Download presentation
Presentation is loading. Please wait.

1
To fund or not to fund: A generalized decision-making model for health care resource allocation PRIORITIES 2010 The 8th Biennial Conference of the International Society on Priorities in Health Care 23-25 April 2010 Boston, USA Devidas Menon, Tania Stafinski & Christopher McCabe

2
ACKNOWLEDGEMENT This work is supported by a New Emerging Team grant on Cancer Technology Decision-making from the Canadian Institutes of Health Research

3
BACKGROUND Health services in Canada: –Federal government roles – regulatory; payment for and delivery of services to specific populations –Provincial government role – payment for and delivery of services to all residents

4
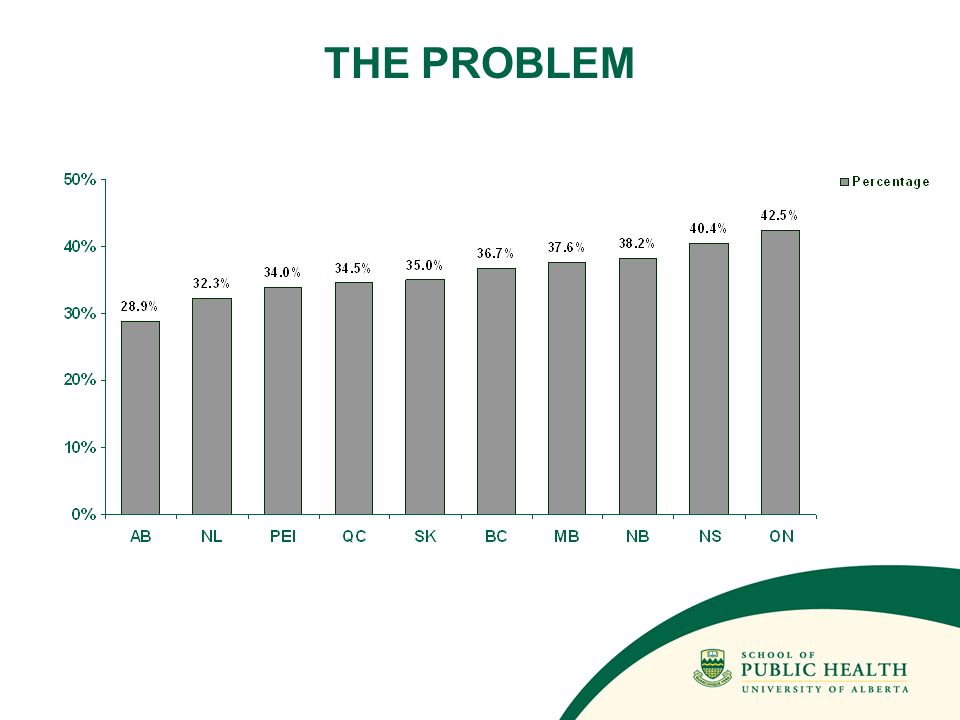
THE PROBLEM

6
THE RESEARCH PROGRAM Focuses on cancer technology decision-making in Canada Involves a joint academia-cancer care policy investigative team Involves Methodology Team, Policy Decision Team and Clinical Decision Team Has helped to build the Priorities in Cancer Care Network (PICCNet)
")
7
RESEARCH QUESTIONS What is known about existing resource allocation decision-making processes? To what extent do they depend on the focus of the decision problem? Are there common elements to these processes that might be generalisable? What value might this body of knowledge hold for cancer care decision makers in Canada?

8
METHODS Systematic review: Sources: Biomedical, health research, social sciences, economics and business bibliographic databases; HTA databases and Web of Science (1987 to 2009; monthly updated searches run); other publications by known researchers in the field; Google searches for grey literature Search terms: MeSH terms, e.g., decision making, policy making, resource allocation, health care rationing; free text terms related to new technologies or treatments, e.g., new, emerging, investigational, innovative (as title terms); terms describing aspects of decision-making, e.g., funding, coverage, reimbursement, value for money
; other publications by known researchers in the field; Google searches for grey literature Search terms: MeSH terms, e.g., decision making, policy making, resource allocation, health care rationing; free text terms related to new technologies or treatments, e.g., new, emerging, investigational, innovative (as title terms); terms describing aspects of decision-making, e.g., funding, coverage, reimbursement, value for money")
9
METHODS (cont’d.) Extraction of information: Titles and abstracts screened by project librarian for relevance Remaining results read by 2 researchers, for inclusion for review When there was disagreement about inclusion, discussion to reach agreement Full papers read by both reviewers, categorized and information extracted
 Extraction of information: Titles and abstracts screened by project librarian for relevance Remaining results read by 2 researchers, for inclusion for review When there was disagreement about inclusion, discussion to reach agreement Full papers read by both reviewers, categorized and information extracted")
10
METHODS (cont’d) Information extracted: Level of decision-making – national, provincial/state, regional or institutional Subject of the decision problem – drugs, non-drug technologies, all technologies, health services in general Committee or panel involved in the process Evidentiary requirements Decision criteria Authority of the decision-making body
 Information extracted: Level of decision-making – national, provincial/state, regional or institutional Subject of the decision problem – drugs, non-drug technologies, all technologies, health services in general Committee or panel involved in the process Evidentiary requirements Decision criteria Authority of the decision-making body")
11
METHODS (cont’d.) Development, modification & validation of a generalised decision making model: 3-element model developed – (1) the need for the decision, (2) the decision-making process itself, (3) the action taken (or to be taken) Consultation with senior cancer care decision-makers – (1) a half day meeting with decision makers from 2 provinces, (2) individual interviews with decision makers from 3 other provinces
 Development, modification & validation of a generalised decision making model: 3-element model developed – (1) the need for the decision, (2) the decision-making process itself, (3) the action taken (or to be taken) Consultation with senior cancer care decision-makers – (1) a half day meeting with decision makers from 2 provinces, (2) individual interviews with decision makers from 3 other provinces")
12
RESULTS Systematic review & extraction of information: 256 papers selected for full review (from 3500 references identified through the search); 91 selected for inclusion The need for the decision: mainly coverage or reimbursement decisions, for new technologies, with some dealing with priority setting more generally The process: Committee/panel membership varied; typically, clinicians were involved in all coverage decisions; administrators (government or institution), ethicists and methodologists in some cases; for decisions on health services more broadly, there were more perspectives included
; 91 selected for inclusion The need for the decision: mainly coverage or reimbursement decisions, for new technologies, with some dealing with priority setting more generally The process: Committee/panel membership varied; typically, clinicians were involved in all coverage decisions; administrators (government or institution), ethicists and methodologists in some cases; for decisions on health services more broadly, there were more perspectives included")
13
RESULTS (cont’d.) Some processes were quite structured, in committee composition and meeting frequency (e.g., in drug formularies), and some were ad hoc (e.g., system wide priority setting) In almost all cases, clinical efficacy or effectiveness data were required, and to a lesser extent, economic or costing analyses and quality of life measures; Evidence requirements are much more clearly defined for drugs than for other interventions or services.
 Some processes were quite structured, in committee composition and meeting frequency (e.g., in drug formularies), and some were ad hoc (e.g., system wide priority setting) In almost all cases, clinical efficacy or effectiveness data were required, and to a lesser extent, economic or costing analyses and quality of life measures; Evidence requirements are much more clearly defined for drugs than for other interventions or services.")
14
RESULTS (cont’d.) Criteria used by the committees were not detailed in most cases; factors such as equity, disease burden/clinical need, severity of illness, physician opinion, alternatives and government priorities also came into play Almost all of the committees/panels were advisory to a higher decision-making body; they make recommendations, and so other social or political factors could well influence the final decision
 Criteria used by the committees were not detailed in most cases; factors such as equity, disease burden/clinical need, severity of illness, physician opinion, alternatives and government priorities also came into play Almost all of the committees/panels were advisory to a higher decision-making body; they make recommendations, and so other social or political factors could well influence the final decision")
15
RESULTS (cont’d.) Model development: Three “components’ defined: (1) the need for a decision, (2) The decision process itself, (3) the action as a result Each of the components was built on the basis of information from the literature synthesis; in each component, the model prescribes a set of questions (based on literature) which could address the requirements of a specific organisation or decision making body.
 Model development: Three components’ defined: (1) the need for a decision, (2) The decision process itself, (3) the action as a result Each of the components was built on the basis of information from the literature synthesis; in each component, the model prescribes a set of questions (based on literature) which could address the requirements of a specific organisation or decision making body.")
16
1. Need for a decision is identified a. What type of decision is this? ( coverage/reimbursement, disinvestment, distributional, evaluation, etc.) b. Why is the decision needed at this time? (one-off request, program review, budget preparation, regular committee schedule, cost-containment, cost- reduction, etc.) c. Who needs to make the decision? (cancer board/agency, provincial government, health authority, etc.) d. Who needs to be consulted? (physicians, patients, industry, administrators, other provinces, etc.) e. Who needs to be managed? (professional associations, patient advocacy groups, industry, media, etc.) 2. Decision-making process takes place a. Are there any ethics/values frameworks or statements of social values that guide decisions made by the organization? (equity, solidarity, distributive justice, utilitarianism, cost- containment, “accountability for reasonableness”, rule of rescue, ethical taskforce guidelines, etc.) b. Who is the decision-making group? (cancer board/agency executive or committee, provincial government executive or committee, hospital executive or committee, health authority executive or committee, etc.) c. What types of information are needed? (prevalence/incidence/burden, clinical, economic, system requirements (e.g., human resource, organizational, etc.), “situational”, status in other jurisdictions, etc.) d. What criteria, factors, or values need to be included in deliberations? (disease burden, clinical effectiveness, cost- effectiveness, budget impact, affordability, availability of alternatives, feasibility, patient preference, etc.) e. How have the individual effects of the technology/service been measured? (systematic reviews, RCTs, other controlled trials, registries, economic analyses, etc.) f. What tools may be used to aggregate the above findings? (checklists, balance sheets, cost/QALY thresholds, ranking exercises, etc.) g. What mechanisms may be employed to manage appeals to recommendations before a decision is made? 3. Action taken a. What decision options are available? (do nothing, defer, fund partially, fund conditionally, fund fully, etc.) b. What other steps need to be considered? (monitoring of technology or service diffusion, planned re- evaluation or review, etc.) c. What mechanisms may be employed to manage appeals to decisions? Overarching ethical frameworks/principles or social values Appeals mechanisms?
 b. Why is the decision needed at this time. (one-off request, program review, budget preparation, regular committee schedule, cost-containment, cost- reduction, etc.) c. Who needs to make the decision. (cancer board/agency, provincial government, health authority, etc.) d. Who needs to be consulted. (physicians, patients, industry, administrators, other provinces, etc.) e. Who needs to be managed. (professional associations, patient advocacy groups, industry, media, etc.) 2. Decision-making process takes place a. Are there any ethics/values frameworks or statements of social values that guide decisions made by the organization. (equity, solidarity, distributive justice, utilitarianism, cost- containment, accountability for reasonableness , rule of rescue, ethical taskforce guidelines, etc.) b. Who is the decision-making group. (cancer board/agency executive or committee, provincial government executive or committee, hospital executive or committee, health authority executive or committee, etc.) c. What types of information are needed. (prevalence/incidence/burden, clinical, economic, system requirements (e.g., human resource, organizational, etc.), situational , status in other jurisdictions, etc.) d. What criteria, factors, or values need to be included in deliberations. (disease burden, clinical effectiveness, cost- effectiveness, budget impact, affordability, availability of alternatives, feasibility, patient preference, etc.) e. How have the individual effects of the technology/service been measured. (systematic reviews, RCTs, other controlled trials, registries, economic analyses, etc.) f. What tools may be used to aggregate the above findings. (checklists, balance sheets, cost/QALY thresholds, ranking exercises, etc.) g. What mechanisms may be employed to manage appeals to recommendations before a decision is made. 3. Action taken a. What decision options are available. (do nothing, defer, fund partially, fund conditionally, fund fully, etc.) b. What other steps need to be considered. (monitoring of technology or service diffusion, planned re- evaluation or review, etc.) c. What mechanisms may be employed to manage appeals to decisions. Overarching ethical frameworks/principles or social values Appeals mechanisms .")
17
RESULTS (cont’d.) Consultation/validation of model: Agreement with the 3 components in a general sense, but some additional points raised: There are numerous different influences and perspectives that enter decision-making in health care Determination of whose or what “values” ought to be considered during the process is a challenge The overarching ethical principles, perhaps embodied in an organization’s vision and mission are important for this process As health care decisions have the potential of impacting diverse groups, it is important to identify these, and how they are to be managed or involved during the process Appeal mechanisms should be available, but this might happen either at the recommendation stage or the decision stage (depending on the authority) Disinvestment of existing technologies to accommodate new ones appears to be an increasingly important consideration
 Consultation/validation of model: Agreement with the 3 components in a general sense, but some additional points raised: There are numerous different influences and perspectives that enter decision-making in health care Determination of whose or what values ought to be considered during the process is a challenge The overarching ethical principles, perhaps embodied in an organization’s vision and mission are important for this process As health care decisions have the potential of impacting diverse groups, it is important to identify these, and how they are to be managed or involved during the process Appeal mechanisms should be available, but this might happen either at the recommendation stage or the decision stage (depending on the authority) Disinvestment of existing technologies to accommodate new ones appears to be an increasingly important consideration")
Similar presentations


 Care in Alberta Alberta Health Services.>")
















