Download presentation
Presentation is loading. Please wait.

1
In the name of God

2
Dr Giti Sadeghian Dermatologist
Alopecia areata Dr Giti Sadeghian Dermatologist

3
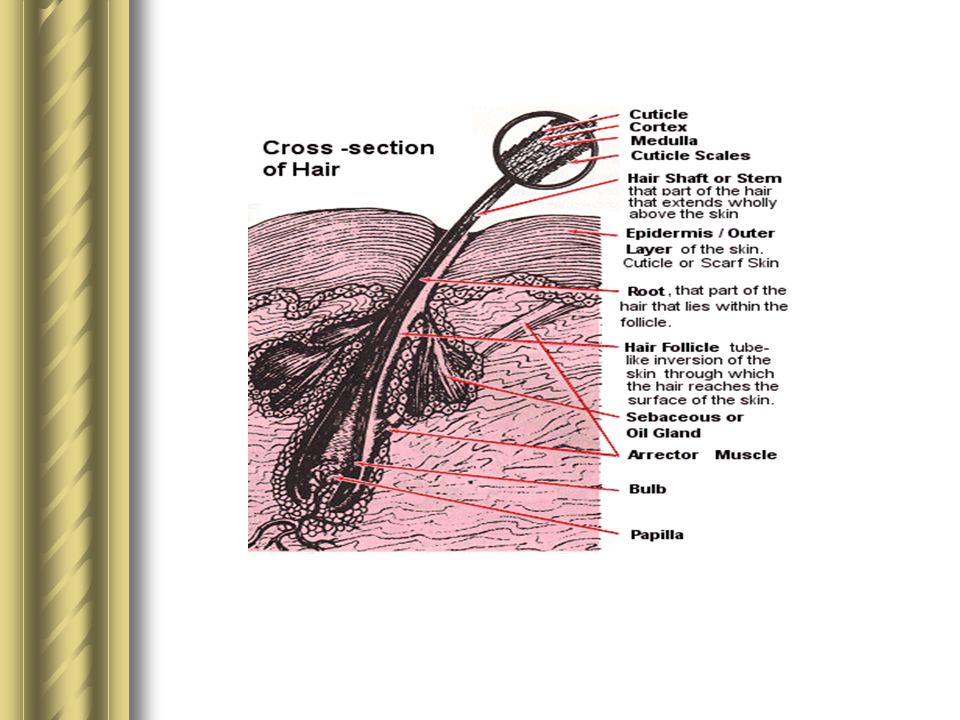
Introduction: Alopecia aerata is a chronic inflammatory disorder affecting hair follicles and sometimes the nails that produces non scarring hair loss.

4
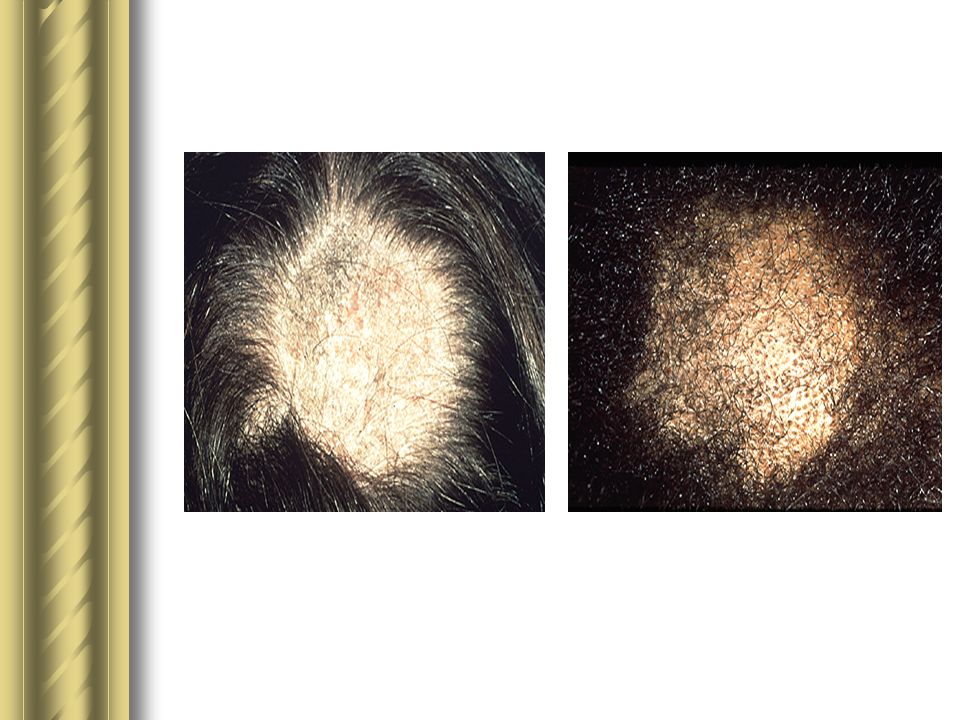
Patient typically Develop discrete Arera of complete Hair loss

5
Epidemiology: The estimated prevalence of alopecia areata is approximately 1 in 1000 people, with a lifetime risk of approximately 2 percent. Men =women Alopecia areata can started at any age although in most patients the onset is before age 30.

6
Patho physiology: the hair follicle pathology of AA is probably mediated by auto reactive T lymphocytes. Hair follicle auto antibodies are frequently present in sera from AA patients but their pathogenic role is uncertain. Other autoimmune diseases, such as vitilligo,thyroiditis,and pernicious anemia, may be associated with AA.

8
Approximately 20% of patient have a family history of AA, indicating a genetic predisposition to the disease. this is thought to be polygenic in nature and association with a variety of genes, predominantly immune response genes, have been reported.

9
A variety of factors, such as infections, drugs, and vaccinations, have been implicated in triggering episodes of AA. Some patients report severe stress, especially emotional stress as a precipitating event, although many patients have no such history.

10
Clinical features: Patients with AA have smooth, circular, discrete area of complete hair loss that develop over a period of a few weeks, followed by regrowth over several months. These patches may enlarge and coalesce into bizarre patterns. Short hairs broken off a few millimeters from the scalp are found at the edges of expanding patches .

16
Area overgrowth often are characterized initially by fine , white vellus hairs.
Alopecia most commonly occurs on the scalp, but may be found on any hair bearing area .

17
There also can be nail involvement with fine pitting or roughening of the nail plates.

18
Eye abnormalities, including the rare early development of cataract, may occur in patients with AA

19
Spontaneous regrowth occurs in the majority of patients.
Around 80% of those with limited patchy hair loss will recover within a year, although almost all will experience more than one episode of the disease. However, alopecia areata may persist for several years and sometimes hair growth never recovers.

20
In a minority of patients there is progression to total loss of scalp hair (alopecia totalis) or loss of the entire scalp and body hair (alopecia universalis).
 or loss of the entire scalp and body hair (alopecia universalis).")
21
Ikeda,s categories: Type 1: the common type 63% Age Total course les than 3 years Alopecia totalis develops in only 6%

22
Type2:atopic type 10% The onset is in childhood Disease course is 10 years Alopecia totalis develops in 75%

23
Type 3:prehypertention type
4% Young adults Disease course is rapid Alopecia totalis develops in 39%

24
Type 4: combined type 5% Patients are over 40 years Course is prolong Alopecia totalis develops in 10%

25
Prognosis

26
The following factors are associated with a poor prognosis and /or high likelihood of relapse:
Onset in childhood Severe disease, specially alopecia totalis or alopecia universalis. Duration of more than one year. Involvement of peripheral scalp (ophiasis) Nail disease Atopy
 Nail disease. Atopy.")
27
Diagnosis

28
The diagnosis of AA is suspected in patients with the following:
Smooth, discrete area of hair loss; affected skin may be slightly reddened but show no other changes. Exclamation point hair at the margins of patches: these are short broken hairs which can be extracted with minimal traction and where the proximal end of the hair is narrower than the distal end. Exclamation point hair can be difficult to see ;their absence does not exclude AA.

30
Biopsy specimens are usually not necessary to confirm the diagnosis, but may be needed in cases where the diagnosis is uncertain. If obtained ,it is best to perform two 4mm punch biopsies into the subcutaneous fat and have one specimen processed with routine vertical sectioning and the other with horizontal sectioning.

31
If only a single specimen is obtained, horizontal sections will give a better representation of the histology. Biopsy taken early in the course of the disease show the majority of follicles in telogen or late catagen. Some anagen hair bulbs are situated at a higher level in the dermis than normal.

32
A peribulbar lymphocytic infiltration is seen around foliclles, this being more dens in early lesions. The infiltrater consiss procominantly of Tcells with increases of langerhans cells. The infiltrate disappears during regrowth.

33
Because of the association between AA and other autoimmune disorders, it is responsible to screen for thyroid disorder or pernicious anemia in the patients with a suggestive history or physical examination.

34
Differential diagnosis:

35
Tinea capitis- tinea capitis may be associated with pruritus and produces scaling and inflammation in area of hair loss AA produces smooth area of hair loss, without any scaling . Adenophaty may be present in tinea capits. Tinea capitis should always be considered in children presenting with patchy hair loss.

38
Nervous hair pulling (trichotillomania)
Trichotillomania pruduces unusual pattern of broken hair of varying length which lead to a characteristic “Wire brush”, feel, as compared with the smooth hair loss of AA. However, AA and trichotillomania can co-exist on the same scalp. A biopsy in the area of alopecia will help differentiate the two conditions.

39
Trichotillomania

40
Trichotillomania

41
Cicatricial Aopecia Cicatricial alopecia may be the result of diverse pathologies, including lichen plano-pilaris, discoid lupus eryhematosu and folliculitis decavans. All are characterized by permanent, distraction of hair follicles. Hair loss is usually patchy and there is loss of follicular orifices. Additional features are variable and depending on the primary pathology may include erythema scaling follicular plugging and pustulation.

42
Cicatricial Aopecia

43
Androgenic Alopecia Onset of hair loss is gradual in androgenic alopecia and in a typical distribution patern. There are no exclamation point hairs. AA occasionally presents as diffuse hair loss, which may resemble androgenetic alopecia but the progression is most wide spreadand more rapid. A biopsy may be necessary in doubtful cases.

45
Secondary syphilis Area of hair loss appear moth- eaten in patients with secondary syphilis rather than the smooth and discrete area seen with AA. Serologic testing may be necessary for differentiation.

46
Counseling Counseling of patients on the nature of AA its prognosis and the treatment options is essential. For the majority of patients AA is a cosmetic issue although it can occasionally cause physical disabilities ,where there is eyelash involvement or marked nail dystrophy.

47
Nevertheless the cosmetic importance of hair loss is such that AA can cause sever emotional problem particularly in children and young women, thought by no means restricted to these groups. In view of limited efficacy of current forms of treatment the clinician has an important role in helping patients adapt to their lack of hair .

48
This is not an easy task and input from other health professionals, such as a clinical psychologist ,may be needed . Many patients though not all are helped by involvement in patient support groups. With children it is often the parents whose reaction must be addressed for the child adjust to the hair loss.

49
Treament

50
Treament Treatment is not mandatory because the condition is benign, and spontaneous remissions and recurrences are common. Treatments used are believed to stimulate hair growth, but no evidence indicates they can influence the ultimate natural course of alopecia areata. Treatment modalities usually are considered first according to the extent of hair loss and the patient's age.

51
Treament Not all patients require treatment. Up to 80 percent of patients with alopecia areata that is limited and of less than one year's duration may expect spontaneous regrowth of hair. Because alopecia areata is believed to be an autoimmune condition, different immunomodulators have been used to treat this condition. Additional treatment options for alopecia areata include minoxidil and other treatment modalities.

52
Topical treatments Corticosteroids
Intralesional corticosteroids — We suggest intralesional corticosteroids as the preferred therapy for adults with isolated patches of hair loss who desire treatment

53
Triamcinolone acetonide (Kenalog) is used most commonly; concentrations vary from mg/mL. The lowest concentration is used on the face. A concentration of 5 mg/mL is usually sufficient on the scalp. Less than 0.1 mL is injected per site, and injections are spread out to cover the affected areas (approximately 1 cm between injection sites; see image below).
.")
54
New growth is usually visible within four weeks
New growth is usually visible within four weeks. The treatment may be repeated as necessary every four to six weeks. Local skin atrophy is a consistent side effect(10%) but usually resolves within a few months. Other side effects of therapy include telangiectasia, hypopigmentation, and systemic absorption.
 but usually resolves within a few months. Other side effects of therapy include telangiectasia, hypopigmentation, and systemic absorption.")
55
Topical steroids Topical steroids have not been extensively evaluated, although they are frequently used to treat alopecia areata, especially in children. 0.2% fluocinolone acetonide cream betamethasone dipropionate 0.05 percent (cream, lotion, ointment) Twice daily applications
 Twice daily applications.")
56
Therapy should be evaluated after three months of use; topical corticosteroids may also be combined with other topical agents or injected glucocorticoids

57
Anthralin Anthralin is an irritant agent.
Both short-contact and overnight treatments have been used. Anthralin concentrations varied from 0.2-1%. Adverse effects include pruritus, erythema, scaling folliculitis, local pyoderma, and regional lymphadenopathy Withholding treatment for a few days results in rapid disappearance of adverse effects

58
Treatment then can be reinstituted, but anthralin should be left on for shorter periods. Staining of clothes and skin can be a concern. The mechanism of action of anthralin is unknown. Most likely, it creates inflammation by generating free radicals, which have antiproliferative and immunosuppressive actions.

59
Use for three months before reevaluating for treatment effectiveness given that treatment with anthralin is uncomfortable and of limited efficacy, we generally do not recommend it, and are particularly hesitant to use it in children.

60
Minoxidil Minoxidil appears to be effective in the treatment of alopecia areata in patients with extensive disease (50-99% hair loss). Response rates in that group vary from 8-45%. Minoxidil was of little benefit in patients with alopecia totalis or alopecia universalis.
. Response rates in that group vary from 8-45%. Minoxidil was of little benefit in patients with alopecia totalis or alopecia universalis.")
61
Minoxidil Minoxidil — Over the counter minoxidil is sometimes used twice daily alone or in combination with betamethasone dipropionate or anthralin in children and adults. The 5% solution appears to be more effective Minoxidil should be tried for three months before evaluating effectiveness.

62
Minoxidil usually is well tolerated
Minoxidil usually is well tolerated. Adverse effects include distant hypertrichosis (5%) and irritation (7%). The exact mechanism of action of minoxidil remains unclear
 and irritation (7%). The exact mechanism of action of minoxidil remains unclear.")
63
mitogenic effect on epidermal cells, both in vitro and in vivo.
Anagen-phase hair bulbs plucked showed a significant increase in proliferation index as measured by DNA flow cytometry. prolong the survival time of keratinocytes in vitro Finally, minoxidil may oppose intracellular calcium entry.

64
Calcium influx normally enhances epidermal growth factors to inhibit hair growth. Minoxidil is converted to minoxidil sulfate, which is a potassium channel agonist and enhances potassium ion permeability, thus opposing the entry of calcium into cells Local vasodilatation does not appear to play a primary role in hair growth associated with minoxidil

65
Immunotherapy Topical immunotherapy is defined as the induction and periodic elicitation of an allergic contact dermatitis by topical application of potent contact allergens.

66
The mechanism of action of topical immunotherapy is unknown
The mechanism of action of topical immunotherapy is unknown. Antigenic competition has been hypothesized. That is, the introduction of a second antigen can initiate a new infiltrate containing T-suppressor cells and suppressor macrophages that may modify the preexisting infiltrate and allow regrowth.

67
Commonly used agents for immunotherapy include squaric acid dibutylester (SADBE) and diphencyprone (DPCP). The median time to achieve significant regrowth was 12.2 months. The relapse rate after reaching significant regrowth was 62.6%.

68
Treatment is provided weekly.
The patient first is sensitized directly on the scalp with a 2% concentration on a small area (2 cm). The following week, a low concentration (0.0001%) is applied. The concentration is increased slowly every week as needed until a mild tolerable allergic contact dermatitis is elicited. Many concentrations are available that achieve this goal.
. The following week, a low concentration (0.0001%) is applied. The concentration is increased slowly every week as needed until a mild tolerable allergic contact dermatitis is elicited. Many concentrations are available that achieve this goal.")
69
Phototherapy Phototherapy and photochemotherapy are potential treatments for alopecia areata. Narrowband UVB is thought to act as an irritant, but there is little documented evidence of efficacy . Psoralen plus UVA therapy (PUVA) can be administered with the psoralen delivered topically as a gel or paint, or orally. Several uncontrolled series have suggested efficacy rates of PUVA of 60 to 65 percent, though with a high relapse rate . Other series have found efficacy rates no higher than might be expected without therapy .
 can be administered with the psoralen delivered topically as a gel or paint, or orally. Several uncontrolled series have suggested efficacy rates of PUVA of 60 to 65 percent, though with a high relapse rate . Other series have found efficacy rates no higher than might be expected without therapy .")
70
Treatment is usually for four to six months, which can result in high cumulative doses. However, a trial of photochemotherapy may be reasonable in patients with extensive alopecia areata (more than 75 percent of scalp involved), alopecia totalis, or alopecia universalis when topical immunotherapy is contraindicated or unacceptable to the patient.
, alopecia totalis, or alopecia universalis when topical immunotherapy is contraindicated or unacceptable to the patient..")
71
PUVA PUVA is a relatively safe treatment modality; adverse effects include burning and, possibly, an increased risk of skin cancer.

72
Oral corticosteroids Systemic steroids most likely are effective via their immunosuppressive effects. An initial benefit may occur by using systemic prednisone in some patients, but the relapse rate is high, and it does not appear to alter the course of the condition. Systemic prednisone is not an agent of choice for alopecia areata because of the adverse effects associated with both short- and long-term treatment.

73
Cyclosporine Cyclosporine has been used both topically and systemically in the treatment of alopecia areata. Topical cyclosporine has not proven to be effective in severe alopecia . The mechanism of action of cyclosporine remains unclear. It may act through its immunosuppressive effect

74
In conclusion, topical cyclosporine has shown limited efficacy
In conclusion, topical cyclosporine has shown limited efficacy. Although systemic CsA appears to be effective in alopecia areata, the adverse effect profile, the recurrence rate after treatment discontinuation, and thus, the inability to produce long-term remissions, make CsA unattractive for the treatment of alopecia areata.

75
Tacrolimus Regrowth was shown on the application site of topical tacrolimus in 2 studies using the DEBR model. Oral tacrolimus was ineffective. No benefit was shown in the use of topical tacrolimus for alopecia areata in a small 2005 study by Price et al that included 11 patients.[25]

76
Interferon A study of 11 patients with alopecia areata ranging from patchy alopecia areata to alopecia universalis showed no benefit using intralesional interferon alfa-2 (1.5 million IU, 3 times per wk for 3 wk).
.")
77
Dapsone, Methotrexate, latanoprost,nitrogen mustard, massage and relaxation, isoprinosine, acupuncture, and aromatherapy efficacy of these treatments needs to be demonstrated in larger, placebo-controlled trials before they can be recommended

78
Biological agents including adalimumab, alefacept, etanercept and infliximab) in the treatment of alopecia areata did not show efficacy, and some patients developed alopecia areata while under treatment with biologic agents for other conditions.
 in the treatment of alopecia areata did not show efficacy, and some patients developed alopecia areata while under treatment with biologic agents for other conditions.")
79
Nonpharmacologic methods
A systematic MEDLINE search could not find any study with sufficient validity to provide scientific evidence of benefit with complementary and alternative medicine therapies for alopecia areata

80
A study on hypnosis for refractory alopecia areata did not show efficacy of regrowth, but it did show that hypnosis can improve depression, anxiety, and quality of life in affected patients

81
COSMETIC APPROACHES — Female patients with extensive alopecia areata will usually require a wig or hairpiece. Wigs are generally less successful in men where hair styles, such as shaving the scalp, are often a more acceptable approach. Temporary tattooing can be helpful for loss of eyebrows.

82
INFORMATION FOR PATIENTS
Explain in detail that although any of the treatments discussed can induce resumption of normal hair growth, none will "cure" the disease or prevent recurrence after healing. In the United States, patients can be encouraged to contact the National Alopecia Areata Foundation, a national support group that publishes a newsletter and provides names of local support groups.

83
SUMMARY AND RECOMMENDATIONS
Patients with alopecia areata typically have smooth, circular, discrete areas of complete hair loss that develop over a period of a few weeks, followed by regrowth over several months. . The diagnosis of alopecia areata is typically made on clinical grounds. Patients have smooth discrete areas of hair loss, and exclamation point hairs may be seen at the margins of patches. . The cosmetic effects of alopecia areata can cause severe emotional distress; counseling in such patients is essential. .

84
Not all patients with alopecia areata require treatment; up to 80 percent of patients with limited alopecia areata of less than one year's duration will experience spontaneous regrowth of hair. There is relatively little evidence on treatment from well-designed clinical trials. For patients who desire treatment, we suggest the following:

85
We suggest that localized scalp alopecia areata be treated with intralesional injections of corticosteroids . Clinicians should consider referral to a dermatologist if facial steroid injections are required. . In children or adults with limited disease and who have concerns about exposure to intralesional steroids, we suggest treatment with topical corticosteroids .

86
If intradermal or topical corticosteroid therapy produces an inadequate response, we suggest a trial of topical 5 percent minoxidil either alone or in combination with continued corticosteroid therapy . We suggest that patients with extensive alopecia areata, including alopecia totalis, as well as patients with more limited disease who do not respond to the above therapies be treated with topical immunotherapy .

87
Patients should generally be referred to a dermatologist for such therapy and any additional management. Photochemotherapy is another option for patients with extensive disease when topical immunotherapy is contraindicated or unacceptable. Long-term photochemotherapy should be avoided.

88
Patients who do not desire treatment may benefit from cosmetic interventions. Wigs (particularly in women) and shaving the scalp (in men) may produce an acceptable cosmetic result. Temporary tattooing can be helpful for loss of eyebrows.
 and shaving the scalp (in men) may produce an acceptable cosmetic result. Temporary tattooing can be helpful for loss of eyebrows..")
89
The End

Similar presentations






















 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")
 Yalew /MD,IMG/ Observational Case Study Hair Re-Growth Program using an Electro Stimulator.>")

 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")

