Download presentation
Presentation is loading. Please wait.

1
Transforming Government using Open Standards Jagdip Grewal Chief Technical Architect 29 th October 2007

2
Agenda Business Context Enterprise Architecture Context Services in an Enterprise Architecture Using standards to enable integrated healthcare Integration challenges UK Government Enterprise Architecture

3
To deliver a 21 st century health service through efficient use of technology to: Enable and improve Access and Choice Enable care pathways and patient focus Improve accuracy in treatment Create opportunities for improved efficiency Create opportunities for real NHS reform Our Objectives

4
Ageing Population 2001 – over 60s > than under 18s 2050 – 4 times as many needing care At 4 times the current cost …while the number available as carers declines Demographic Challenge

5
Life expectancy increased to 75 years 9 million people over 65 and increasing Population more mobile Greater long term chronic illness Patients more educated on health and want greater involvement 1,200 Patients dying each year from medication errors 5,000 procedures cancelled each year 5% of patient safety incidents due to documentation errors Has overburdened the system The NHS in 2002 Patient records held on paper Highly variable usage of IT Lots of home-grown specialist systems Continuing reliance on 1970s mainframes A Changing Health Environment 1 The need for change

6
Local procurement of IS/IT Systems by GPs, Trusts etc Disparate Technologies, 1000s of suppliers Limited data sharing Lack of standardisation Lots of paper Little leverage of NHS buying power Challenges

7
National Programme for IT Launched Spring 2002 by “21 st Century IT” policy document Mobilisation from Q1 2003 Procurement completed Q1 2004 ‘Services’ based contracts Local and National Suppliers £6bn of IT services contracted over ten years The answer…

8
Largest civil IT project in the world 40,000 GPs 80,000 other doctors 350,000 nurses 300+ hospitals 10 year programme 50m+ patients 1.344m healthcare workers chooseandbook Electronic Prescriptions Service NHSmail National & Local Care Record Services Healthspace Picture Archiving & Communications Service Secure E-mail for all NHS workers Web Access for Patients Secondary Uses Service Analysing National Health Trends New National Network Patient Choice Scope N3

9
…and what does it look like 120 Different Supplier Accredited Systems to integrate 3 Suppliers with differing Architectures Multiple and Disparate Channels Integration required with set of common services

10
Programme Challenges Hundreds of different applications and suppliers Large scale systems e.g. Prescriptions at 500tps End Users with differing requirements and geographically distributed Diverse (often ‘legacy’) Supplier Technologies Lack of Standards Desire to Use COTS packages – avoid bespoke Evolution in requirements and functionality Data availability, quality and integrity is critical Enterprise Architecture required to define overall End to End approach
 Supplier Technologies Lack of Standards Desire to Use COTS packages – avoid bespoke Evolution in requirements and functionality Data availability, quality and integrity is critical Enterprise Architecture required to define overall End to End approach.")
11
Agenda Business Context Enterprise Architecture Context Services in an Enterprise Architecture Using standards to enable integrated healthcare Integration challenges UK Government Enterprise Architecture

12
Business Services IS Services Technology Services Enterprise Architecture EA - Context Policy NASP NHS CFH Medical Advances Patient Demand LSP/ESP We may all have different perspectives but we can make our lives much easier by ‘talking’ the same language. Clinical Processes Outcomes Better Patient Care Reduced Cost Lower waiting Times

13
The bigger picture - In support of traceability (simplified view)
")
14
NHS – relationship map

15
Agenda Business Context Enterprise Architecture Context Services in an Enterprise Architecture Using standards to enable integrated healthcare Integration challenges UK Government Enterprise Architecture

16
Enterprise Architecture – Domain View

17
Conceptual Services: what we do

18
E.g. Demographics Within local Services Domain Set of services required to be implemented by local systems Within Enterprise Services Domain Set of services required to be implemented by national service provider for all 60m patients Set of compliance docs from NHS CFH Covering requirements to be met by systems implementing those services MIM for message definitions and example process flows Principles - loose coupling, search local first, update local first What is to be tested and verified during integration testing

19
Logical Applications…

20
Agenda Business Context Enterprise Architecture Context Services in an Enterprise Architecture Using standards to enable integrated healthcare Integration challenges UK Government Enterprise Architecture

21
The role for standards Explicit from the outset. The standards base evolves and grows Standards chosen to maximise interoperability and to meet different integration requirements Use of ebXML, (https, SOAP, XML) - reliable asynchronous messaging for patient demographic updates Web Services and WS standards e.g. WS-A – lightweight synchronous messaging for patient demographic queries Use of SNOMED CT Use of HL7 v3 (ETP, C&B, PDS) and CDA v2 (Clinical Documents) Lots more…. Objective is to federate the design responsibility to the systems providers, working within a framework of standards and specifications
 - reliable asynchronous messaging for patient demographic updates Web Services and WS standards e.g. WS-A – lightweight synchronous messaging for patient demographic queries Use of SNOMED CT Use of HL7 v3 (ETP, C&B, PDS) and CDA v2 (Clinical Documents) Lots more…. Objective is to federate the design responsibility to the systems providers, working within a framework of standards and specifications.")
22
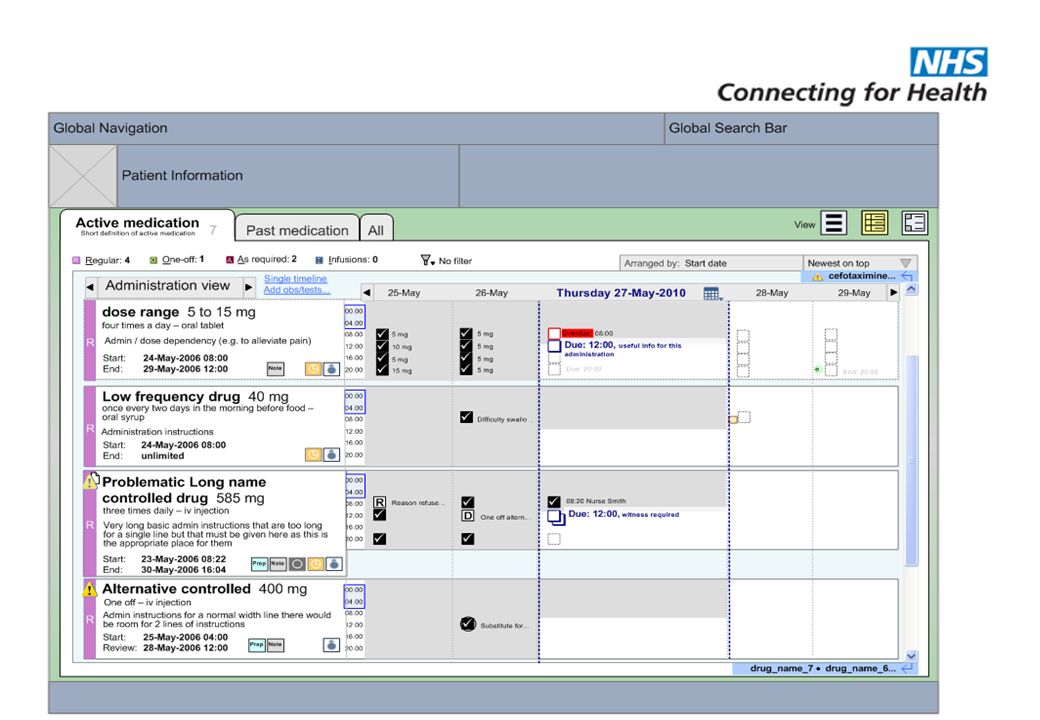
Not just technical standards Common User Interface (CUI) - Microsoft and NHS CFH (http://www.mscui.org/) Knowledge authorship to allow Knowledge Support (KBS) and Decision Support into all aspects of the implementation The International Health Terminology Standards Development Organisation SNOMED CT Charter Members (Australia, Canada, Denmark, Lithuania, New Zealand, United Kingdom United States) A drug database – The Dictionary of Medication and Devices (dm+d) Standards by which we accredit systems as safe to implement and exchange information
 - Microsoft and NHS CFH ( Knowledge authorship to allow Knowledge Support (KBS) and Decision Support into all aspects of the implementation The International Health Terminology Standards Development Organisation SNOMED CT Charter Members (Australia, Canada, Denmark, Lithuania, New Zealand, United Kingdom United States) A drug database – The Dictionary of Medication and Devices (dm+d) Standards by which we accredit systems as safe to implement and exchange information")
25
Elective / Passive Decision Support – same component in all local solutions

26
Standard drug dictionary A standard drug dictionary for all systems We (and Australia) have chosen to make and maintain a new one called dm+d (The dictionary of medications and devices) NB. This is NOT decision support but a standard way of naming and structuring medication and devices so that decision support and complex rules based content can be added with predictable results.

27
Atenolol 50mg Tablet x28 (VMPP) Atenolol 50mg Tablet (COX) (AMP) Atenolol 50mg Tablet (Cox) X28 (AMPP ) Atenolol 50mg Tablet (VMP) Atenolol (drug product) (VTM) Cardioselective beta-blocker IS_A Beta-blocker drug IS_A etc IS_A Snomed CT drug core NHS dm+d Dm+d and SNOMED CT (300,000 terms) Both dm+d and SNOMED have a central core with local additions
 Atenolol 50mg Tablet (COX) (AMP) Atenolol 50mg Tablet (Cox) X28 (AMPP ) Atenolol 50mg Tablet (VMP) Atenolol (drug product) (VTM) Cardioselective beta-blocker IS_A Beta-blocker drug IS_A etc IS_A Snomed CT drug core NHS dm+d Dm+d and SNOMED CT (300,000 terms) Both dm+d and SNOMED have a central core with local additions")
28
Standards enable supplier expansion The use of Open Standards for integration (ebXML, HL7) has enabled an expansion in number of suppliers to the programme Leverages existing knowledge capital and established standards Allows suppliers to build COTS packages based upon industry standards. Move away of bespoke development Allows plug and play of new services Standardisation reduces overall testing complexity To meet business objectives we have integrated 100s of supplier applications Access from private corporate WAN (N3) as well as internet aggregators for high street access
 as well as internet aggregators for high street access.")
29
What have we achieved so far? … - some “numbers” (at 08/10/07) 17,454 instances of systems connected into the national services which allows in a typical day 190,000 prescription messages issued electronically (18% of all prescriptions) 19,000 Choose and Book electronic bookings 1,400,000 queries to be recorded on the patient demographic system enabling letters to be posted to the correct address and patient information to be handled more efficiently These are deployed via the 20,662 connections to N3 (the national NHS WAN) 380,350,622 images have been stored using PACS from NHS CFH There are 394,367 Smartcard holders who are registered and approved for access to systems
 17,454 instances of systems connected into the national services which allows in a typical day 190,000 prescription messages issued electronically (18% of all prescriptions) 19,000 Choose and Book electronic bookings 1,400,000 queries to be recorded on the patient demographic system enabling letters to be posted to the correct address and patient information to be handled more efficiently These are deployed via the 20,662 connections to N3 (the national NHS WAN) 380,350,622 images have been stored using PACS from NHS CFH There are 394,367 Smartcard holders who are registered and approved for access to systems.")
30
Acute System Patient info Broken Leg Patient visits Emergency Dept Emergency Dept Discharge GP System Back Pain Patient visits GP Acute System Patient info Chest infection Patient visits hospital Summary Care Record What’s next - more clinical Information flows between systems Enabled by standards (HL7v3 and HL7 CDA v2 over ebXML (https/SOAP/XML) and central messaging services (TMS) Update GP Summary Emergency Dept Discharge Discharge
 and central messaging services (TMS) Update GP Summary Emergency Dept Discharge Discharge")
31
Agenda Business Context Enterprise Architecture Context Services in an Enterprise Architecture Using standards to enable integrated healthcare Integration challenges UK Government Enterprise Architecture

32
Integration – The Challenges Large number of suppliers – and growing Each supplier footprint is different & can consume different services Suppliers in different phases of development Business critical services – cannot be stopped for more than a few hours We cannot ‘lose’ data Data must only flow from accredited applications running from authorised endpoints originating from users with the relevant roles Large numbers of endpoints, systems and users Strict Information Governance Rules

33
Challenges – Service Definition Right Granularity ? To high and they are subject to constant change. To Low and it can result in significant increases in message flow. Generic or Specific business process ? The level of business logic can impact the re-usability of the service. What SLAs ? Services that are used for many business functions may have varying SLA needs – these must be balanced against cost Trade off between performance and extensibility What security model ? Whilst some aspects of information security can be centralised – others must be federated

34
Challenges – Compatibility FORWARD and BACKWARD A change to a service can impact many applications and suppliers -Each system needs to be fully tested before it is accredited for deployment !!! The more ‘versions’ we support the less scope we have to add new capabilities Translation services are required to accommodate supplier applications running at different versions

35
Services usage can be different to expectation All local systems will integrate with Summary Care Record SCR provides a set of services to enable this in different ways Summary Care Record CSA Request Response ESP On-demand … Request Response LSP Pre-fetch Request Response

36
Agenda Business Context Enterprise Architecture Context Services in an Enterprise Architecture Using standards to enable integrated healthcare Integration challenges UK Government Enterprise Architecture

37
Cross Government Enterprise Architecture CTO Council formed in Sept 2005. The aim is to support the CIO Council through the optimisation of the use of IT resources across the public sector. Strategic value of xGEA is to identify opportunities for collaboration and reuse across government. Without a business and IT Blueprint for Government – an Enterprise Architecture – avoidable cost would be incurred as IT is developed in ‘islands.’

38
So where do the CTO Council sit?

39
xGOV EA Domains and Leads CHANNEL DOMAIN Terry Hawes (HMRC) INFRASTRUCTURE DOMAIN Andrew Bull (HMRC) APPLICATION DOMAIN TBD PROCESS DOMAIN John Wailing (Home Office) INFORMATION DOMAIN Pete Desmond (DWP) STRATEGY Andrew Stott (Cabinet Office) SERVICES MANAGEMENT DOMAIN Paul McAvoy (DWP) INTEGRATION DOMAIN Inderjit Singh (NHS CfH) INFORMATION ASSURANCE DOMAIN Marc Hocking (Cabinet Office)
 INFRASTRUCTURE DOMAIN Andrew Bull (HMRC) APPLICATION DOMAIN TBD PROCESS DOMAIN John Wailing (Home Office) INFORMATION DOMAIN Pete Desmond (DWP) STRATEGY Andrew Stott (Cabinet Office) SERVICES MANAGEMENT DOMAIN Paul McAvoy (DWP) INTEGRATION DOMAIN Inderjit Singh (NHS CfH) INFORMATION ASSURANCE DOMAIN Marc Hocking (Cabinet Office)")
40
xGov EA Context The majority of the work of the CTO council is structured around the xGov EA through the Domain Teams. The Domain Team leads collectively form the Architecture Review Board (ARB) whose purpose is to: Oversee the development of cross-Government Enterprise Architecture – xGEA Oversee the development and operation of the clearing house process for exemplars Assesses the fitness for purpose of proposed exemplars (managed services and solutions) for reuse across the public sector Resolves overlaps between domains Provides a forum for peer reviews
 whose purpose is to: Oversee the development of cross-Government Enterprise Architecture – xGEA Oversee the development and operation of the clearing house process for exemplars Assesses the fitness for purpose of proposed exemplars (managed services and solutions) for reuse across the public sector Resolves overlaps between domains Provides a forum for peer reviews.")
41
Capturing EXEMPLARS at various levels A hosted service that is offered to others A packaged service including: code, design that can be rebuilt The approach to providing the service Experiences gained implementing the service

42
Clearing House Process and Domain ToR Detailed Process Flow Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Entry Viability Definition Design Business Justification Build Go Live Benefits Generate Idea Test Feasibility Define Proposition Design Service Complete business case Build Service Live Running Test Service Define Idea Match Reqs Reuse & Identify New Harvest to Exemplar Organisations’ Architecture Team Interface Process Domain Teams Clearing House ARB CTO Council Future / WIPExisting Delivery and Transformation Group Business Idea X Architecture Priority : 1 CIO Gate Status: Viability Primary Domain : Infrastructure Secondary Domain : Channels Business Idea X Architecture Priority : 1 CIO Gate Status : Viability Primary Domain : Infrastructure Secondary Domain : Channels Check keywords against ‘Metadata’ Exemplar Exist Record as WIP Re-use as-is Enhance and re-use Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Re-used Business ‘artefact’ eRoom
 Architecture Team Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Entry Viability Definition Design Business Justification Build Go Live Benefits Generate Idea Test Feasibility Define Proposition Design Service Complete business case Build Service Live Running Test Service Define Idea Match Reqs Reuse & Identify New Harvest to Exemplar Organisations’ Architecture Team Interface Process Domain Teams Clearing House ARB CTO Council Future / WIPExisting Delivery and Transformation Group Business Idea X Architecture Priority : 1 CIO Gate Status: Viability Primary Domain : Infrastructure Secondary Domain : Channels Business Idea X Architecture Priority : 1 CIO Gate Status : Viability Primary Domain : Infrastructure Secondary Domain : Channels Check keywords against ‘Metadata’ Exemplar Exist Record as WIP Re-use as-is Enhance and re-use Organisation Organisations’ (Technical) Architecture Team Organisation Organisations’ (Technical) Architecture Team Re-used Business ‘artefact’ eRoom")
43
Summary Use a service based Enterprise Architecture to enable a common language Set standards and frameworks that permit increasing levels of interoperability and interaction across multiple suppliers Be aware of the challenges of integrating multiple suppliers

Similar presentations







 Knowledge Council Workstreams and the CTO Council Domains www.nglis.org.uk/tipshome.htm.>")












