium homonis, Ekinella corrodence Kingella kingae
 Persistently positive blood cultures ( B/Cs drown more than 12 hr apart, or All of 3 or majority of 4 separate B/Cs with 1 st & last drawn at least 1 hr apart ) HACEK: Haemophilus spp, Actinobacillus spp, Cardiobacterium homonis, Ekinella corrodence Kingella kingae.")
37
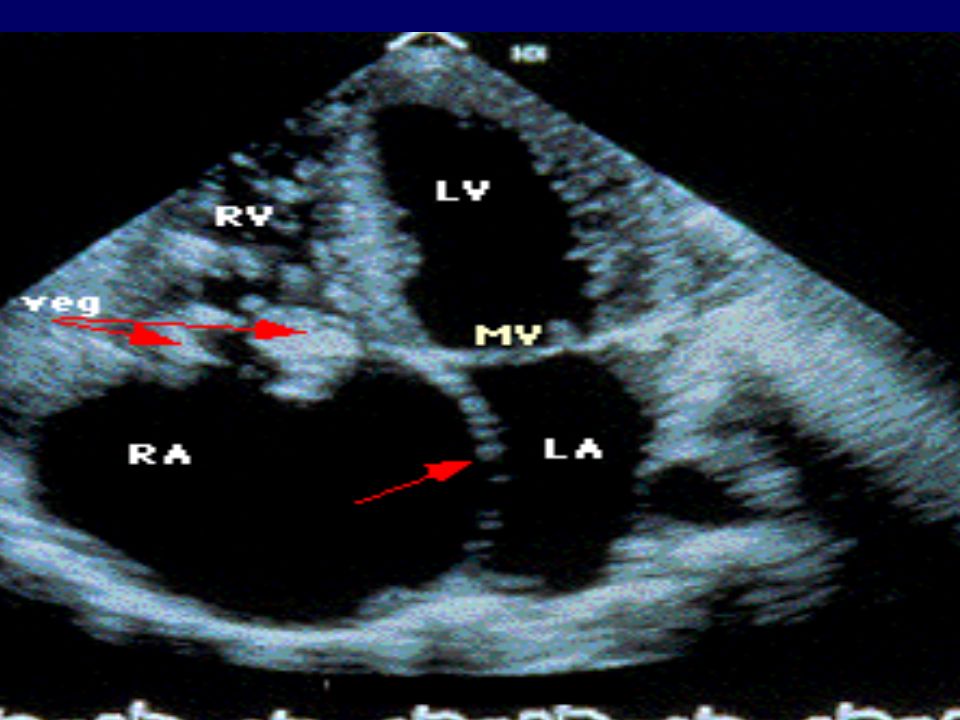
EVIDENCE OF ENDOCARDIAL INVOLVEMENT Positive ECHO for IE New valvular regurgitation Oscillating intracardiac mass Abscess New dehiscence of prosthetic valve

40
veg

41
Mitral valve Vegetation

42
Mitral valve vegetation

43
TREATMENT Antimicrobial therapy High dose, prolonged & IV antibiotics High dose, prolonged & IV antibiotics Surgical therapy ANTIMICROBIAL THERAPY Empirical therapy Organisms based therapy Duration of treatment

44
MONITORING ANTIMICROBIAL THERAPY Serum concentration of antibioticSerum concentration of antibiotic should be monitoring. should be monitoring. Antibiotic toxicities should be considered.Antibiotic toxicities should be considered. Blood culture should be repeated daily SterileBlood culture should be repeated daily Sterile Rechecked B/C if there is recrudescent fever.Rechecked B/C if there is recrudescent fever. Performed B/C 4 – 6 WKS after therapyPerformed B/C 4 – 6 WKS after therapy to document cure. to document cure.

45
MONITORING ANTIMICROBIAL THERAPY B/C became sterile after start antibiotics:B/C became sterile after start antibiotics: 2 days in S.Viridance 2 days in S.Viridance Enterococci Enterococci HACEK organisms HACEK organisms 3 – 5 days in S. Aureus + beta lactam 3 – 5 days in S. Aureus + beta lactam 7 days in S. Aureus + Vancomycin 7 days in S. Aureus + Vancomycin

46
MONITORING ANTIMICROBIAL THERAPY If fever persist for 7 days in spite appropriate AB Evaluate patient for: appropriate AB Evaluate patient for: Paravalvular abscess Paravalvular abscess Extracardiac abscess Extracardiac abscess Embilic event Embilic event Vegetation became smaller with effective therapy 3 months after cure: 50% unchanged 3 months after cure: 50% unchanged 25% are slightly larger 25% are slightly larger

47
SURGICAL THERAPY Refractory CHF > One serious systemic emboli Uncontrolled infection Valve dysfunction ( ECHO ) Fungal & Brucella endocarditis Mycotic aneurysms Prosthetic valve Local suppurative complications Large vegetation > 1 cm Vegetation size after 4 WKS Aortic valve endocarditis Acute valve insufficiency Recurrent endocarditis
 Fungal & Brucella endocarditis Mycotic aneurysms Prosthetic valve Local suppurative complications Large vegetation > 1 cm Vegetation size after 4 WKS Aortic valve endocarditis Acute valve insufficiency Recurrent endocarditis")
48
INDICATION FOR SURGICAL INTERVENTION Surgery required for optimal outcome Surgery to be strongly considered for improved outcome for improved outcome

49
INDICATION FOR SURGICAL INTERVENTION Surgery required for optimal outcome: * Moderate to severe CHE due to valvular dysfunction. * Moderate to severe CHE due to valvular dysfunction. *Partially dehisced unstable prosthetic valve. *Partially dehisced unstable prosthetic valve. * Persistent bacteremia despite optimal AB therapy. * Persistent bacteremia despite optimal AB therapy. *Lake of effective microbial therapy ( fungal, Brucella…) *Lake of effective microbial therapy ( fungal, Brucella…) *S. Aureus PVIE + intra cardiac complication. *S. Aureus PVIE + intra cardiac complication. *Relapse of PVIE after optimal therapy *Relapse of PVIE after optimal therapy
 *Lake of effective microbial therapy ( fungal, Brucella…) *S. Aureus PVIE + intra cardiac complication. *S. Aureus PVIE + intra cardiac complication. *Relapse of PVIE after optimal therapy *Relapse of PVIE after optimal therapy.")
50
INDICATION FOR SURGICAL INTERVENTION Surgery to be strongly considered for improved outcome: * Peivalvular extension of infection * Peivalvular extension of infection *Poorly responsive S. aureus in aortic or mitral valve. *Poorly responsive S. aureus in aortic or mitral valve. *Large > 10 Cm hypermobile vegetation *Large > 10 Cm hypermobile vegetation *Persistent unexplained fever >10 days in culture -ve IE. *Persistent unexplained fever >10 days in culture -ve IE. *Poorly responsive or relapse ( Entrococci & Gram-ve ) *Poorly responsive or relapse ( Entrococci & Gram-ve )
 *Poorly responsive or relapse ( Entrococci & Gram-ve ).")
52
Valve Ring abscess

53
Intra operation

54
After repair

55
Intraoperative TEE

59
PROPHYLAXIS OF ENDOCADITIS Potential Interventions Alleviation of predisposing condition Alleviation of predisposing condition Immunization against bacteria Immunization against bacteria Inhibition of bacterial adherence Inhibition of bacterial adherence Application of antiseptic in the mouth Application of antiseptic in the mouth Administration of antibiotics Administration of antibiotics

60
Procedure Causing Bacteremia: Oral cavity Respiratory tract Genitourinary tract Gastrointestinal tract Vascular system

61
RISK OF IE WITH CARDIAC DISORDERS HIGH RISK: PHV, PID, Cyanotic CHD, PDA, AS, MR, VSD, Coarctation of aorta INTERMEDIATE RISK Prolapse +MR, MS, TS, TR Bicaspid Aorta, Degenerative Heart Disease LOW / NO RISK Prolapse Mitral, ASD, Aterosclerosic Plaques, CAD, Pacemaker.

62
ANTIBIOTIC PROPHYLAXIS High risk procedures High risk procedures & High risk of cardiac disease High risk of cardiac disease Recommended High risk procedures High risk procedures & Intermediate risk of cardiac disease Intermediate risk of cardiac disease Recommended Low risk procedures Low risk procedures & High risk of cardiac disease High risk of cardiac disease Optional

63
RECOMMENDED REGIMENS Procedures: Dental, upper Res, GI, GU, Implantation of Prosthetic Valve Amoxicillin PO Clindamycin Po Ampicillin + Gentamycin Cefazolin Vancomycin + Gentamycin Before&After

Similar presentations









 The term can also include noninfective endocarditis, in which sterile.>")








 Definition: Rheumatic fever (RF) is an autoimmune disease affecting the heart and extra- cardiac.>")








