Download presentation
Presentation is loading. Please wait.

1
Calcium..PTH .. CaSR Vitamin D
RANIA AHMED ENDOCRINE August 15 ,2012

2
Objective Calcium homeostasis PTH structure and function
CaSR structure and actions Vitamin D metabolism Calcitonin

3
CALCIUM HOMEOSTASIS Serum calcium concentrations are normally maintained within the very narrow range that is required for the optimal activity of extracellular and intracellular processes. Intracellular : secretion ,differentiation , proliferation , motility ,and cell death. Extracellular: »hormones secretion »excitation-contraction »synaptic transmission »platelet aggregation and coagulation.

6
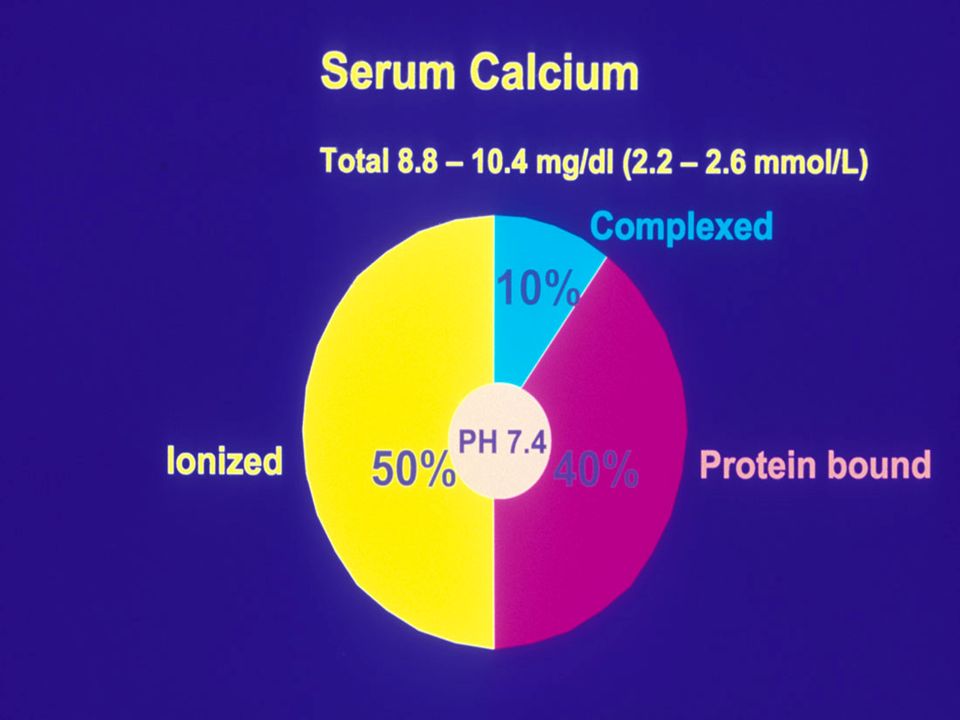
Calcium Metabolism 40 % bound to plasma proteins , albumin
10 % bound to small anions such as phosphate and citrate 50% Ionized state Concentration of ionized ca 1.25±0.07mmol/L, It is the ionized ca that is regulated in extracellular fluid .

7
Calcium Metabolism Based on a balance between intestinal absorption, bone mineralization and demineralization, and urinary filtration and reabsorption. Major direct regulators: Dietary intake Parathyroid hormone (PTH) 1,25 (OH)2-cholecalciferol Calcitonin.
 1,25 (OH)2-cholecalciferol. Calcitonin.")
9
PTH PTH

10
Embryology The parathyroid glands develop at 6 weeks.
Superior parathyroid glands develop with the thyroid gland from the fourth branchial pouch and are residing lateral and posterior to the upper pole of the thyroid at the level of the cricothyroid cartilage. Inferior parathyroid glands descend with the thymus from the third branchial pouch and migrate to the level of the aortic arch or, rarely, fail to migrate, remaining in the high neck parathyroid glands typically located posterolateral to the thyroid

12
Anatomy Number of glands: can vary from 4-6
They measure 6 x 4 x 2 mm in maximum diameter and weigh mg each. Arterial supply: inferior thyroid artery venous drainage: inferior, middle, superior thyroid veins Adult parathyroid gland: 50% parenchyma 50% fat cell types: chief cells oxyphil cells Both types make Parathyroid hormone .

13
Parathyroid Hormone peptide hormone secreted by chief cells
half-life is only 10 minutes. Increased by: low serum calcium Decreased by: high serum calcium, low magnesium, High 1,25 dihydroxy vitamin D

14
Parathyroid Hormone PTH is synthesized in the parathyroid gland as a precursor hormone,preproparathyroid hormone, which is cleaved first to proparathyroid hormone and then to the final 84-amino-acid PTH. Secreted PTH has a half-life of 2 to 4 minutes. In the liver, PTH is metabolized into the active N-terminal component and the relatively inactive C-terminal fraction

15
PTH Receptors PTH1R expressed in bone and kidney, and also present in breast ,skin ,heart ,blood vessels and pancreas PTH1R binds intact PTH and N-terminal residues. Activation of PTH1R activates multiple cellular pathways and release intracellular calcium stores. PTH2R expressed in the CNS,CVS ,GIT, lung and testes PTH2R selectively binds PTH only. C-PTHRs which present in bone with specificity to carboxyl-terminal region of PTH, PTH 7-84 and shown to possess hypocalcemic activity ,that is reserved by PTH1-34and PTH 1-84.

16
Action of PTH : Calcium PTH acts to increase the plasma Ca2+ concentration in three ways : It stimulates bone resorption, resulting in the release of calcium phosphate. It enhances intestinal Ca2+ and phosphate absorption by promoting the formation of calcitriol (1,25 dihydroxycholecalciferol)within the kidney. It augments active renal Ca2+ reabsorption.
within the kidney. It augments active renal Ca2+ reabsorption.")
17
Regulation of PTH Secretion: Calcitriol & Ions
Calcitriol (1,25-OH-Vit D) Binds to the intracellular vitamin D receptor and inhibits PTH gene expression Inhibits parathyroid cell proliferation Magnesium Maintains normal parathyroid secretory response Hypomagnesemia impairs response to PTH and its release hypocalcemia Phosphate Hyperphosphatemia stimulates PTH secretion Stimulates parathyroid growth
 Binds to the intracellular vitamin D receptor and inhibits PTH gene expression. Inhibits parathyroid cell proliferation. Magnesium. Maintains normal parathyroid secretory response. Hypomagnesemia impairs response to PTH and its release hypocalcemia. Phosphate. Hyperphosphatemia stimulates PTH secretion. Stimulates parathyroid growth.")
18
Effects of PTH on Bone Increase bone turnover, osteoclastic bone resorption and new bone formation Intermittent PTH administration has anabolic activity on bone Enhanced mineralization, recruitment of osteoblasts and reduction of apoptosis Continous administration/secretion results in bone resorption Osteoclast activation occurs secondarily to osteoblast recruitment

19
Renal Actions of PTH Stimulate Ca reabsorption
Inhibits proximal and distal reabsorption of phosphate Stimulate Synthesis of 1,25-OH-Vitamin D

20
PTH homeostasis PTH Homeostasis

22
Calcium-ion Sensing Receptor (CaSR)
A G-protein coupled receptor Located on the cell surfaces of parathyroid and renal tissues, Also in thyroidal C cells, brain cells & GI tract Mediates the effects of Ca on target tissues & acts as a first-messenger

23
Calcium sensing receptors
Allows the parathyroid gland to detect changes in Ca concentration Actions aim to normalize serum calcium concentration Decrease in serum Ca concentration is a potent stimulus for PTH release

24
Effects of CaSR on PTH In hypercalcemia, CaSR acts to:
Increase intracellular calcium Decrease PTH production Decrease PTH secretion Increase PTH degradation and promotes urinary Ca2+ excretion In chronic hypocalcemia, CaSR affects: PTH gene expression Parathyroid cell proliferation

26
Renal Effects of CaSR CaSR expressed heavily in the thick ascending limb of the Loop of Henle. CaSR also expressed in the collecting duct.

27
Located on the basolateral aspect of cells
Elevated serum Ca inhibits reabsorption of filtered Ca, Mg and NaCl Located on the apical aspect of cells Inhibits ADH action inhibits concentration of urine and results in isotonic polyuria

28
Disorders with parathyroid-specific decrease in sensitivity to Ca2+
Disorders of extracellular calcium-sensing by the calcium-sensing receptor (CaSR) Disorders with generalized decrease in sensitivity to Ca2+ (affecting all CaSR-expressing tissue) 1. Familial hypocalciuric hypercalcemia (FHH) 2. Neonatal (NHPT) and neonatal severe hyperparathyroidism (SHPT) 3. Familial isolated hyperparathyroidism caused by CaSR mutations 4. Autoimmune hypocalciuric hypercalcemia Disorders with parathyroid-specific decrease in sensitivity to Ca2+ 1. Primary hyperparathyroidism 2. Severe uremic secondary and tertiary hyperparathyroidism Disorders with generalized increase in sensitivity to Ca2+ 1. Autosomal dominant hypoparathyroidism (ADH) due to activating CaSR mutations 2. ADH with features of Bartter's syndrome 3. Hypoparathyroidism due to activating antibodies to the CaSR
 Disorders with generalized decrease in sensitivity to Ca2+ (affecting all CaSR-expressing tissue) 1. Familial hypocalciuric hypercalcemia (FHH) 2. Neonatal (NHPT) and neonatal severe hyperparathyroidism (SHPT) 3. Familial isolated hyperparathyroidism caused by CaSR mutations. 4. Autoimmune hypocalciuric hypercalcemia. Disorders with parathyroid-specific decrease in sensitivity to Ca2+ 1. Primary hyperparathyroidism. 2. Severe uremic secondary and tertiary hyperparathyroidism. Disorders with generalized increase in sensitivity to Ca2+ 1. Autosomal dominant hypoparathyroidism (ADH) due to activating CaSR mutations. 2. ADH with features of Bartter s syndrome. 3. Hypoparathyroidism due to activating antibodies to the CaSR.")
29
Inactivating Mutations of CaSR: Familial Hypocalciuric Hypercalcemia
Autosomal dominant condition resulting in partial CaSR function loss About 200 mutations have been identified Mutated CaSR less sensitive to Ca therefore higher concentrations required to decrease PTH release from parathyroid glands In the kidney, defect results in increased tubular Ca and Mg reabsorption Net result is hypercalcemia, hypocalciuria, hypermagnesemia, inappropriately normal or high PTH

30
Activating Mutations of CaSR: Autosomal Dominant Hypocalcemia
Caused by activating mutation of CaSR CaSR more sensitive to serum calcium levels therefore PTH release inhibited at lower serum Ca levels In the kidneys, reabsorption of Ca inhibited at lower serum Ca levels Net result is hypocalcemia, hypercalciuria and inappropriately low or normal PTH

31
Vitamin D Lipid soluble compounds with a four-ringed cholesterol backbone. SOURCES — Food and Sunlight. Ultraviolet light photoisomerize provitamin D to vitamin D3 (cholecalciferol) in the skin from 7-dehydrocholesterol Vitamin D transported in the blood principally bind to DBP (85%) and albumin (15%).
 in the skin from 7-dehydrocholesterol. Vitamin D transported in the blood principally bind to DBP (85%) and albumin (15%).")
32
Vitamin D Vitamin D2 is manufactured through the ultraviolet irradiation of ergosterol, it has a lower affinity than 25-hydroxyvitamin D3 for vitamin D-binding protein. Thus, 25-hydroxyvitamin D2 has a shorter half-life than 25OHD3 Production of 1,25(OH)2D in the kidney stimulated by PTH and IGF-1 and inhibited by FGF23 and high levels of calcium and phosphate.
2D in the kidney stimulated by PTH and IGF-1 and inhibited by FGF23 and high levels of calcium and phosphate.")
34
VIT D Action 1,25-dihydroxyvitamin D binds to intracellular receptors VDR in target tissues and regulates gene transcription Its most important biological action is to promote enterocyte differentiation and the intestinal absorption of calcium. Stimulation of intestinal phosphate absorption, direct suppression of PTH release, regulation of osteoblast function, and allowing PTH-induced osteoclast activation and bone resorption Production of 1,25(OH)2D in the kidney stimulated by PTH and IGF-1 and inhibited by FGF23 and high levels of calcium and phosphate
2D in the kidney stimulated by PTH and IGF-1 and inhibited by FGF23 and high levels of calcium and phosphate.")
35
Action in Intestine 1,25 (OH)2D enhance the efficacy of small intestine to absorb calcium and phosphorus. Both vitamin D and VDR are required for optimal absorption of calcium. Vitamin D induce active cellular calcium uptake and transport mechanisms. Calcium uptake is the rate limiting step in intestinal calcium absorption, which is highly dependent on vitD. Vitamin D increase active phosphorus transport.

36
Action in Bone Vitamin D is essential for the development & maintenance of mineralized skeleton. Osteoblastic bone formation and osteoclastic bone resorption demand both vitamin D and VDR. 1,25(OH)2D VDR system is critical in PTH induced osteoclastogenesis. 1,25(OH)2D VDR increased the expression of RANKL on the surface of osteoblast ,RANK interaction with its receptor RANKL promotes maturation of osteoclast progenitor cell & mature osteoclast. Vitamin D ,PTH and prostaglandin stimulate RANKL expression.
2D VDR system is critical in PTH induced osteoclastogenesis. 1,25(OH)2D VDR increased the expression of RANKL on the surface of osteoblast ,RANK interaction with its receptor RANKL promotes maturation of osteoclast progenitor cell & mature osteoclast. Vitamin D ,PTH and prostaglandin stimulate RANKL expression.")
37
Action in Kidney The kidney expresses VDR, and 1,25 (OH)2D stimulate Ca²-ATPase in distal tubule as well as 24,25(OH)2D production in the proximal tubule. 1,25 dihydroxyvitamin D decrease its own synthesis through negative feedback and decrease secretion and synthesis of PTH. 1,25 dihydroxyvitamin D increase expression of 25-hydroxyvitamin D-24-hydroxylase to catabolize 1,25(OH)2D to the water-soluble ,biological inactive calcitroic acid .
2D stimulate Ca²-ATPase in distal tubule as well as 24,25(OH)2D production in the proximal tubule. 1,25 dihydroxyvitamin D decrease its own synthesis through negative feedback and decrease secretion and synthesis of PTH. 1,25 dihydroxyvitamin D increase expression of 25-hydroxyvitamin D-24-hydroxylase to catabolize 1,25(OH)2D to the water-soluble ,biological inactive calcitroic acid .")
39
Denosumab in postmenopausal women with osteoporosis
Human monoclonal antibody to RANK ligand [RANK-L]) Approved for the treatment of postmenopausal osteoporosis in June 2010, and is highly effective in reducing the risk of vertebral, nonvertebral, and hip fracture risk.
 Approved for the treatment of postmenopausal osteoporosis in June 2010, and is highly effective in reducing the risk of vertebral, nonvertebral, and hip fracture risk.")
40
Mechanism of action Denosumab binds to osteoblast-produced RANK-L, thereby preventing RANK-L from binding to the osteoclast receptor, RANK. By preventing RANK-L from binding to RANK, there is less osteoclast differentiation and activity so that bone resorption decreases.

42
Denosumab 'FREEDOM' 5-year data indicates continued safety and efficacy, and will be extended. Denosumab offers a highly effective and safe parenteral therapy for osteoporosis and is being studied long term with the extension of the FREEDOM trial, and in other osteoporotic states - in men and glucocorticoid-induced osteoporosis. Dose of 60 mg by subcutaneous injection every 6 months.

44
The results of the pivotal registration fracture trial with denosumab versus placebo (‘FREEDOM’). Over 3 years denosumab (60 mg as a subcutaneous injection every 6 months) significantly reduced the incidence of vertebral, nonvertebral and hip fractures compared with placebo [Cummings et al. 2009]. Composite measurement excluding pathological fractures and those associated with severe trauma, fractures of vertebrae, skull, face mandible, metacarpals, fingers and toes.
![The results of the pivotal registration fracture trial with denosumab versus placebo (‘FREEDOM’). Over 3 years denosumab (60 mg as a subcutaneous injection every 6 months) significantly reduced the incidence of vertebral, nonvertebral and hip fractures compared with placebo [Cummings et al. 2009].](http://slideplayer.com/slide/7550535/24/images/44/The+results+of+the+pivotal+registration+fracture+trial+with+denosumab+versus+placebo+%28%E2%80%98FREEDOM%E2%80%99%29.+Over+3+years+denosumab+%2860+mg+as+a+subcutaneous+injection+every+6+months%29+significantly+reduced+the+incidence+of+vertebral%2C+nonvertebral+and+hip+fractures+compared+with+placebo+%5BCummings+et+al.+2009%5D..jpg "Composite measurement excluding pathological fractures and those associated with severe trauma, fractures of vertebrae, skull, face mandible, metacarpals, fingers and toes.")
45
CAlCITONIN Calcitonin is a 32-amino-acid peptide
Calcitonin secreted by parafollicular C cells of the thyroid. Secretion of calcitonin is under the control of ionized ca. CaSR expressed on C cell of thyroid ,high extracellular calcium increase secretion of calcitonin. Hypocalcaemia inhibit calcitonin secretion.

46
Action of CALCITONIN Osteoclast and proximal renal tubule cells express calcitonin receptors. In the bone calcitonin inhibit osteoclastic bone resorption. In the kidney calcitonin inhibits the reabsorption of PO4 and increase renal excretion of calcium.

48
THANK YOU

Similar presentations












 builds up the internal frame.>")

 –Free calcium is 1.2 mM.>")



![Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.](/12/3581741/big_thumb.jpg "Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.>")










