Download presentation
Presentation is loading. Please wait.

1
CML

4
Stem cell disorder Characterized by myeloproliferation Well-described clinical course 9 9q+ 22 Ph 22q- BCR ABL BCR ABL Translocation Transcription and translation Inhibition by TKI BCR-ABL fusion protein CML Constitutive tyrosine kinase Phosphorylation of multiple substrates Mitogenic signaling and genomic instability increased Apoptosis and stromal regulation decreased

5
*Clonal myeloproliferative disorder resulting from neoplastic transformation of pluripotent stem cells (affect myeloid, erythroid & megakaryocytic lineages) * proliferation, apoptosis *Cytogenetic hallmark: Ph chromosome positivity
 * proliferation, apoptosis *Cytogenetic hallmark: Ph chromosome positivity")
6
*7% to 15% of all adult leukemias (5 th leukemia in USA) *Median age at diagnosis: 55 years (20% to 30% of patients ≥ 60 years)
 *Median age at diagnosis: 55 years (20% to 30% of patients ≥ 60 years)")
8
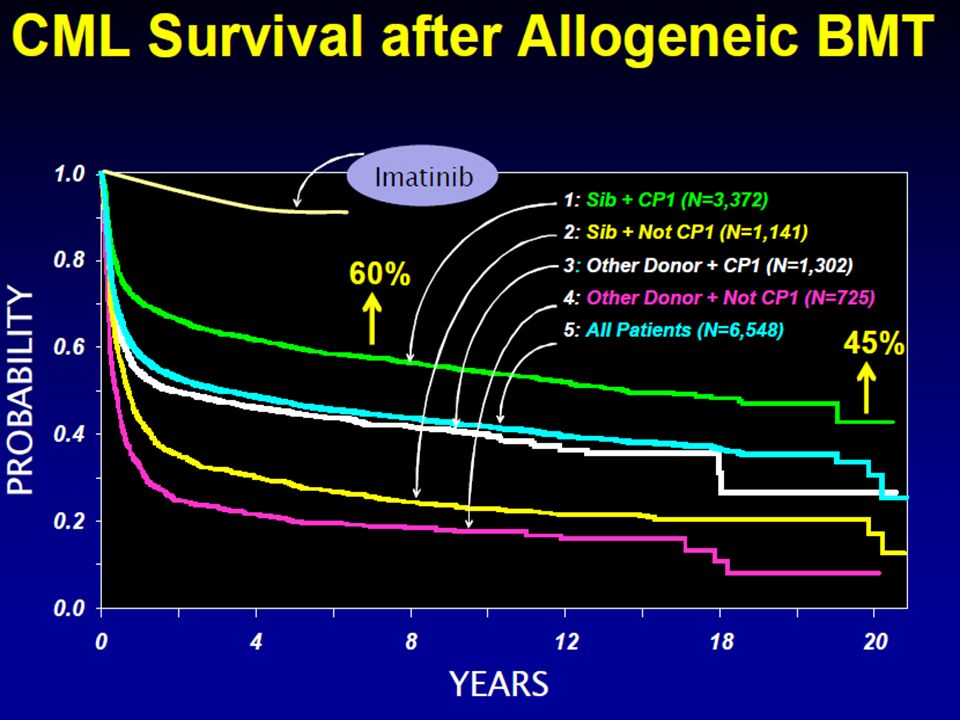
*Fatal disorder with poor prognosis *Median survival: 3-5 years (2 years without treatment) *Allogeneic SCT curative in 40% to 70% of patients (Associated with mortality and toxicity) *Interferon alfa ± cytarabine: CCyR of 20% to 30% Median survival: 6-7 years Also associated with adverse events *Other options: hydroxyurea, busulfan
 *Allogeneic SCT curative in 40% to 70% of patients (Associated with mortality and toxicity) *Interferon alfa ± cytarabine: CCyR of 20% to 30% Median survival: 6-7 years Also associated with adverse events *Other options: hydroxyurea, busulfan")
9
* The exact cause is not found * Pathogenesis is well established with consequences on treatment & prognosis *Possible association with ionizing radiation & exposure to industrial benzene

10
Asymptomatic – accidentally discovered on routine CBC Anemia – easy fatigability, malaise, shortness of breath, chest pain, palpitation High metabolic rate - weight loss, fever Lt hypochondrial discomfort, easy satiety Bleeding- skin ecchymoses, bruises, petechiae UGI ulceration & bleeding (↑ s histamine due to basophilia) Thrombosis – thrombocytosis, leukocytosis Headache, bone pain, gouty arthritis, leukostasis, priapism
 Thrombosis – thrombocytosis, leukocytosis Headache, bone pain, gouty arthritis, leukostasis, priapism")
11
Pallor, cutaneous bleeding, splenomegaly (one of the largest spleens) No lymphadenopathy Fever Weight Loss Hepatomegaly – less common than splenomegaly
 No lymphadenopathy Fever Weight Loss Hepatomegaly – less common than splenomegaly")
12
*85% of patients diagnosed with chronic-phase CML *50% of patients asymptomatic Symptomatic patients exhibit Constitutional symptoms Left upper quadrant discomfort Early satiety purpura,Splenomegaly, hepatomegaly

13
1- Benign Phase – in which the disease behavior & response is predictable(Stable phase) 2- Accelerated phase – tumor burden increases rapidly with more systemic symptoms & increasing difficulty in control of disease 3- Acute phase – Blastic crisis may be AML,ALL, AUL Patient may present in accelerated or acute phase for the first time
 2- Accelerated phase – tumor burden increases rapidly with more systemic symptoms & increasing difficulty in control of disease 3- Acute phase – Blastic crisis may be AML,ALL, AUL Patient may present in accelerated or acute phase for the first time")
14
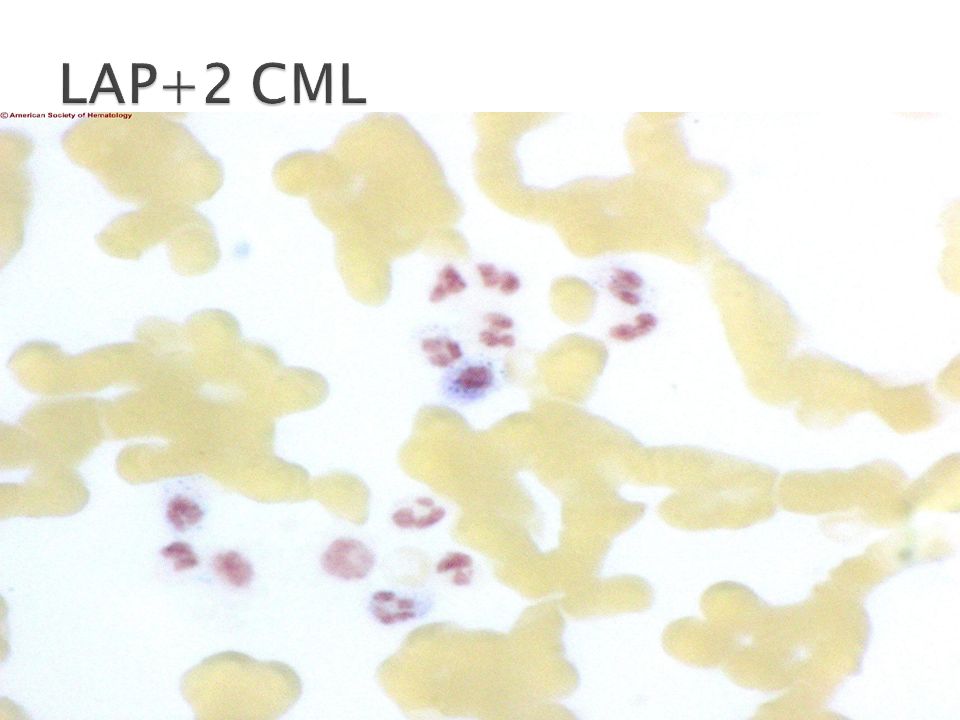
CBC- Hb↓, PCV↓, WBC↑ > 10000/µl Differential count – Neutrophilic leukocytosis different stages seen (blasts, promyelocytes, myelocytes, metamyelocytes, stab or band forms), eosinophilia, basophilia Thrombocytosis or thrombocytopenia LAP score ↓ or absent STC I, III ↑, SLDH↑, S histamine↑, S uric acid↑
, eosinophilia, basophilia Thrombocytosis or thrombocytopenia LAP score ↓ or absent STC I, III ↑, SLDH↑, S histamine↑, S uric acid↑")
15
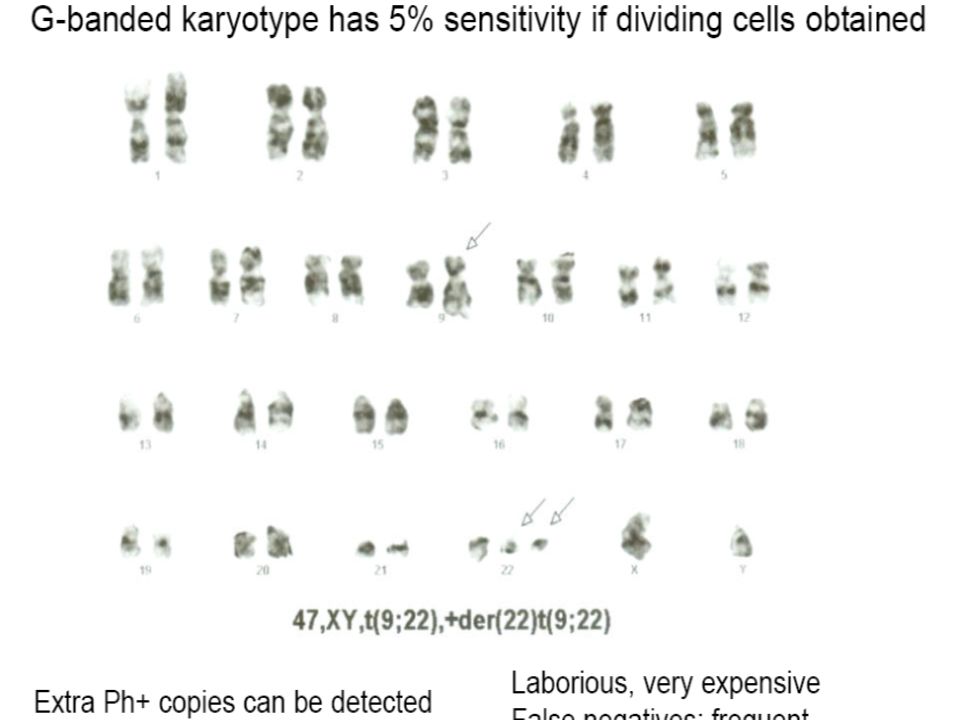
Bone Marrow Aspirate & Biopsy- hypercellular, devoid of fat, myeloid hyperplasia, ↑retculin or collagen fibers, M:E ratio 15-20:1 Cytogenetics- Philadelphia chromosome positivity 95% (Ph –ve 5%) shortened long arm of chromosome22 Molecular biology- BCR/ABL gene positive
 shortened long arm of chromosome22 Molecular biology- BCR/ABL gene positive")
21
* Balanced reciprocal translocation between chromosome 22 & chromosome 9 [t(9;22)] that brings BCR gene in juxtaposition with ABL gene forming a new hybrid gene BCR/ABL that codes for synthesis of a chimeric protein P210 that shows tyrosine kinase activity causing uncontrolled proliferation of the malignant clone
![* Balanced reciprocal translocation between chromosome 22 & chromosome 9 [t(9;22)] that brings BCR gene in juxtaposition with ABL gene forming a new hybrid gene BCR/ABL that codes for synthesis of a chimeric protein P210 that shows tyrosine kinase activity causing uncontrolled proliferation of the malignant clone](http://images.slideplayer.com/24/7510515/slides/slide_21.jpg "* Balanced reciprocal translocation between chromosome 22 & chromosome 9 [t(9;22)] that brings BCR gene in juxtaposition with ABL gene forming a new hybrid gene BCR/ABL that codes for synthesis of a chimeric protein P210 that shows tyrosine kinase activity causing uncontrolled proliferation of the malignant clone")
23
1- Leukemoid reaction rarely WBC count exceeds 30000, not clonal, BM no blasts excess, seen in overwhelming sepsis & disseminated TB. 2- MDS – CMML stage. 3- chronic corticosteroids use (demargination). 4- other MPD.
. 4- other MPD..")
26
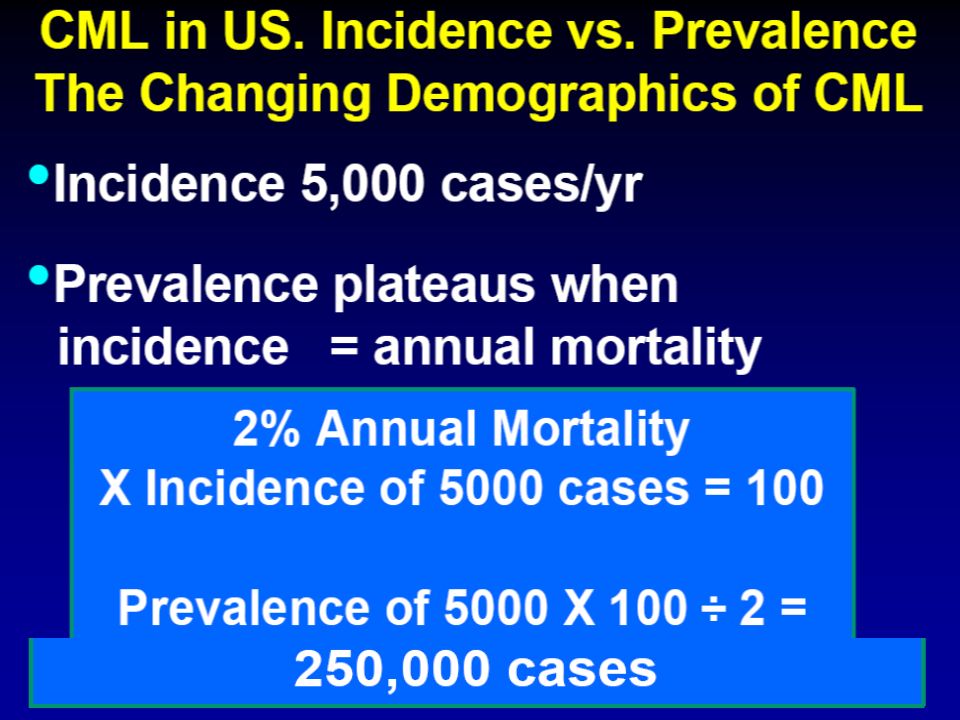
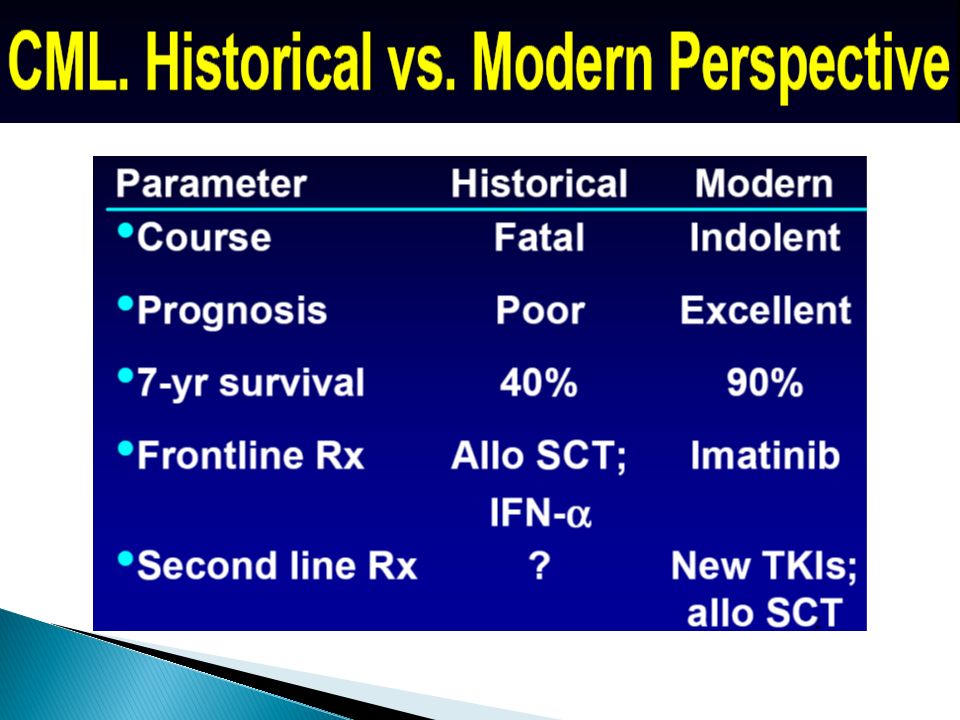
ParameterHistorical Perspective (Until 2000) Modern Perspective (Since 2000) CourseFatalIndolent PrognosisPoorExcellent Median survival, yrs3-6≥ 25* Frontline treatmentAllogeneic SCT, interferon alfa Imatinib Second-line treatmentNot establishedAllogeneic SCT, novel TKIs
 Modern Perspective (Since 2000) CourseFatalIndolent PrognosisPoorExcellent Median survival, yrs3-6≥ 25* Frontline treatmentAllogeneic SCT, interferon alfa Imatinib Second-line treatmentNot establishedAllogeneic SCT, novel TKIs")
27
Targeted Therapy- 1- Imatinib mesylate 400 mg/d - TKI targets the pathogenetic mechanism - revolutionized treatment causing CCyR & CMR S/E skin rash, edema, myelosuppression, hepatitis 2- Dasatinib & Nilotinib 2 nd line for imatinib failure or hypersensitivity 3- high dose imatinib 600-800 mg/d

28
* BMT when enter accelerated phase prior to acute phase * Interferon-α + cytosine arabinoside * Hydroxyurea orally * Busulfan (myleran) orally – no more used now because of severe & protracted myelosuppression
 orally – no more used now because of severe & protracted myelosuppression")
29
1- Allopurinol 2- H-2 blockers 3- PPI 4- Blood transfusion 5- platelet transfusion

30
It was an inevitably fatal disease With recent treatment became a curable disease compatible with long survival Newer agents are evolving Improving BMT &SCT results Once the patient enters the acute phase the only hope remains in transplantation & TKI are used as bridging to that

31
Poor Prognostic Factors in CML Older age Splenomegaly Anemia Thrombocytosis, thrombocytopenia Blasts, promyelocytes, basophils Marrow fibrosis Cytogenetic clonal evolution (Euro), MDACC Prognostic Models: Sokal, Hasford
, MDACC Prognostic Models: Sokal, Hasford")
Similar presentations




































 Myelodysplastic / myeloproliferative diseases (MDS/MPD) >")

:>")
 leukemia Is characterized by an unregulated proliferation of myeloid elements in the bone marrow,>")





