Download presentation
Presentation is loading. Please wait.

1
Ninh T. Nguyen, MD Professor of Surgery Division of GI Surgery University of California, Irvine Medical Center Gastric Plication: Is it Ready for Prime Time? Con

2
Disclosure Slide Disclosure Slide Ninh T. Nguyen CovidienGrant/speaker GoreSpeaker SurgiquestConsultant EthiconSpeaker

3
Why Gastric Plication is not Ready for Prime Time! Lack of scientific rationale Lack of data No evidence for metabolic effect Not recognized by ASMBS

4
Why Gastric Plication is not Ready for Prime Time! Lack of scientific rationale Lack of data No evidence for metabolic effect Not recognized by ASMBS

5
Rationale for Gastric Plication? Improve weight loss and resolution of comorbidities?

6
Rationale for Gastric Plication? Minimize complication associated with sleeve gastrectomy

7
Rationale for Gastric Plication?

8
Complications of Sleeve Gastrectomy Bleeding Leaks Obstruction

9
Complications after Gastric Plication 135 pts underwent LGCP GI bleeding (1.5%) leaks (1.5%) Acute gastric obstruction (2.2%) Skrekas et al. Obes Surg 2011

10
Complications after Gastric Plication 100 pts underwent LGCP 3 yr, 57% EWL (n=11) for GCP Obstruction requiring reop (1%) Leaks (2%) Talebpour et al. J Laparoendosc Adv Surg Tech 2007

11
Complications after Gastric Plication 15 pts underwent LGCP 1 yr, 53% EWL (n=6) for GCP Acute gastric obstruction requiring reop (16.6%) Brethauer et al. SOARD 2011

12
Ideal Bariatric Operation Low morbidity & low mortality (risks) Good efficacy (benefits) Reproducible Low revisional rate
 Good efficacy (benefits) Reproducible Low revisional rate")
13
Issues with Gastric Plication for Widespread Acceptance Variability in technique & not easily reproducible - Small margin for error (too small vs too large) Doesn’t appear to reduces perioperative complications Complicated for revisional
 Doesn’t appear to reduces perioperative complications Complicated for revisional")
14
Why Gastric Plication is not Ready for Prime Time! Lack of scientific rationale Lack of data No evidence for metabolic effect Not recognized by ASMBS

15
Accumulating Data Perform under institutional IRB Courses on procedure should only be held specifically for investigators planning to participate in a multicenter trials of the new procedure Publish data for peer-review

16
Sleeve Gastrectomy as bariatric Procedure CIC of ASMBS First stage to reduce surgical risk 775 patients (15 reports) Single study with 3-year follow-up %EWL 33-83%, mortality: 0.39% The ASMBS recognizes sleeve may be an option for selected patients, particularly high-risk or super obese as a risk reduction strategy SOARD 2007
 Single study with 3-year follow-up %EWL 33-83%, mortality: 0.39% The ASMBS recognizes sleeve may be an option for selected patients, particularly high-risk or super obese as a risk reduction strategy SOARD 2007")
17
Updated Position Statement on Sleeve Gastrectomy as bariatric Procedure Overall 36 studies (2570 patients) - Primary procedure, 24 studies (1749 patients) For primary procedure, follow-up 3-36 mos., 60.6% EWL Conclusions: - Long-term data remain limited - ASMBS accepted SG as an approved bariatric procedure as a first stage for high-risk patients and possible obviate the need for a 2 nd stage SOARD 2010
 - Primary procedure, 24 studies (1749 patients) For primary procedure, follow-up 3-36 mos., 60.6% EWL Conclusions: - Long-term data remain limited - ASMBS accepted SG as an approved bariatric procedure as a first stage for high-risk patients and possible obviate the need for a 2 nd stage SOARD 2010")
18
Is another Operation Needed to Improve to Outcomes of Sleeve?

19
International Sleeve Gastrectomy Expert Panel Consensus Statement Best Practice Guidelines Based on Experience of Over 12,000 Cases Surgery for Obesity & Related Diseases. 8(1):8-19, 2012 Jan doi:10.1016/j.soard.2011.10.019 19 DSL#12-0041
:8-19, 2012 Jan doi: /j.soard DSL#")
20
2011 I NTERNATIONAL S LEEVE G ASTRECTOMY E XPERT C ONSENSUS A UTHORS /P ANEL E XPERTS a Conference Chairman and Statement primary author b Conference Co-Chairman 20 Surg Obes Relat Dis 8(1):8-19, 2012 Jan. Aceves AlbertoMexicoJossart GreggUS Arvidsson DagSwedenLakdawala Muffazal b India Baker S. RandalUSMourad Haicam ElBelgium Basso NicolaItalyNguyen Ninh TUS Bellanger DrakeUSNocca DavidFrance Boza CamiloChilePomp AlfonsUS France MichaelAustraliaPrager GerhardAustria Gagner MichelUSRamos Almino b Brazil Galvao ‐ Neto Manoel BrazilRosenthal Raul J a US Higa Kelvin DUSShah ShashankIndia Himpens Jacques b BelgiumVix MichelFrance Jacobs MoisesUSWittgrove AlanUS Jorgensen John OAustraliaZundel NatanUS/Colombia

21
C OLLECTIVE O UTCOMES D ATA In their sleeve gastrectomy practice: Preoperative age: 42 ± 3.8* years Preoperative BMI: 44 ± 4.5* Approximately 3 of every 4 are women Length of hospital stay: 2.5 ± 0.9* days. Only about 1 ± 2* % converted to open 1 ± 1* % leaks, <1% strictures, and 12 ± 9.0* % GERD postoperatively. 21 Surg Obes Relat Dis 8(1):8-19, 2012 Jan. * Mean and Standard Deviation
:8-19, 2012 Jan. * Mean and Standard Deviation.")
22
Reduces Leaks or Improve Management of Leaks or Both

23
Sleeve Complication

24
Endoscopic Management of Sleeve Leaks

25
Why Gastric Plication is not Ready for Prime Time! Lack of scientific rationale Lack of data No evidence for metabolic effect Not recognized by ASMBS

26
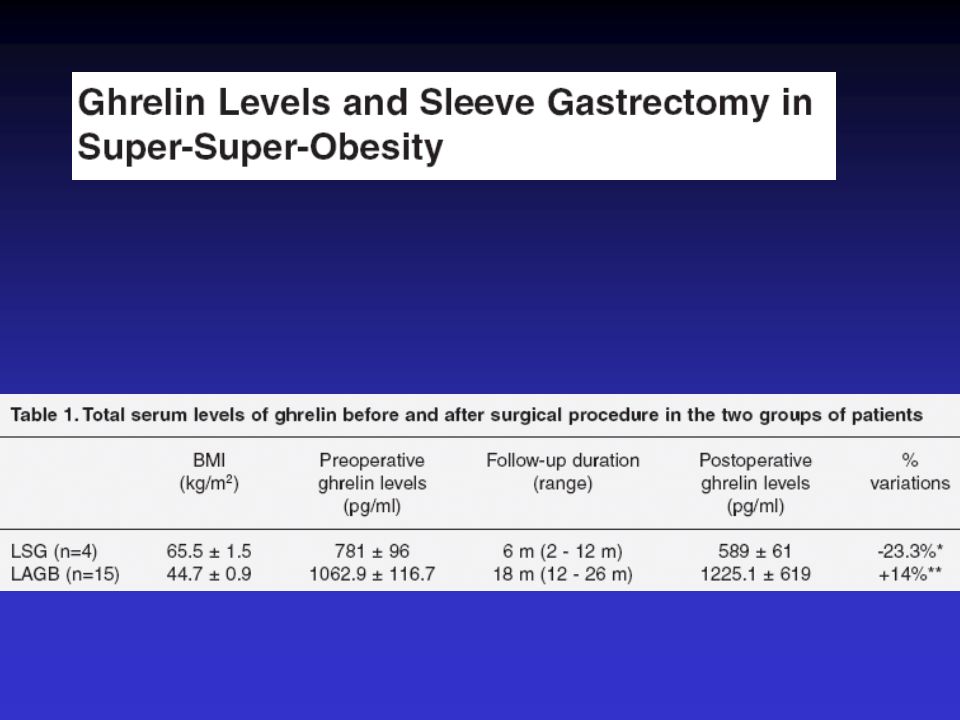
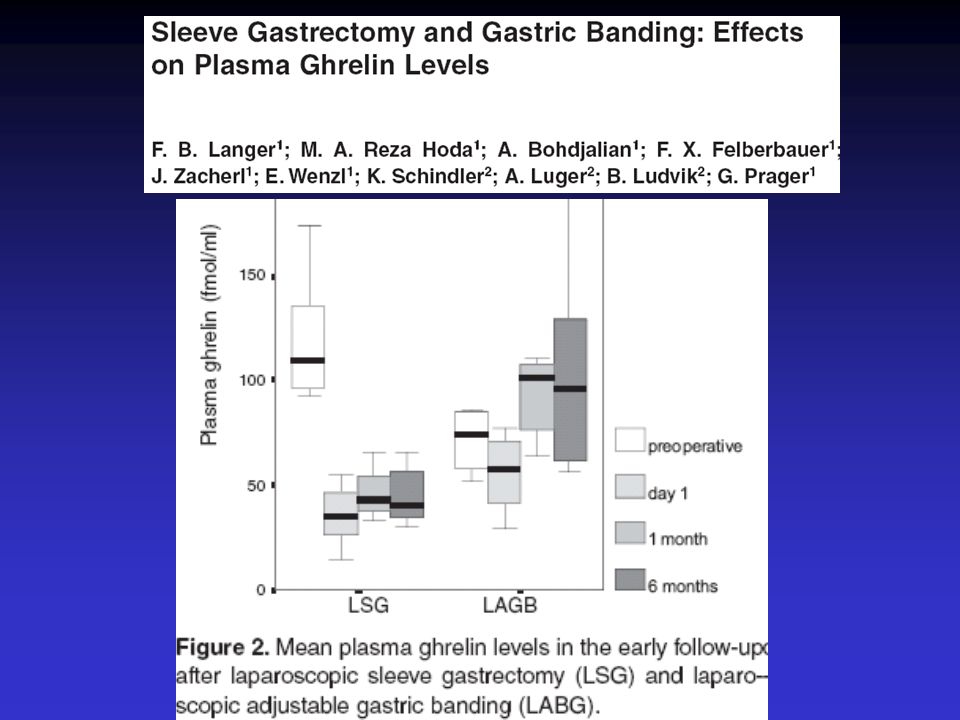
Mechanisms of Sleeve gastrectomy Restriction Neurohormonal changes - Ghrelin - PYY - GLP-1

29
First-phase insulin secretion, insulin sensitivity, ghrelin, GLP-1, and PYY changes 72 h after sleeve gastrectomy in obese diabetic patients: the gastric hypothesis Insulin secretion and peripheral insulin sensitivity using the IVGTT were assessed in 18 obese type 2 diabetic and in 10 nondiabetic obese patients before and 3 days after SG In diabetic patients with disease less than 10.5 years, the first phase of insulin secretion promptly improved after SG, indicating an increased glucose-induced insulin secretion. The second phase of insulin secretion (late AUC) significantly decreased after SG in all groups, indicating an improved insulin peripheral sensitivity. In all groups, pre- and postoperatively, IVGTT determined a decrease in ghrelin values and an increase in GLP-1 and PYY values. Basso et al. Surg Endosc 2011
 significantly decreased after SG in all groups, indicating an improved insulin peripheral sensitivity. In all groups, pre- and postoperatively, IVGTT determined a decrease in ghrelin values and an increase in GLP-1 and PYY values. Basso et al. Surg Endosc")
30
Why Gastric Plication is not Ready for Prime Time! Lack of scientific rationale Lack of data No evidence for metabolic effect Not recognized by ASMBS

31
Surgeon & Innovation OperationTechniqueDeviceIndications Low BMI

32
Why Systematic Process is Needed? Protection of patients Protection of our field Protection of the surgeon

33
Systematic Pathway for Recognzing a New Bariatric Operation FDA approval Accumulate substantial peer-reviewed data demonstrating its safety & short and medium-term efficacy Recognized by ASMBS Obtaining coverage for the procedure

34
Recognition by ASMBS Statement development by the Clinical Issues committee Statement is reviewed by legal advisor Review by ECEC & EC Circulate through membership for comments Review again by EC for approval SOARD for publication

35
Gastric Plication: Is it Ready for Prime Time?

36
ASMBS Policy Statement on Gastric Plication 4 studies (<300 patients) Band & plication (1 study, 26 patients) Recommendations: - Gastric plication should be considered investigational performed under IRB review - Encourage data reporting - Marketing should include a statement that this is investigational - ASMBS does not support CME courses on investigational procedures & devices 10/6/2011
 Band & plication (1 study, 26 patients) Recommendations: - Gastric plication should be considered investigational performed under IRB review - Encourage data reporting - Marketing should include a statement that this is investigational - ASMBS does not support CME courses on investigational procedures & devices 10/6/2011")
37
Gastric Plication is not Ready for Prime Time! Lack of scientific rationale Lack of data No evidence for metabolic effect Not recognized by ASMBS

38
Ninh T. Nguyen, MD Professor of Surgery Division of GI Surgery University of California, Irvine Medical Center Gastric Plication: Is it Ready for Prime Time? Con

Similar presentations