Download presentation
Presentation is loading. Please wait.

1
Improving Preventive Health Care Success Stories: USPSTF and ePSS at San Francisco General Hospital AHRQ 2009 Conference Alice Hm Chen, MD, MPH

2
SFGH Acknowledgements Lisa Johnson, Medical Director for Quality Improvement Programs, Community Primary Care Fred Strauss, IS/Provider Liaison Winnie Tse, Analyst, Community Primary Care Flu-FOBT Project: Michael Potter, Professor of Clinical Family and Community Medicine and Albert Yu, Medical Director of Chinatown Public Health Center

3
Outline Background SFGH delivery system and EMR Case study: colorectal cancer screening Case study: breast cancer screening

4
Why focus on preventive care? Only 10% of female Medicare beneficiaries received all of 5 recommended preventive care measures (cervical, breast and colorectal cancer screening; pneumovax and influenza vaccines). Significant disparities in receipt of preventive care services among racial/ethnic groups and poor. General Accounting Office congressional testimony on 3/23/02, available at: www.gao.gov/cgi-bin/getrpt?GAO-02-777T.
. Significant disparities in receipt of preventive care services among racial/ethnic groups and poor. General Accounting Office congressional testimony on 3/23/02, available at: GAO T..")
5
Barriers to Screening in the Safety Net Financial barriers (lack of insurance, co-pays) System resource constraints, e.g. Lack of ability to offer screening colonoscopies Difficulty hiring mammographers Literacy, language, and cultural barriers Conflicting guidelines for PCPs 7.4 hours/day to provide all USPSTF “A” and “B” services Yarnell KS, Pollak KI, Ostbye T, Krause KM, Michener JL. Primary care: Is there enough time for prevention? American Journal of Public Health 2003; 635-641.

6
Whose guidelines should we be following, anyways? Proliferation of guidelines “Eminence” based versus evidence based Internal versus external Ability to tailor to resources Time consuming to develop Need for ongoing updates

7
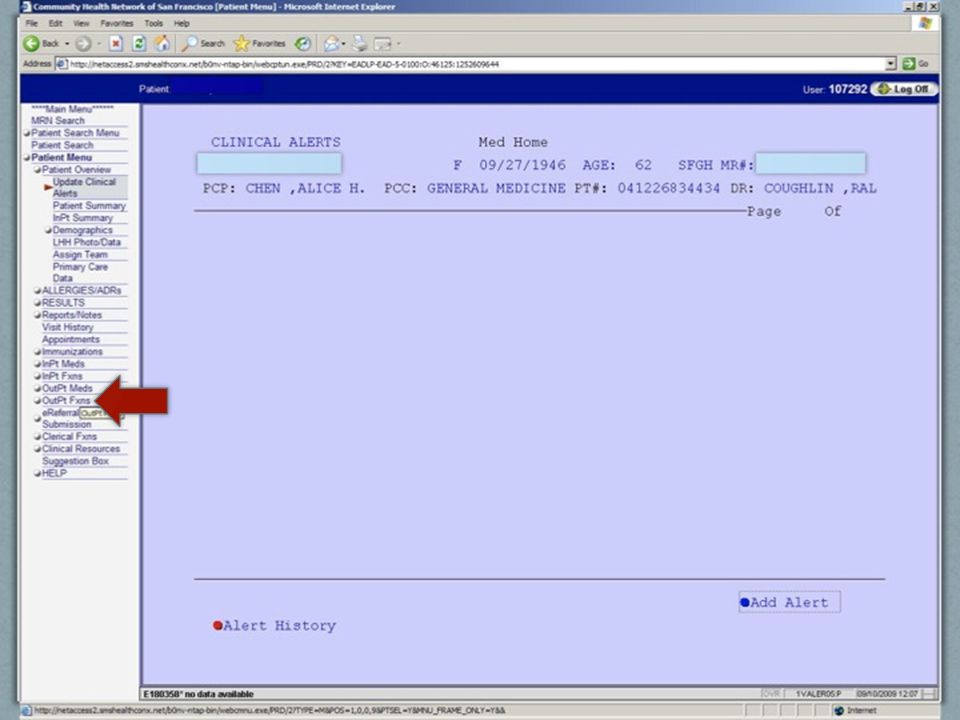
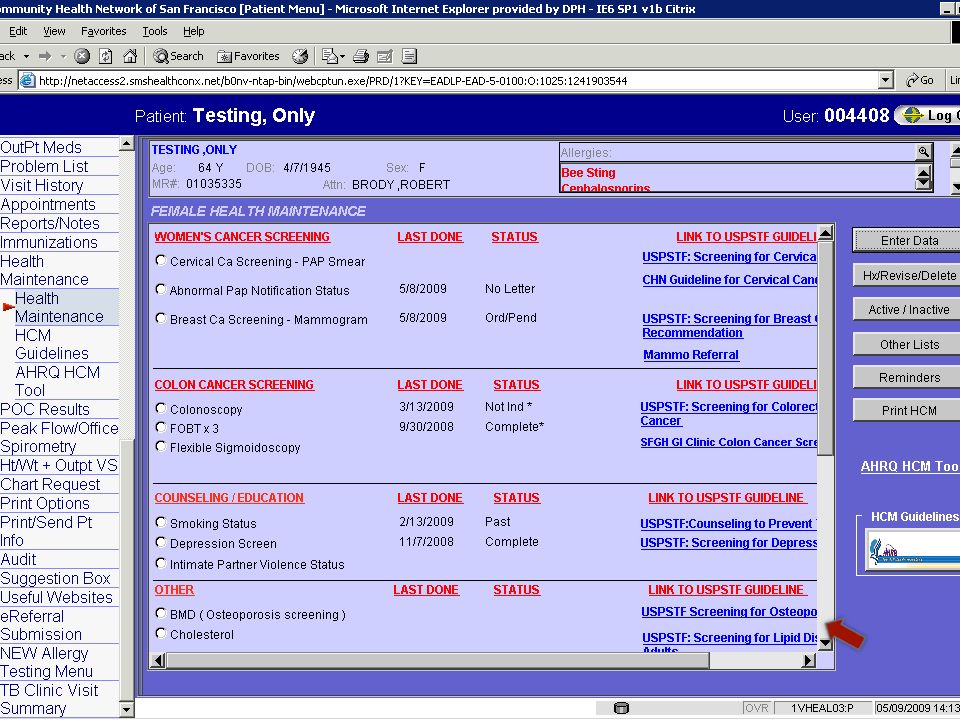
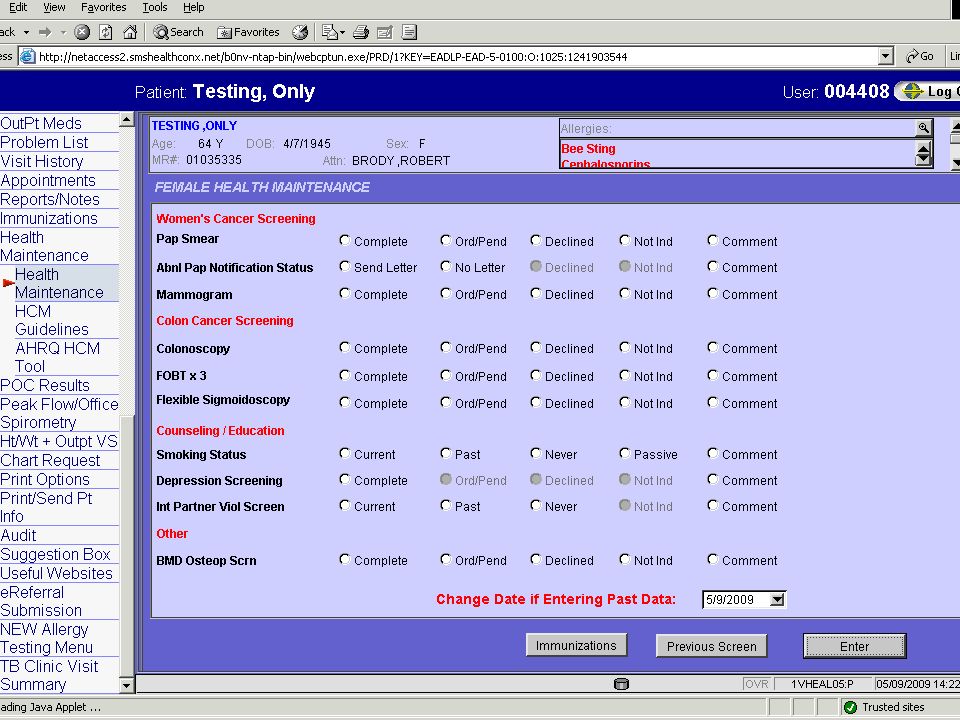
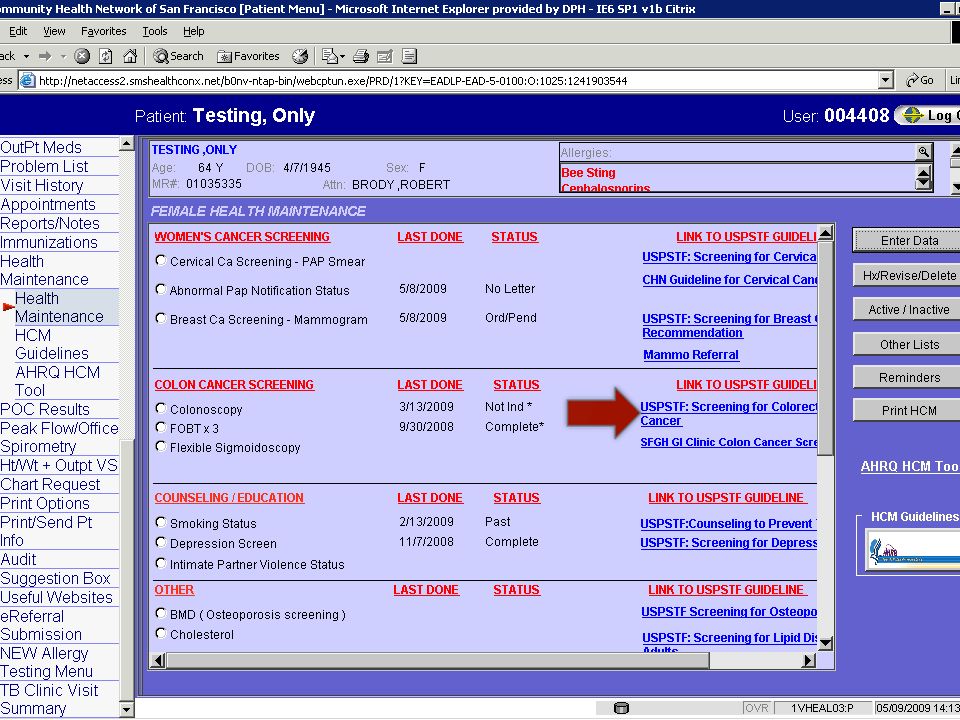
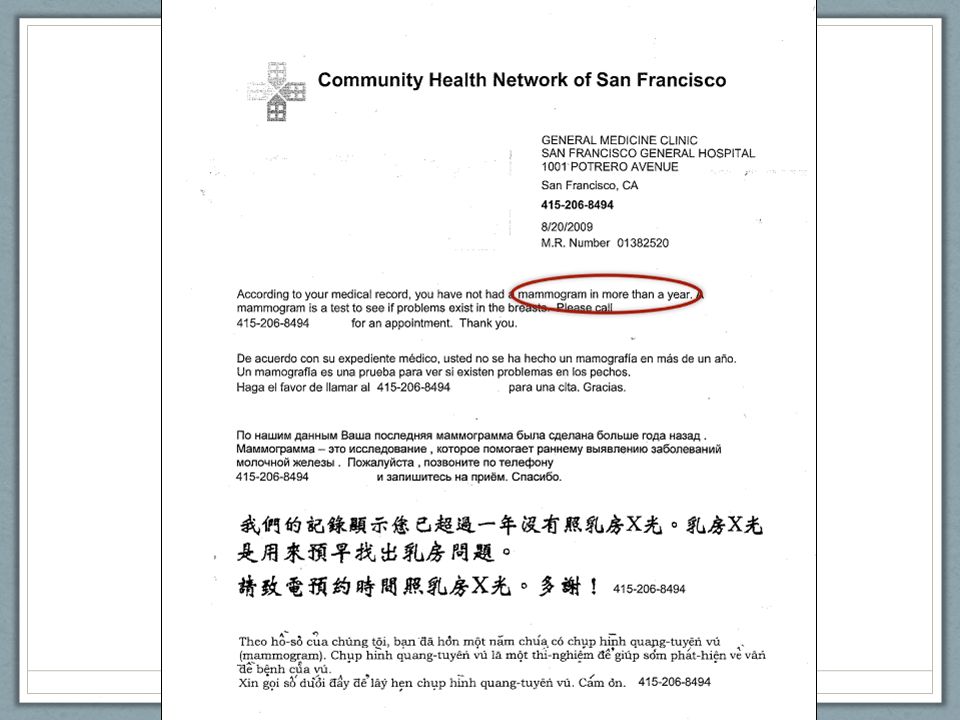
SFGH Approach Agreement on evidence-based guidelines (USPSTF), tailored to our system’s resource constraints Harnessing information technology Electronic medical record AHRQ Electronic Preventive Services Selector (ePSS) Patient registries Systems interventions Standing orders Panel management Culturally and linguistically appropriate outreach
, tailored to our system’s resource constraints Harnessing information technology Electronic medical record AHRQ Electronic Preventive Services Selector (ePSS) Patient registries Systems interventions Standing orders Panel management Culturally and linguistically appropriate outreach")
17
Colorectal Cancer Screening “Success” Practice based on USPSTF guidelines, tailored to system resource constraints (no screening colonoscopy) SF DPH recommends annual home FOBT, with diagnostic colonoscopy for abnormals Systems intervention: Flu-FOBT program Culturally and linguistically appropriate outreach
 SF DPH recommends annual home FOBT, with diagnostic colonoscopy for abnormals Systems intervention: Flu-FOBT program Culturally and linguistically appropriate outreach")
21
Flu-FOBT Program Strategy: offer FOBT in combination with flu shots Initial pilot results Flu only: 52.9% 57.3% eligible completed FOBT Flu + FOBT: 54.5% 84.3% eligible completed FOBT Difference of 25.4 points, p<0.001 Potter MB, Phengrasamy L, Hudes ES, McPhee SJ, Walsh J. Offering annual fecal occult blood tests at annual flu shot clinics increases colorectal cancer screening rates. Annals of Family Medicine 2009; 7:17-23. SF DPH program at Chinatown Public Health Center led by Mike Potter and Albert Yu, funded by CDC Slide courtesy of Albert Yu and Mike Potter

22
Outreach Materials Slide courtesy of Albert Yu and Mike Potter

23
Designed at Request of CPHC Staff with Patient Input

24
CPHC Preliminary Results Efficacy among 50-80 year olds who came in for primary care visit during flu shot season Got Flu Shot Didn’t Get Flu Shot (n=1286)(n=588) Up to date 9-29-0851.2%60.2% Up to date 3-31-0975.2%64.8% Change+25.0%+4.6% Slide courtesy of Albert Yu and Mike Potter
(n=588) Up to date %60.2% Up to date %64.8% Change+25.0%+4.6% Slide courtesy of Albert Yu and Mike Potter")
25
SF DPH Screening Rates U.S average (NHIS 2000)
")
26
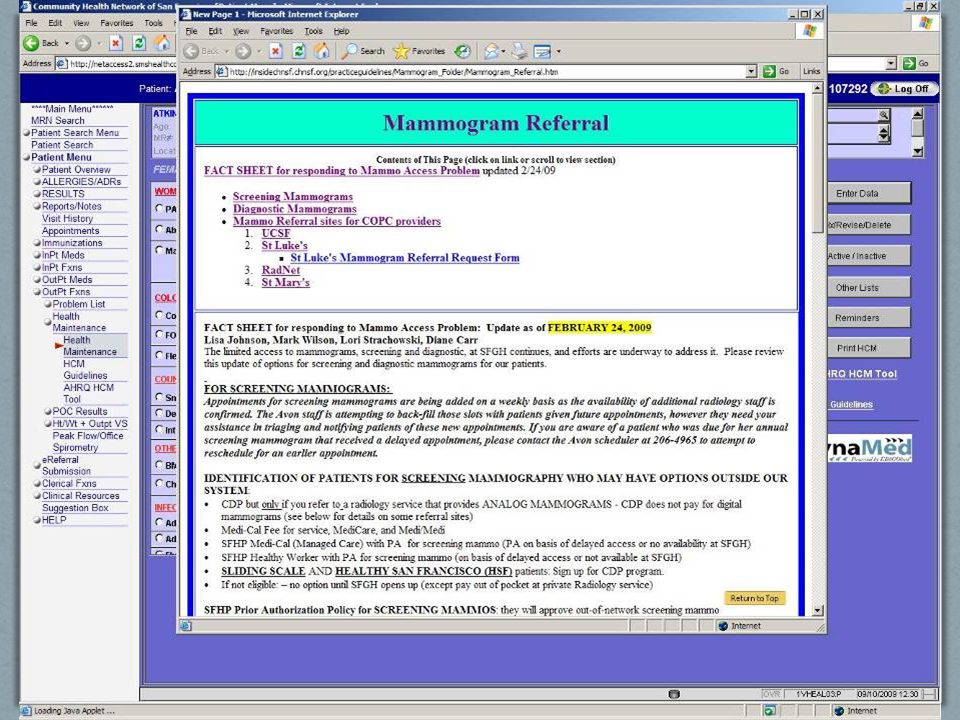
Breast Cancer Screening Challenges Primary care quality improvement committee uses USPSTF guidelines, but specialty society (radiology) recommendations different Difficulties hiring mammographers had led to significant wait times for both screening and diagnostic mammograms Conflicting information given to patients Low mammography rates due to CBE requirement
 recommendations different Difficulties hiring mammographers had led to significant wait times for both screening and diagnostic mammograms Conflicting information given to patients Low mammography rates due to CBE requirement")
33
SF DPH Mamography Rates Percent of women ages 42-69 who have had a mammogram in the past 2 years. Excludes “not indicated” but does not give credit for “declined.” HEDIS 2007 Medicaid HEDIS 2007 Commercial * * Historically not held to requirement for CBE.

34
Conclusions USPSTF guideline process (rigorous, evidence- based, ongoing) critical to reliability and credibility. AHRQ ePSS enables easy access to updated USPSTF guidelines, especially with linkages EMR. Challenges remain with systems barriers that can only be addressed on an institutional level.

35
Questions? Alice Hm Chen, MD, MPH Assistant Professor of Medicine, UCSF Medical Director, Adult Medical Center, SFGH achen@ medsfgh.ucsf.edu

Similar presentations










 Screening Costanza ME, White MJ, Stark JR, Stoddard AM, Avrunin JS, Luckmann.>")
 Prevention Research Center is a new PRC, 2014-2019 Principal.>")







 data only, rate per 1,000 mm. 2014:>")









