Download presentation
Presentation is loading. Please wait.

1
刘学波 葛均波 复旦大学附属中山医院心内科 上海市心血管病研究所 New Progress of mechanical support in AMI patients with cardiogenic shock AMI 合并心源性休克心肺支持技术进展

2
Cardiogenic Shock Incidence ~8% of STEMI in NRMI~8% of STEMI in NRMI 2% of NSTEMI2% of NSTEMI ~50,000 patients per year~50,000 patients per year Babaev et al: JAMA 294:448, 2005 Shock (%) NRMI Registry STEMI
 NRMI Registry STEMI")
3
Cardiogenic Shock Hochman et al. JACC 2000; 36: 1063 Acute myocardial infarction (most common) Pump failure Large infarctionLarge infarction Smaller infarctions with preexisting CHFSmaller infarctions with preexisting CHF Infarction extension or expansionInfarction extension or expansion Mechanical complications Acute MR caused by papillary muscle dysfunction Acute MR caused by papillary muscle dysfunction Free wall rupture Free wall rupture Pericardial tamponade Pericardial tamponade Other conditions End-stage cardiomyopathyEnd-stage cardiomyopathy myocarditismyocarditis prolonged cardiopulmonary bypassprolonged cardiopulmonary bypass aortic stenosisaortic stenosis mitral stenosis mitral stenosis left atrial mxyomaleft atrial mxyoma acute aortic insufficiency acute aortic insufficiency
 Pump failure Large infarctionLarge infarction Smaller infarctions with preexisting CHFSmaller infarctions with preexisting CHF Infarction extension or expansionInfarction extension or expansion Mechanical complications Acute MR caused by papillary muscle dysfunction Acute MR caused by papillary muscle dysfunction Free wall rupture Free wall rupture Pericardial tamponade Pericardial tamponade Other conditions End-stage cardiomyopathyEnd-stage cardiomyopathy myocarditismyocarditis prolonged cardiopulmonary bypassprolonged cardiopulmonary bypass aortic stenosisaortic stenosis mitral stenosis mitral stenosis left atrial mxyomaleft atrial mxyoma acute aortic insufficiency acute aortic insufficiency.")
4
Cardiogenic Shock Patients in NRMI registry presenting with cardiogenic shock who died (%) < 75 years Babaer et al: JAMA 1294:448, 2005 ≥75 years P<0.001 Prognosis
 < 75 years Babaer et al: JAMA 1294:448, 2005 ≥75 years P<0.001 Prognosis")
5
Cardiogenic Shock Temporal trends in mortality AMIS Registry (Switzerland) Jeger, Ann Intern Med 149: 618, 2008
 Jeger, Ann Intern Med 149: 618, 2008")
6
Cardiogenic Shock Timing Present on admission in only 10-15 % of patients who develop CS complicating MI 50 % develop CS rapidly within 6 hr of MI onset. 25 % develop CS later the first day Subsequent CS may to due to reinfarction, or a mechanical complication (MR, VSD)
.")
7
Cardiogenic Shock Temporal trends in incidence AMIS Registry (Switzerland) Jeger, Ann Intern Med 149: 618, 2008
 Jeger, Ann Intern Med 149: 618, 2008")
8
Cardiogenic Shock Pathogenesis Reynolds and Hochmena: Circulation 117:686, 2008 Myocardial infarction Myocardial dysfunction SystolicSystolicDiastolicDiastolic Survival with good quality of life Systemic inflammatory response syndrome (IL-6, TNF- NO) cardiac output stroke volume systemic perfusion Hypotension Compensatory vasoconstriction coronary perfusion pressure Hypoxemia LVEDP Pulmonary congestion IschemiaIschemia DeathDeath Progressive myocardial dysfunction Relief of ischemia Revascularization
 cardiac output stroke volume systemic perfusion Hypotension Compensatory vasoconstriction coronary perfusion pressure Hypoxemia LVEDP Pulmonary congestion IschemiaIschemia DeathDeath Progressive myocardial dysfunction Relief of ischemia Revascularization")
9
Treatment of Acute Myocardial Infarction Goal of Therapy Restore patency Restore flow Restore perfusion Restore function Improve survival What is the additional role of hemodynamic support (over and above reperfusion) on allowing the myocardium to recover?
 on allowing the myocardium to recover")
10
LV pressure and volume unloading with enhanced remodeling capabilityLV pressure and volume unloading with enhanced remodeling capability Decreased wall tension with improved endocardial blood flowDecreased wall tension with improved endocardial blood flow Beating, non-working heart has low metabolic requirementBeating, non-working heart has low metabolic requirement Presumed enhanced ability for cellular repair and survivalPresumed enhanced ability for cellular repair and survival Theoretical Advantages of LVAD

11
Historical Perspectives IABPTandemHeart Impella Hemopump ECMOCPS 90’s80’s70’s00’s

12
Hemodynamic Support Options in Myocardial Infarction

13
IABP Inflation - Diastole Augmentation of diastolic pressureAugmentation of diastolic pressure Increase coronary perfusionIncrease coronary perfusion Increase myocardial oxygen supplyIncrease myocardial oxygen supply Decrease cardiac workDecrease cardiac work Decrease afterloadDecrease afterload Increase cardiac outputIncrease cardiac output IABP Deflation - Systole Intraaortic Balloon Pump

15
The SHOCK Trial (n=302) Randomization from Apr 1993-Nov 1998 Hochman et al: NEJM 341:625, 1999 Primary endpoint: overall 30-day mortalityPrimary endpoint: overall 30-day mortality Secondary endpoints: 6-month and 1-year mortalitySecondary endpoints: 6-month and 1-year mortality Emergency revascularization (n=152) Medical therapy (n=150) Angioplasty or CABG within 6 hours after randomization Angioplasty or CABG within 6 hours after randomization IABP recommended in all pt IABP recommended in all pt IABP IABP Thrombolytic therapy Thrombolytic therapy Delayed revascularization after 54 hours following randomization, if appropriate Delayed revascularization after 54 hours following randomization, if appropriate
 Randomization from Apr 1993-Nov 1998 Hochman et al: NEJM 341:625, 1999 Primary endpoint: overall 30-day mortalityPrimary endpoint: overall 30-day mortality Secondary endpoints: 6-month and 1-year mortalitySecondary endpoints: 6-month and 1-year mortality Emergency revascularization (n=152) Medical therapy (n=150) Angioplasty or CABG within 6 hours after randomization Angioplasty or CABG within 6 hours after randomization IABP recommended in all pt IABP recommended in all pt IABP IABP Thrombolytic therapy Thrombolytic therapy Delayed revascularization after 54 hours following randomization, if appropriate Delayed revascularization after 54 hours following randomization, if appropriate")
16
SHOCK Trial Primary Endpoint Hochman et al: NEJM 341:625, 1999 Proportion alive Days after randomization 30-Day Mortality Medical therapy (n=150) Revascularization (n=152) P=0.11
 Revascularization (n=152) P=0.11")
17
SHOCK Trial Relative Risk for 30-Day Mortality by Subgroups Hochman et al: JAMA 295:2511, 2006 Patients Subgroup(no.) Age <75 yr246 Age 75 yr 56 Men205 Women 97 Transfer admission167 Direct admission135 Time from MI to randomization <6 hr 73 Time from MI to randomization 6 hr227 Eligible for thrombolytic therapy284 Ineligible for thrombolytic therapy 17 Hypertension137 No hypertension159 Diabetes 92 No diabetes204 Prior MI 98 No prior MI204 Anterior MI181 No anterior MI118 U.S. site175 Non-U.S. site127 Revascularization-group benefit Medical-therapy group benefit Relative risk

18
Emergency RevascularizationInitial Medical Stabilization SHOCK Trial: 12-Month Mortality Hochman, JAMA 285: 190, 2001 47.0% 50.0% 54.0% 56.0% 63.0% 67.0% 0% 10% 20% 30% 40% 50% 60% 30-Day (302)6-Month (301)12-Month (299) p=0.109 p=0.025p=0.027 80% 70%
6-Month (301)12-Month (299) p=0.109 p=0.025p= % 70%")
19
SHOCK Trial Long-Term Outcomes Hochman et al: JAMA 295:2511, 2006 Proportion alive Years since randomization Early revascularization, compared to initial medical stabilization, resulted in 13.2% absolute improvement in 6-year survival Early revascularization, compared to initial medical stabilization, resulted in 13.2% absolute improvement in 6-year survival 8 patients needed to be treated to save 1 life 8 patients needed to be treated to save 1 life No. at risk ERV152564233183 IMS150382918 92 Initial medical stabilization Early revascularization All Patients P=0.03

20
ACC-AHA class I recommendationACC-AHA class I recommendation IABP support associated with a in mortalityIABP support associated with a in mortality –NRMI-2 with lysis, from 67% to 49% –SHOCK Trial, from 63% to 47% Intraaortic Balloon Pump

21
A systematic review and meta-analysis of intra aortic balloon pump therapy in ST-elevation myocardial infarction: should we change the guidelines? European Heart Journal Advance Access published January 23, 2009

22
B alloon-pump assisted C oronary I ntervention S tudy BCIS-1 No evidence that Elective IABP to support high risk PCI is associated with a reduction in MACCE at hospital discharge

23
Impella LP 2.5 Transcatheter hemodynamic support devices Tandem Heart

24
“Unloading” – Reducing Work (O 2 Demand) of the Myocardium Work = pressure x volume Work = pressure x volume Ventricular “work” = area of PV loop; proportional to O 2 demand Ventricular “work” = area of PV loop; proportional to O 2 demand Unloading work = reducing area of PV loop Unloading work = reducing area of PV loop Pressure Volume A B C D A.End diastole – mitral valve closure B.Aortic valve opening C.End systole – aortic valve closure D.Mitral valve opening “PV Loop” of the Cardiac Cycle
 of the Myocardium Work = pressure x volume Work = pressure x volume Ventricular work = area of PV loop; proportional to O 2 demand Ventricular work = area of PV loop; proportional to O 2 demand Unloading work = reducing area of PV loop Unloading work = reducing area of PV loop Pressure Volume A B C D A.End diastole – mitral valve closure B.Aortic valve opening C.End systole – aortic valve closure D.Mitral valve opening PV Loop of the Cardiac Cycle")
25
“Unloading” – Reducing Work Inotropic drugs Increase peak systolic pressureIncrease peak systolic pressure Stroke volume increaseStroke volume increase Balloon pump Reducing systolic aortic pressure Reducing systolic aortic pressure Stroke volume increase Stroke volume increase Impella Unloads from ventricle Unloads from ventricle Reduces diastolic volume Reduces diastolic volume Volume Pressure Work reduction Reduced area of PV loop? No: increases PV loop area No: stroke volume increase offsets pressure reduction Yes: volume reduction reduces PV loop area Pressure Volume Pressure Volume

26
Next Generation pVAD: Impella Miniaturized technology (12Fr pump) Rapid insertion across Aortic valve using over the wire technique Pigtail for increased pump stability Catheter (9Fr) for better limb perfusion Flow modulation 2.5L/min (LP 2.5)
 Rapid insertion across Aortic valve using over the wire technique Pigtail for increased pump stability Catheter (9Fr) for better limb perfusion Flow modulation 2.5L/min (LP 2.5)")
27
IMPELLA IMPELLA Catheter Mounted Micro Axial Flow Pump

28
Impella: Platform Technology Impella® 5.0 Impella® 2.5 Console Pumps Implantation

29
Blood 20% Dextrose IV solution is purged through the Motor Area Purge Pressure > 300mmHg, Preventing blood from entering the Motor Area MOTOR Braun Vista Purge System

30
Impella System Cart Components Infusion Pump for Purge System Impella Console Power Supply

31
Impella 2.5 Technology Miniaturized 12F pump Single femoral access Placement with 0.018” wire Actively unloads the LV Forward flow up to 2.5L/min Low anticoagulation

33
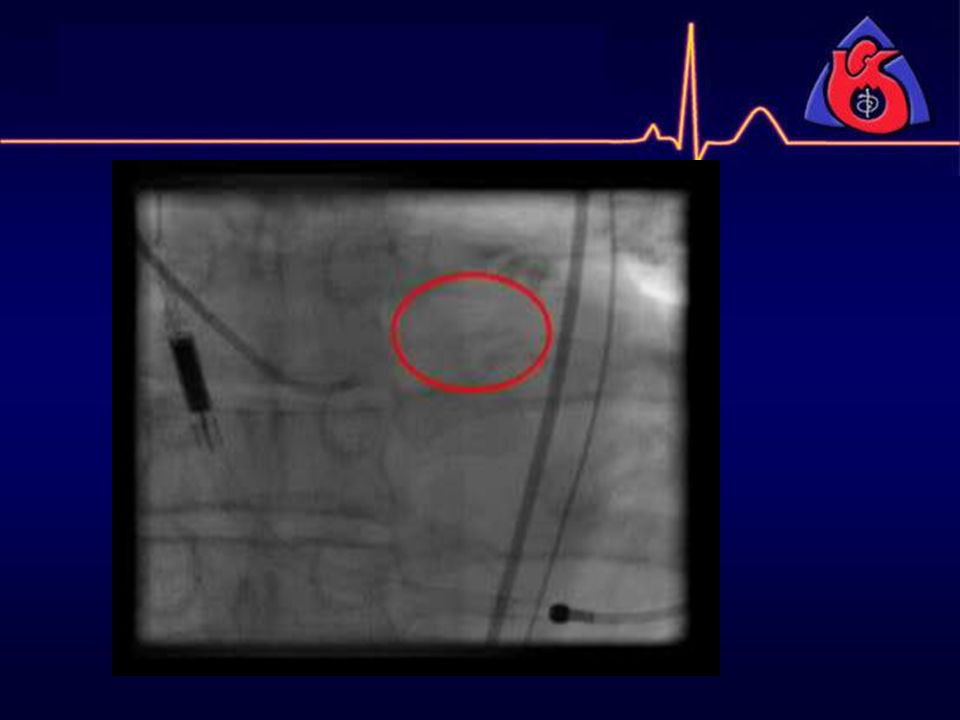
optimal position of aortic valve plane motor cannula in aorta blood inlet area in LV pigtail in LV blood outlet area in aorta RAO: 25 - 30 Inlet cannula centered to the aortic valve Placement of Impella 2.5

34
*Flameng et al 2000 Massive Myocardial damage Up to 5-times reduction in infarct size over base line without offloading Infarct with offloading Potential Reduction in Infarct Size Using Impella Technology Infarct LAD occlusion model Impella products are investigational devices limited by Federal Law solely to investigational use in the United States.

35
ISAR SHOCK Impella 2.5 vs IABP

36
ISAR-SHOCK randomized trial Impella vs. IABP (26 pts) The cardiac index after 30 min was significantly increased in patients with the Impella device compared to patients with IABP (change in CI 0.5 vs. 0.1 L/min/m2, p = 0.02) Overall 30-day mortality was 46 % in both groups. Seyfarth, JACC 2008; 52: 1584.
 The cardiac index after 30 min was significantly increased in patients with the Impella device compared to patients with IABP (change in CI 0.5 vs. 0.1 L/min/m2, p = 0.02) Overall 30-day mortality was 46 % in both groups. Seyfarth, JACC 2008; 52:")
37
PROTECT I Impella is a feasable option for high risk PCI PROTECT II ONGOING TRIAL

38
USPella is the largest study reported so far for Impella 2.5 that confirms prior results: –Impella 2.5 is Safe and Easy to Use –Adverse events/Complications are decreasing –Demonstrated increase in EF post procedure –Provides excellent support to stabilize the patients during high risk interventions and restore the hemodynamics in unstable conditions and refractory shock

39
TandemHeart p-VAD System Removes Oxygenated Blood from Left Atrium via Transeptal cannula inserted via the femoral vein Centrifugal External pump “aspirates” the blood outside the body Return Blood via Femoral artery Provides continuous flow to the systemic circulation

40
Tandem Heart Trans-septal Cannula http://www.cardiacassist.com/Video/TDAnimation.html

41
http://www.cardiacassist.com/Video/PumpAnimation.html Tandem Heart pump

42
Tandem Heart Console

43
TandemHeart: Disadvantages Vascular complications: large femoral arterial return lines (17Fr+) Complex and time consuming insertion requiring transeptal puncture. LA cannula instability Complex nursing care requirements

44
Randomized Trial of Tandem Heart vs IABP n=41 Thiele et al: EHJ 26:1276, 2005 Tandem Heart Percutaneous Device (CardiacAssist, Inc, USA) Transseptal puncture with inflow venous catheter placed in LA Transseptal puncture with inflow venous catheter placed in LA 17 French arterial cannula or two 12 Fr in both femoral arteries 17 French arterial cannula or two 12 Fr in both femoral arteries Delivery 4.0 L/min at 7500 rpm Delivery 4.0 L/min at 7500 rpm ACT 180-200 secs ACT 180-200 secs 42 pt with cardiogenic shock VADn=21VADn=21IABPn=20IABPn=20
 Transseptal puncture with inflow venous catheter placed in LA Transseptal puncture with inflow venous catheter placed in LA 17 French arterial cannula or two 12 Fr in both femoral arteries 17 French arterial cannula or two 12 Fr in both femoral arteries Delivery 4.0 L/min at 7500 rpm Delivery 4.0 L/min at 7500 rpm ACT secs ACT secs 42 pt with cardiogenic shock VADn=21VADn=21IABPn=20IABPn=20")
45
Randomized Trial of Tandem Heart vs IABP n=41 Thiele et al: EHJ 26:1276, 2005 Cardiac power index (W/m 2 ) Hours PrePost81624324048566472 Patients (no.) IABP2020171716161616161616 VAD2121212121191918181717 IABP VAD * * * * Primary endpoint: cardiac power index CI x mean arterial pressure x 0.0022
 Hours PrePost Patients (no.) IABP VAD IABP VAD * * * * Primary endpoint: cardiac power index CI x mean arterial pressure x")
46
Randomized Trial Tandem Heart vs. IABP in Cardiogenic Shock Burkhoff, AHJ 2006; 152:469. * P <.005 vs. baseline, † p < 0.05 vs IABP IABP Tandem Heart Roll In

47
Randomized Trial Tandem Heart vs. IABP in Cardiogenic Shock Burkhoff, AHJ 2006; 152:469. IABP n=14 Tandem Heart n=19 30 d Survival p=ns

48
Cheng et al: EHJ 30:2102, 2009 Cardiac LVADIABPindex meanP heterogeneity=0.22 mean ± SDmean ± SDdifferenceI 2 =34.0% Thiele et al2.3±0.61.8±0.4 0.55 (0.23-0.87) Burkhoff et al2.2±0.62.1±0.2 0.16 (-0.14-0.46) Seyfarth et al2.2±0.61.8±0.7 0.36 (-0.16-0.88) Pooled0.35 (0.09-0.61) Hemodynamic Support Favors IABP Favors LVAD Mean arterial LVADIABPpressure meanP heterogeneity=0.10 mean ± SDmean ± SDdifferenceI 2 =55.9% Thiele et al76±1070±16 5.5 (-2.9-13.9) Burkhoff et al91±1672±1218.6 (9.4-27.9) Seyfarth et al87±1871±2216.0 (0.5-31.5) Pooled12.8 (3.8-22.0) Favors IABP Favors LVAD Pulmonary wedge LVADIABPpressure meanP heterogeneity=0.01 mean ± SDmean ± SDdifferenceI 2 =76.6% Thiele et al16±522±7 -5.6 (-9.2 to -2.1) Burkhoff et al16±425±3 -8.4 (-11.o to -5.8) Seyfarth et al19±520±6-1.0 (-5.2-3.2) Pooled -5.3 (-9.4 to -1.2) Favors LVAD Favors IABP IABP vs LVAD Meta-Analysis
 Burkhoff et al2.2±0.62.1± ( ) Seyfarth et al2.2±0.61.8± ( ) Pooled0.35 ( ) Hemodynamic Support Favors IABP Favors LVAD Mean arterial LVADIABPpressure meanP heterogeneity=0.10 mean ± SDmean ± SDdifferenceI 2 =55.9% Thiele et al76±1070± ( ) Burkhoff et al91±1672± ( ) Seyfarth et al87±1871± ( ) Pooled12.8 ( ) Favors IABP Favors LVAD Pulmonary wedge LVADIABPpressure meanP heterogeneity=0.01 mean ± SDmean ± SDdifferenceI 2 =76.6% Thiele et al16±522± (-9.2 to -2.1) Burkhoff et al16±425± (-11.o to -5.8) Seyfarth et al19±520±6-1.0 ( ) Pooled -5.3 (-9.4 to -1.2) Favors LVAD Favors IABP IABP vs LVAD Meta-Analysis")
49
Cheng et al: EHJ 30:2102, 2009 LVADIABP30-day mortalityP (heterogeneity=0.83 (no.)(no.)relative riskI 2 =0% Thiele et al 9/21 9/200.95 (0.48-1.90) Burkhoff et al 9/19 5/141.33 (0.57-3.10) Seyfarth et al 6/13 6/131.00 (0.44-2.29) Pooled24/5320/471.06 (0.68-1.66) Favors LVAD 30-Day Mortality Favors IABP IABP vs LVAD Meta-Analysis
(no.)relative riskI 2 =0% Thiele et al 9/21 9/ ( ) Burkhoff et al 9/19 5/ ( ) Seyfarth et al 6/13 6/ ( ) Pooled24/5320/ ( ) Favors LVAD 30-Day Mortality Favors IABP IABP vs LVAD Meta-Analysis")
50
Cheng et al: EHJ 30:2102, 2009 Complications Reported fever LVADIABPor sepsisP heterogeneity=0.10 (no.)(no.)relative riskI 2 =62.1 Thiele et al17/2110/201.62 (1.0-2.63) Burkhoff et al 4/19 5/14 0.59 (0.19-1.80) Pooled21/4015/34 1.11 (0.43-2.90) Favors LVAD Favors IABP 0.010.1110100 Reported leg LVADIABPischemia P heterogeneity=0.38 (no.)(no.)relative riskI 2 =0% Thiele et al 7/210/2014.32 (0.87-235.4) Burkhoff et al 4/192/141.47 (0.31-6.95) Seyfarth et al 1/130/133.00 (0.13-67.51) Pooled12/532/472.59 (0.75-8.97) Favors LVAD Favors IABP Reported LVADIABPbleeding P heterogeneity=0.73 (no.)(no.)relative riskI 2 =0% Thiele et al 19/21 8/202.26 (1.30-3.94) Burkhoff et al 8/19 2/14 2.95 (0.74-11.80) Pooled27/4010/342.35 (1.40-3.93) Favors LVAD Favors IABP 0.00010.01110010,0000.010.1110100
(no.)relative riskI 2 =62.1 Thiele et al17/2110/ ( ) Burkhoff et al 4/19 5/ ( ) Pooled21/4015/ ( ) Favors LVAD Favors IABP Reported leg LVADIABPischemia P heterogeneity=0.38 (no.)(no.)relative riskI 2 =0% Thiele et al 7/210/ ( ) Burkhoff et al 4/192/ ( ) Seyfarth et al 1/130/ ( ) Pooled12/532/ ( ) Favors LVAD Favors IABP Reported LVADIABPbleeding P heterogeneity=0.73 (no.)(no.)relative riskI 2 =0% Thiele et al 19/21 8/ ( ) Burkhoff et al 8/19 2/ ( ) Pooled27/4010/ ( ) Favors LVAD Favors IABP ,")
51
Devices for Transcatheter Hemodynamic Support for Left-Heart Failure Conclusions The effect of transcatheter left ventricular assist devices in high risk PCI and AMI complicated by cardiogenic shock remains to be proven. While no mortality benefit has been demonstrated with LVEDs compared to IABP, preliminary data (MACH 2) suggest greater improvement in LV recovery. The Impella 2.5 is currently being investigated in the setting of high-risk PCI in the PROTECT II Trial. However, more widespread application of timely reperfusion to prevent cardiogenic shock in AMI patients including pre-hospital triage (ECG), effective nationwide STEMI networks and 24 x 7 D2B interventional teams may have the greatest impact on reducing mortality from current levels.
 suggest greater improvement in LV recovery. The Impella 2.5 is currently being investigated in the setting of high-risk PCI in the PROTECT II Trial. However, more widespread application of timely reperfusion to prevent cardiogenic shock in AMI patients including pre-hospital triage (ECG), effective nationwide STEMI networks and 24 x 7 D2B interventional teams may have the greatest impact on reducing mortality from current levels..")
52
ACC/AHA Guidelines for PCI in Patients with Cardiogenic Shock Primary PCI is recommended for patients <75 years with ST elevation or LBBB or who develop shock within 36 hours of MI and are suitable for revascularization that can be performed within 18 hours of shock Primary PCI is reasonable for selected patients 75 years with ST elevation or LBBB or who develop shock within 36 hours of MI and are suitable for revascularization that can be performed within 18 hours of shock AIIIaIIbIII BIIIaIIbIII

53
复 旦 大 学 附 属 中 山 医 院 新 貌 谢谢!

Similar presentations

 VAD (Ventricular assist device)>")


>")















>")