Download presentation
Presentation is loading. Please wait.

1
Chapter 13 Bronchiectasis

2
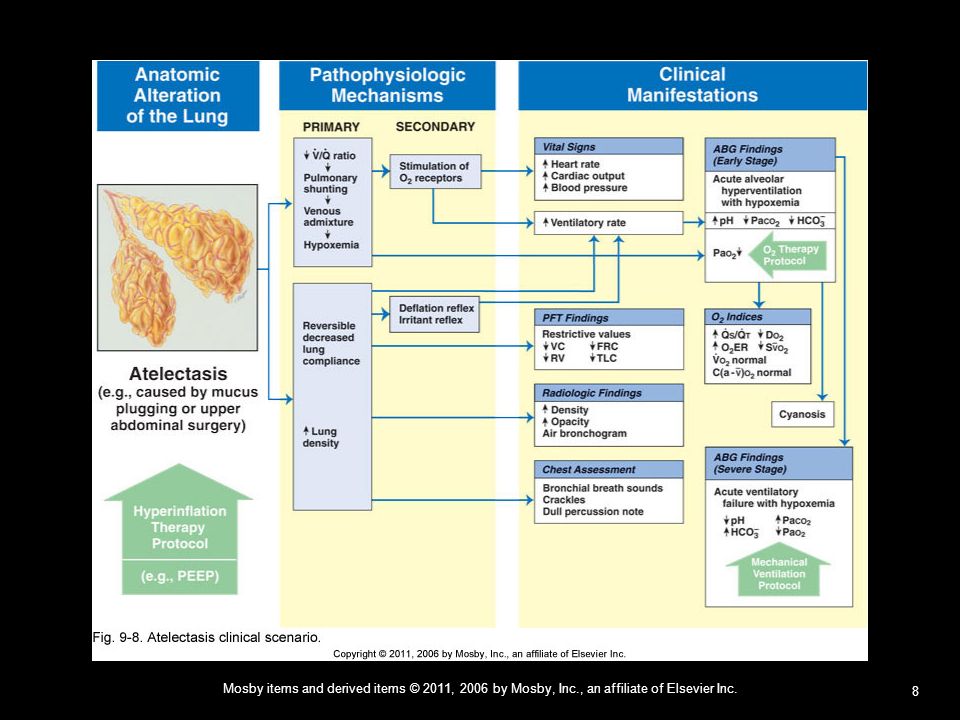
C E A B D Figure Bronchiectasis. A, Varicose bronchiectasis. B, Cylindrical bronchiectasis. C, Cystic (saccular) bronchiectasis. Also illustrated are excessive bronchial secretions (D) and atelectasis (E), which are both common anatomic alterations of the lungs in this disease.
 bronchiectasis. Also illustrated are excessive bronchial secretions (D) and atelectasis (E), which are both common anatomic alterations of the lungs in this disease.")
3
Three Forms of Bronchiectasis
Cylindrical bronchiectasis Also called Tubular bronchiectasis Varicose bronchiectasis Also called Fusiform bronchiectasis Cystic bronchiectasis Also called Saccular bronchiectasis

4
Anatomic Alterations of the Lungs
Chronic dilation and distortion of bronchial airways Excessive production of often foul-smelling sputum Bronchospasm Hyperinflation of alveoli (air-trapping) Atelectasis, and parenchymal fibrosis Hemorrhage secondary to bronchial arterial erosion
 Atelectasis, and parenchymal fibrosis. Hemorrhage secondary to bronchial arterial erosion.")
5
Etiology Acquired bronchiectasis Congenital bronchiectasis
Recurrent pulmonary infection Bronchial obstruction Inhalation and aspiration Congenital bronchiectasis Kartagener’s syndrome Systemic disorders

6
Overview of the Cardiopulmonary Clinical Manifestations Associated with Bronchiectasis
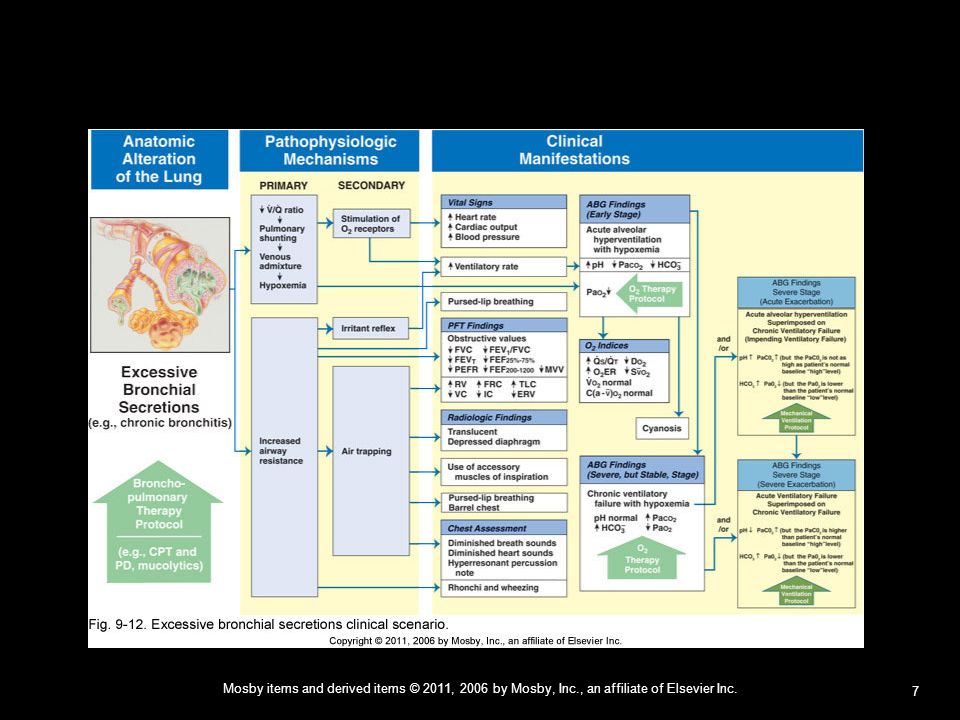
The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Excessive Bronchial Secretions Bronchospasm Increased Alveolar-Capillary Membrane Thickness
 by. Excessive Bronchial Secretions. Bronchospasm. Increased Alveolar-Capillary Membrane Thickness.")
9
Figure 9-11. Bronchospasm clinical scenario (e.g., asthma).
Figure Bronchospasm clinical scenario (e.g., asthma).
.")
10
Figure 9-9. Alveolar consolidation clinical scenario.

11
Figure 9-10. Increased alveolar-capillary membrane thickness clinical scenario.

12
Clinical Data Obtained at the Patient’s Bedside Depending on the amount of bronchial secretions, and the degree of bronchial destruction and fibrosis associated with bronchiectasis, the disease may create either an obstructive lung disorder, or a restrictive lung disorder, or a combination of both. If the disease is limited to a relatively small portion of the lungs—as it often is—the patient may not have any of the following clinical manifestations.

13
The Physical Examination
Vital Signs Increased Respiratory rate (Tachypnea) Heart rate (pulse) Blood pressure
 Heart rate (pulse) Blood pressure.")
14
The Physical Examination (Cont’d)
Use of accessory muscles of inspiration Use of accessory muscles of expiration Pursed-lip breathing

15
The Physical Examination (Cont’d)
Increased anteroposterior chest diameter (barrel chest) Cyanosis Digital clubbing
 Cyanosis. Digital clubbing.")
16
The Physical Examination (Cont’d)
Peripheral edema and venous distension Distended neck veins Pitting edema Enlarged and tender liver

17
The Physical Examination (Cont’d)
Cough, sputum production, and hemoptysis Chronic cough with production of large quantities of foul-smelling sputum is a hallmark of bronchiectasis.

18
The Physical Examination (Cont’d)
Chest Assessment Findings When primarily obstructive in nature: Decreased tactile and vocal fremitus Hyperresonant percussion note Diminished breath sounds Wheezing Rhonchi

19
The Physical Examination (Cont’d)
Chest Assessment Findings When primarily restrictive in nature (i.e., over areas of atelectasis and consolidation): Increased tactile and vocal fremitus Bronchial breath sounds Crackles Whispered pectoriloquy Dull percussion note
: Increased tactile and vocal fremitus. Bronchial breath sounds. Crackles. Whispered pectoriloquy. Dull percussion note.")
20
Clinical Data Obtained from Laboratory Tests and Special Procedures

21
Pulmonary Function Test Findings When Primarily Obstructive in Nature
(Moderate to Severe Bronchiectasis) Forced Expiratory Flow Rate Findings FVC FEVT FEV1/FVC ratio FEF25%-75 FEF50% FEF PEFR MVV
 Forced Expiratory Flow Rate Findings. FVC FEVT FEV1/FVC ratio FEF25%-75. FEF50% FEF PEFR MVV. ")
22
Pulmonary Function Test Findings
When Primarily Obstructive in Nature Moderate to Severe Bronchiectasis Lung Volume & Capacity Findings VT IRV ERV RV VC N or N or N or IC FRC TLC RV/TLC ratio N or N or N or

23
Pulmonary Function Test Findings When Primarily Restrictive in Nature
(Moderate to Severe Bronchiectasis) Forced Expiratory Flow Rate Findings FVC FEVT FEV1/FVC ratio FEF25%-75 N or N or N or FEF50% FEF PEFR MVV N or N or N or N or
 Forced Expiratory Flow Rate Findings. FVC FEVT FEV1/FVC ratio FEF25%-75. N or N or N or FEF50% FEF PEFR MVV. N or N or N or N or ")
24
Pulmonary Function Test Findings
When Primarily Restrictive in Nature Moderate to Severe Bronchiectasis Lung Volume & Capacity Findings VT IRV ERV RV VC N or IC FRC TLC RV/TLC ratio N

25
Arterial Blood Gases Bronchiectasis
Mild to Moderate Stages Acute Alveolar Hyperventilation with Hypoxemia (Acute Respiratory Alkalosis) pH PaC HCO Pa02 (slightly)
 pH PaC02 HCO3 Pa02. (slightly) ")
26
PaO2 and PaCO2 trends during acute alveolar hyperventilation.

27
Arterial Blood Gases Bronchiectasis
Severe Stage Chronic Ventilatory Failure with Hypoxemia (Compensated Respiratory Acidosis) pH PaC HCO Pa02 N (Significantly)
 pH PaC02 HCO3 Pa02. N (Significantly) ")
28
PaO2 and PaCO2 trends during acute or chronic ventiliatory failure.

29
Arterial Blood Gases Bronchiectasis
Acute Ventilatory Changes Superimposed On Chronic Ventilatory Failure Because acute ventilatory changes are frequently seen in patients with chronic ventilatory failure, the respiratory care practitioner must be familiar with and alert for the following: Acute alveolar hyperventilation superimposed on chronic ventilatory failure Acute ventilatory failure (acute hypoventilation) superimposed on chronic ventialtory failure.
 superimposed on chronic ventialtory failure.")
30
Moderate to Severe Stages
Oxygenation Indices Moderate to Severe Stages QS/QT D V C(a-v) ER Sv02 N N
02 02ER Sv02. N N ")
31
Moderate to Severe Stages
Hemodynamic Indices Moderate to Severe Stages CVP RAP PA PCWP CO SV N N N SVI CI RVSWI LVSWI PVR SVR N N N N

32
Abnormal Laboratory Tests and Procedures
Increased hematocrit and hemoglobin Elevated white blood count if acutely infected Sputum examination Streptococcus pneumoniae Haemophilus influenzae Pseudomonas aeruginosa Anaerobic organisms

33
Radiologic Findings Chest Radiograph
When the bronchiectasis is primarily obstructive in nature Translucent (dark) lung fields Depressed or flattened diaphragms Long and narrow heart (pulled down by diaphragms) Areas of consolidation and/or atelectasis may or may not be seen
 lung fields. Depressed or flattened diaphragms. Long and narrow heart (pulled down by diaphragms) Areas of consolidation and/or atelectasis may or may not be seen.")
34
Figure 13-2. Gross cystic bronchiectasis
Figure Gross cystic bronchiectasis. Posteroanterior chest radiograph showing overinflated lungs. There are multiple ring opacities, most obvious at the lung bases, ranging from 3 to 15 mm in diameter. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of diseases of the chest, ed 4, Philadelphia, 2005, Elsevier.)
")
35
Figure 13-3. Left lower lobe bronchiectasis
Figure Left lower lobe bronchiectasis. The marked volume loss of left lower lobe is indicated by a depressed hilum, vertical left mainstem bronchus, mediastinal shift, and left-sided transradiancy. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of diseases of the chest, ed 4, Philadelphia, 2005, Elsevier.)
")
36
Figure 13-4. Ciliary dyskinesia syndrome—Kartagener’s syndrome
Figure Ciliary dyskinesia syndrome—Kartagener’s syndrome. This 62-year-old woman gave a 40 year history consistent with bronchiectasis. The aortic arch, descending aorta, heart, and gastric air bubble are all on the right side. There is diffuse complex pulmonary shadowing with many ring opacities. Broad-branching band shadows can just be seen through heart and represent dilated fluid-filled airways.

37
Figure 13-5. Cylindrical bronchiectasis
Figure Cylindrical bronchiectasis. Left posterior oblique projection of a left bronchogram showing cylindrical bronchiectasis affecting the whole of the lower lobe except for the superior segment. Few side branches fill. Basal airways are crowded together, indicating volume loss of the lower lobe, a common finding in bronchiectasis. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of diseases of the chest, ed 4, Philadelphia, 2005, Elsevier.)
")
38
Figure 13-6. Cystic (saccular) bronchiectasis
Figure Cystic (saccular) bronchiectasis. Right lateral bronchogram showing cystic bronchiectasis affecting mainly the lower lobe and posterior segment of the upper lobe. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of diseases of the chest, ed 4, Philadelphia, 2005, Elsevier.)
 bronchiectasis. Right lateral bronchogram showing cystic bronchiectasis affecting mainly the lower lobe and posterior segment of the upper lobe. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of diseases of the chest, ed 4, Philadelphia, 2005, Elsevier.)")
39
Figure 13-7. Varicose bronchiectasis
Figure Varicose bronchiectasis. Left posterior oblique projection of left bronchogram in a patient with the ciliary dyskinesia syndrome. All basal bronchi are affected by varicose bronchiectasis. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of diseases of the chest, ed 4, Philadelphia, 2005, Elsevier.)
")
40
Radiologic Findings (Cont’d) Computed Tomography (CT Scan)
The bronchial walls may appear as follows: Thick Dilated Characterized by ring lines or clusters Signet ring-shaped Flamed-shaped

41
Figure 13-8. Signet ring sign in patient with cystic fibrosis.

42
Figure 13-9. Cylindrical bronchiectasis
Figure Cylindrical bronchiectasis. A and B, Examples from two patients. Airways parallel to the plane of the section in anterior segment of an upper lobe show changes of cylindrical bronchiectasis; bronchi are wider than normal and fail to taper as they proceed toward the lung periphery.

43
Figure 13-10. Varicose bronchiectasis
Figure Varicose bronchiectasis. Patient with allergic bronchopulmonary aspergillosis and cystic fibrosis. The bronchiectatic airways have a corrugated, or beaded, appearance.

44
Figure 13-11. Cystic bronchiectasis (advanced) in the upper lobes.
 in the upper lobes.")
45
General Management of Bronchiectasis
General treatment includes: Controlling pulmonary infections Controlling airway secretions Preventing complications

46
General Management of Bronchiectasis (Cont’d)
Respiratory care treatment protocols Oxygen Therapy Protocol Bronchopulmonary Hygiene Therapy Protocol Lung Expansion Therapy Protocol Aerosolized Medication Therapy Protocol Mechanical ventilation protocol

47
General Management of Bronchiectasis (Cont’d)
Other medications commonly prescribed by the physician Expectorants Antibiotics

48
Classroom Discussion Case Study: Bronchiectasis

Similar presentations


 –Partial.>")
















