Download presentation
Presentation is loading. Please wait.

1
THE URBAN INSTITUTE 1 Innovative strategies to enroll eligible people into Medicaid and CHIP SCI National Meeting Albuquerque, NM Stan Dorn The Urban Institute sdorn@urban.org 202.261.5561 July 30, 2009

2
THE URBAN INSTITUTE 2 Topics to discuss I. Express Lane Eligibility (ELE) under CHIPRA II. Eligibility determination and enrollment in Massachusetts

3
THE URBAN INSTITUTE 3 Preliminary comment: CHIPRA’s new incentives to enroll eligible children If CHIP enrollment this year is low, future CHIP allocations shrink If child Medicaid enrollment grows, the state wins performance bonuses

4
THE URBAN INSTITUTE 4 Part I. Express Lane Eligibility under CHIPRA

5
THE URBAN INSTITUTE 5 Key ELE principles Basic idea: Been there, done that Don’t sweat the small stuff: ELE overlooks different eligibility methodologies Multiple uses – enrollment and renewal

6
THE URBAN INSTITUTE 6 Key limits and requirements May not use ELE to establish citizenship Immigration status OK The “Express Lane Agency,” or ELA, must give the family an opt-out notice May not use ELE to deny eligibility Reasonable time period State choice New options for “Screen and enroll” Threshold approach, 30 FPL percentage points above standard Medicaid eligibility Temporary coverage, based on the child’s likely eligibility

7
THE URBAN INSTITUTE 7 No CMS interpretation as yet But – no sanctions if the state reasonably interprets CHIPRA Key questions for CMS include: 1115 waivers to use ELE for parents Definition of “error rate” Access to enhanced FMAP for IT improvements

8
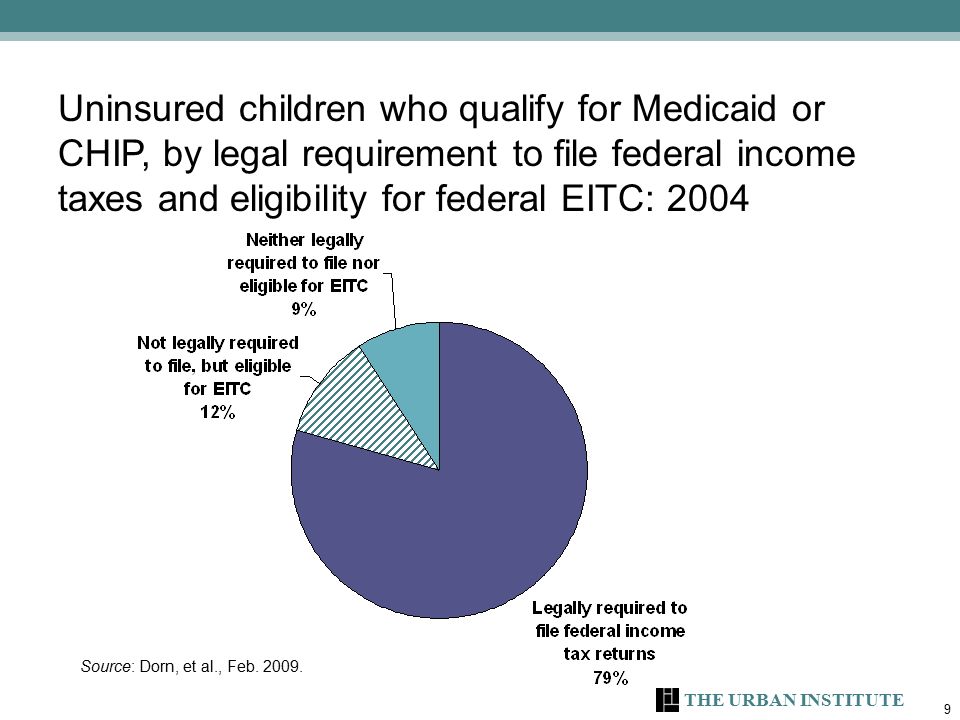
THE URBAN INSTITUTE 8 First example of ELE: state income tax forms CHIPRA specifically authorizes ELE based on gross income or adjusted gross income on state income tax returns and records

9
THE URBAN INSTITUTE 9 Uninsured children who qualify for Medicaid or CHIP, by legal requirement to file federal income taxes and eligibility for federal EITC: 2004 Source: Dorn, et al., Feb. 2009.
10
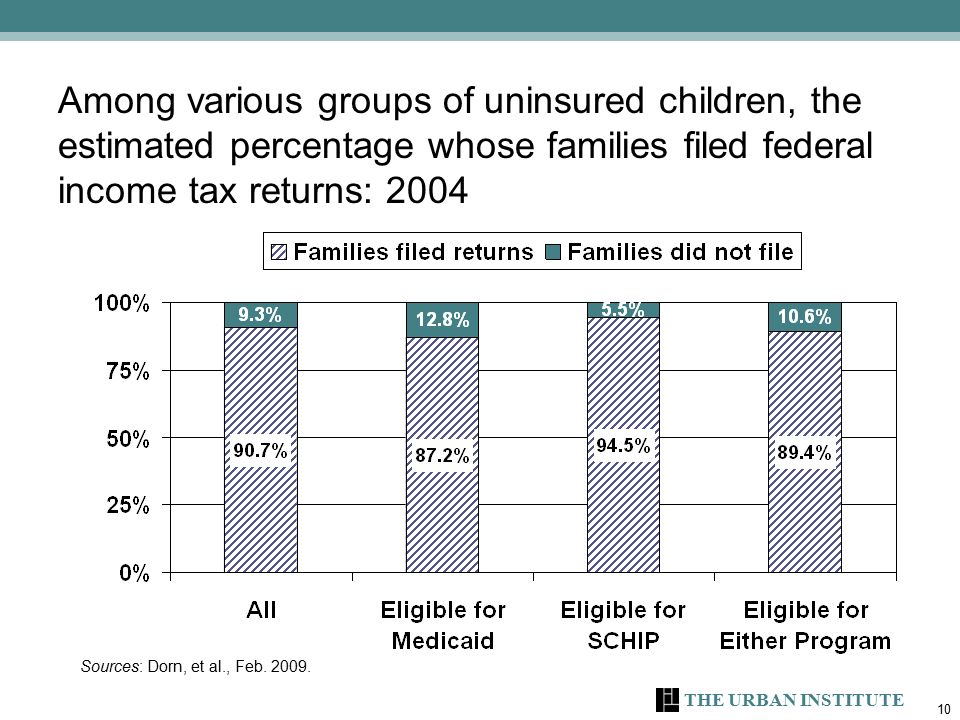
THE URBAN INSTITUTE 10 Among various groups of uninsured children, the estimated percentage whose families filed federal income tax returns: 2004 Sources: Dorn, et al., Feb. 2009.
11
THE URBAN INSTITUTE 11 What about state income taxes? Very high percentage of eligible, uninsured children. IA, MD and NJ - hundreds of thousands of children identified Consider: Minimum income threshold for required tax filing? Any refundable state income tax credits? Money withheld from paychecks?

12
THE URBAN INSTITUTE 12 How state income tax ELE could work 1. On tax form, parent taxpayers : Identify their uninsured children Can request disclosure of their tax data to the health agency Very important step. 2. Grant income-eligibility based on gross income (or AGI) and household size as shown on the income tax return 3. Qualify children as citizens based on SSA data 4. Determine immigration status for non-citizens Intensive application assistance to obtain immigration evidence Enrollment phase Presumptive eligibility (PE) Possible ELE based on SSA and SSN
 and household size as shown on the income tax return 3. Qualify children as citizens based on SSA data 4. Determine immigration status for non-citizens Intensive application assistance to obtain immigration evidence Enrollment phase Presumptive eligibility (PE) Possible ELE based on SSA and SSN.")
13
THE URBAN INSTITUTE 13 How it could work, continued 5. If child is partially but not fully eligible based on ELE, use standard methods to figure out the rest. 6. Collecting any remaining paperwork CBOs, facilitated enrollers In a managed care state, can collect documents during enrollment, using managed- care organizations (MCOs) oKey: no MCO contact with family until a plan is chosen
 oKey: no MCO contact with family until a plan is chosen.")
14
THE URBAN INSTITUTE 14 Possible adjustments Prior-year tax data CHIPRA allows – not a legal problem Ample federal precedent: Medicare Part B premium subsidies, 2008 stimulus payments, federally- subsidized college student aid For policy reasons, a state might: adjust prior-year tax information based on more recent quarterly earnings data (via IEVS or National Directory of New Hires) limit ELE if a new hire is reported or if the prior-year tax return shows significant non-W-2 income Self-employment income
 limit ELE if a new hire is reported or if the prior-year tax return shows significant non-W-2 income Self-employment income")
15
THE URBAN INSTITUTE 15 Second example of ELE: food stamps

16
THE URBAN INSTITUTE 16 Background information on food stamps Income-eligibility: Household must be at or below: 100 percent FPL in net income (using food stamp disregards); and 130 percent FPL in gross income Impact. 12.4 percent of eligible, uninsured children received food stamps in 2004. Dorn, et al., April 2009. Administrative ease. Most Medicaid agencies already have access to food stamp eligibility files. Huge efficiency gains. Almost no value is added by requiring a separate health application. < 1 percent are ineligible for Medicaid and CHIP, under standard rules for health coverage. Dorn, et al., April 2009.

17
THE URBAN INSTITUTE 17 How food stamp ELE could work 1. Identify uninsured children, by matching eligibility records 2. Send opt-out notice 3. Determine eligibility Automatically find, via ELE, that All food stamp children are income-eligible for Medicaid; All immigrant food stamp children are legally residing in the U.S., for purposes of Medicaid oMaybe not in a state with a 5-year bar for newly arrived immigrants Establish citizenship via SSA data-match See if have private coverage 4. Parents must consent before enrollment 5. Use ELE at renewal If child receives food stamps, automatically continue income-eligibility for Medicaid

18
THE URBAN INSTITUTE 18 Third example of ELE: the National School Lunch Program (NSLP)
")
19
THE URBAN INSTITUTE 19 Background information on NSLP Practical issues Matchable, centralized eligibility data in your state’s NSLP? Can you implement statewide? Or must you go district-by-district? What incentives apply to schools? Broad reach—Dorn and Kenney, 2006, found that NSLP families include: 59% of all uninsured children under 200% FPL 56% of uninsured citizen children under 200% FPL NSLP eligibility Free lunch: 130% FPL, gross income Reduced-price lunch: 185% FPL, gross income No immigration status restrictions

20
THE URBAN INSTITUTE 20 How ELE could work with NSLP 1. On NSLP application form, parents can: Identify any uninsured children; and Consent to disclose data to establish eligibility for health coverage 2. If children receive free lunches, use ELE to automatically qualify them as income-eligible for Medicaid 3. If children receive reduced-price lunches, either ELE or PE, then intensive assistance to establish ongoing eligibility 4. For anything beyond PE, need standard Medicaid/CHIP procedures to establish citizenship or legally resident status 5. Collection of remaining paperwork Can follow income tax approach

21
THE URBAN INSTITUTE 21 NSLP-recipient children, by type of NSLP benefit and income-eligibility under standard Medicaid and CHIP rules (based on audited family income) Children receiving free school lunches Children receiving reduced-price school lunches Income-eligible for Medicaid 81% 49% Income-eligible for CHIP 14% 38% Income too high for both programs 4% 13% Total:100% Source: Dorn, April 2009.
 Children receiving free school lunches Children receiving reduced-price school lunches Income-eligible for Medicaid 81% 49% Income-eligible for CHIP 14% 38% Income too high for both programs 4% 13% Total:100% Source: Dorn, April 2009.")
22
THE URBAN INSTITUTE 22 Part II. Eligibility determination and enrollment in Massachusetts Preliminary findings from a SHARE grant funded by the Robert Wood Johnson Foundation

23
THE URBAN INSTITUTE 23 Coverage expansion in Massachusetts Extraordinary results. Only 2.6 percent of state residents were uninsured in 2008 Well-known policy changes Subsidies up to 300% FPL, through Medicaid and a new program, called Commonwealth Care (CommCare) All adults mandated to purchase coverage Exception for those unable to afford coverage Health insurance exchange (the “Connector”) offers multiple private plans
 All adults mandated to purchase coverage Exception for those unable to afford coverage Health insurance exchange (the Connector ) offers multiple private plans.")
24
THE URBAN INSTITUTE 24 Net increase in the number of Massachusetts residents with health insurance, by coverage type: 6/30/06 to 9/30/08 Source: Massachusetts Division of Health Care Finance and Policy, February 2009.

25
THE URBAN INSTITUTE 25 How did Medicaid and CommCare enroll so many people? Generous subsidies, comprehensive benefits Massive PR campaign The mandate was important in getting people’s attention. Not enforced: 73% of CommCare enrollees All Medicaid adults Behavioral economics research - “avoiding a problem” motivates more than “gaining a benefit” Community-based organizations (CBOs) received $2.5-$3.5 million in annual outreach and enrollment mini-grants Long before 2006 legislation
 received $2.5-$3.5 million in annual outreach and enrollment mini-grants Long before 2006 legislation.")
26
THE URBAN INSTITUTE 26 Eligibility determination A single application form for multiple programs: Medicaid/CHIP/CommCare Uncompensated care payments to safety net hospitals and community health centers KDE instrument A single agency - Medicaid - determines eligibility for all of those programs One statewide office Logic-driven and computerized, not worker-driven Common eligibility methodologies for all programs Integrated eligibility determination prevents consumers from falling through the cracks between programs

27
THE URBAN INSTITUTE 27 Eligibility determination (continued) On-line application form (“virtual gateway”) Trained staff + computer routines=cheaper applications to process The application form must be properly completed for a hospital or clinic to get paid DSH dollars go farther State does not pay providers for this work Provider or CBO becomes the applicant’s authorized representative, copied on all eligibility-related state notices murder mystery Major efficiency gains – roughly doubled caseload while increasing state administrative staff less than 10%. But there were up-front transition costs, both financial and cultural Timing: Long before recent legislation

28
THE URBAN INSTITUTE 28 Data-driven eligibility Auto-conversion, based on free-care pool data Enrollment into MCOs: Notice of eligibility, encouraged to pick MCO Auto-assignment to MCOs, if eligible for premium- free coverage Under 100% FPL, 48,000 auto-assigned in late 2006 100-150% FPL, approximately 15,000 auto-assigned in late 2007* If an eligible consumer neither chooses nor is auto- assigned to an MCO, what happens when the consumer seeks care?

29
THE URBAN INSTITUTE 29 The effects of data-driven eligibility Huge initial impact > 80% of all CommCare enrollment by the sixth month Leverage to lower MCO premium bids Simplified enrollment by eliminating the need to complete and process application forms 100-300% FPL – 62,000 were auto-converted to CommCare. Not yet known how many chose an MCO and enrolled. Total auto-conversion: 110,000 Compared to requiring standard application forms, less costly for providers, CBOs, and state Consumers were more likely to enroll without the need to complete application forms. Fits with other state policies that encourage trained private entities to complete applications on behalf of consumers, via “virtual gateway” Rough estimate: >50% of Medicaid and CommCare enrollment comes via virtual gateway

30
THE URBAN INSTITUTE 30 Massachusetts is not paradise Government costs rose, because the formerly uninsured received subsidies. A few administrative glitches remain. For example: Churning Movement from Medicaid to CommCare. CommCare does not begin until the first of the month, but Medicaid begins and ends at any time. The state’s integrated eligibility system leaves out one program, which covers the recently unemployed. As a result, uninsured consumers eligible for subsidies sometimes go months without coverage as they move between programs. Confusion when notices come from Medicaid.

31
THE URBAN INSTITUTE 31 Conclusion Behavioral economics: many people won’t fill out forms. Not just low-income people. The classic studies involve middle-income people & 401(k) plans. ELE uses existing data to establish eligibility, eliminating the need for consumers to complete largely redundant application forms. Massachusetts: Used existing data to establish eligibility without new application forms, in many cases Safety net providers and CBOs filled out forms for consumers A single, integrated eligibility system for multiple programs simplified enrollment, often making it seamless Potential results: Increase participation Lower state administrative costs Cut red tape Prevent errors
 plans. ELE uses existing data to establish eligibility, eliminating the need for consumers to complete largely redundant application forms. Massachusetts: Used existing data to establish eligibility without new application forms, in many cases Safety net providers and CBOs filled out forms for consumers A single, integrated eligibility system for multiple programs simplified enrollment, often making it seamless Potential results: Increase participation Lower state administrative costs Cut red tape Prevent errors.")
32
THE URBAN INSTITUTE 32 Sources Express Lane Eligibility Massachusetts Stan Dorn, Express Lane Eligibility and Beyond: How Automated Enrollment Can Help Eligible Children Receive Medicaid and CHIP, prepared by the Urban Institute for the Robert Wood Johnson Foundation and the National Academy for State Healthy Policy, April 2009. Stan Dorn, Bowen Garrett, Cynthia Perry, Lisa Clemans-Cope, and Aaron Lucas, Nine in Ten: Using the Tax System to Enroll Eligible, Uninsured Children into Medicaid and SCHIP, prepared by the Urban Institute for First Focus, February 2009. Stan Dorn and Genevieve Kenney, Automatically Enrolling Eligible Children and Families Into Medicaid and CHIP: Opportunities, Obstacles, and Options For Federal Policymakers, prepared by the Economic and Social Research Institute and the Urban Institute for The Commonwealth Fund, June 2006. Massachusetts Division of Health Care Finance and Policy, Health Care in Massachusetts: Key Indicators, February 2009. Stephanie Anthony, Robert W. Seifert, Jean C. Sullivan, The MassHealth Waiver: 2009-2011…and Beyond, prepared by the Center for Health Law and Economics, University of Massachusetts Medical School, for the Massachusetts Medicaid Policy Institute and the Massachusetts Health Policy Forum, February 2009. The Massachusetts Health Insurance Connector Authority, Report to the Massachusetts Legislature: Implementation of the Health Care Reform Law, Chapter 58, 2006-2008, October 2008. Note: much of the presentation’s discussion of Massachusetts reforms is based on a site visit to Massachusetts, which was part of Urban Institute research conducted through a grant under the State Health Access Reform Evaluation program (SHARE). SHARE is funded by the Robert Wood Johnson Foundation, with the State Health Access Data Assistance Center serving as the national program office. Together with state administrative data, findings from the site visit will be published shortly.
. SHARE is funded by the Robert Wood Johnson Foundation, with the State Health Access Data Assistance Center serving as the national program office. Together with state administrative data, findings from the site visit will be published shortly..")
Similar presentations







 1.>")











