Download presentation
Presentation is loading. Please wait.

1
Novel Aspects of Renal Bone Disease: Current guidelines Günter Klaus, Marburg, Germany

2
Review Parts of... European Guidelines (Klaus et al, 2006) K/DOQI Clinical Practice guidelines for Bone Metabolism and Disease in children with Chronic Kidney Disease 2005 (kdoqi/guidelines_pedbone)
 K/DOQI Clinical Practice guidelines for Bone Metabolism and Disease in children with Chronic Kidney Disease 2005 (kdoqi/guidelines_pedbone).")
3
Guideline 1: Biochemical and radiological marker MarkerFrequency at GFR 59-30 29-15 < 15 Aim calcium 6 3 1normal range phosphate 6 3 1normal range for age band Ca x Pi 6 3 1 target range 3.3-4.4, 5.0 mmol 2 /l 2, AP 6 3 1Normal range (age band) S-HCO 3 - 6 3 1normal range, at least: bicarbonate > 22mmol/l, base excess > -5 mmol/l PTH 6 3 1within normal range in moderate CRF (GFR>29ml/min/1.73m 2 ) 2-3 times upper limit of normal in advanced CRF or on dialysis 25-(OH) D 3 as indicated> 20 pg/ml left hand / wrist X-ray 6-12no radiological signs of sHPT, Looser zones or osteopenia
 S-HCO normal range, at least: bicarbonate > 22mmol/l, base excess > -5 mmol/l PTH 6 3 1within normal range in moderate CRF (GFR>29ml/min/1.73m 2 ) 2-3 times upper limit of normal in advanced CRF or on dialysis 25-(OH) D 3 as indicated> 20 pg/ml left hand / wrist X-ray 6-12no radiological signs of sHPT, Looser zones or osteopenia")
4
Case 1 (2002) 2y old girl CKD due to fetofetal Transfusion Syndrome (shock) CCR 7.8 ml/min/1.73m2 SDS Height –3,04, weight –2.15, BMI –0,08 Treatment: erythropoietin 1000 U/w s.c. iron supplements sodium bicarbonate (BE-0.8) 1,25(OH) 2 D 3 0.15µg/d in the morning
 1,25(OH) 2 D µg/d in the morning.")
5
Calcium-Phosphate-Vitamin D Ca 2.6 mmol/l (2.2-2.7) Phosphate 1.9 mmol/l (1.25-2.1) 25(OH)D 10 nmol/l (10-20) PTH 105 pg/ml (19-80) X-ray left wrist: no periosteal resorption zones, no metaphyseal abnormalities
 Phosphate 1.9 mmol/l ( ) 25(OH)D 10 nmol/l (10-20) PTH 105 pg/ml (19-80) X-ray left wrist: no periosteal resorption zones, no metaphyseal abnormalities")
6
Recommendation 7: Vitamin D deficiency should be avoided (Klaus et al, 2006) Common, deficiency ( 80% adult dialysis patients (Sadlier 2007, Del Vale 2007) In early CRF: PTH-levels ~ 25(OH)D-Conc. (Reichel 1991) Same after TPL (good renal function) dto. ( Lomonte 2005) Vit D Substitution in pts. with 25(OH)D 3 in the range 20 to 50 nmol/l lowers iPTH (Van der Wielen, 1995) sHPT in CRF-Pts. 38% with 25(OH)D > 20ng/ml 68% with 25(OH)D < 20ng/ml (Holick 2005) extra-renal 1 -OHase is substrate dependent 25(OH)D 3 but not 1,25(OH) 2 D 3 affects muscle phosphate content and muscle function (Birge SJ 1975; Eastwood JB 1977) OH HO OH
 Same after TPL (good renal function) dto. ( Lomonte 2005) Vit D Substitution in pts. with 25(OH)D 3 in the range 20 to 50 nmol/l lowers iPTH (Van der Wielen, 1995) sHPT in CRF-Pts. 38% with 25(OH)D > 20ng/ml 68% with 25(OH)D < 20ng/ml (Holick 2005) extra-renal 1 -OHase is substrate dependent 25(OH)D 3 but not 1,25(OH) 2 D 3 affects muscle phosphate content and muscle function (Birge SJ 1975; Eastwood JB 1977) OH HO OH.")
7
25-(OH)-Vitamin D and PTH CKD 2-3(-4), n=57 77 % Vit D Insufficiency Supplementation with Ergocalciferol 2000 IE insufficiency 4000 IE deficiency decrease of PTH in treated 122±83 to 80±59ng/ml Increase in untreated 119 ± 93 to 143 ± 104 (p < 0.001) Prior to ergocalciferol treatment: Menon et al., Pediatr Nephrol 2008
-Vitamin D and PTH CKD 2-3(-4), n=57 77 % Vit D Insufficiency Supplementation with Ergocalciferol 2000 IE insufficiency 4000 IE deficiency decrease of PTH in treated 122±83 to 80±59ng/ml Increase in untreated 119 ± 93 to 143 ± 104 (p < 0.001) Prior to ergocalciferol treatment: Menon et al., Pediatr Nephrol 2008")
8
Vitamin D Supplementation Dose? 500 Units/d(Marburg, 66.6 % sufficency, no deficiency in CKD 3-5) 2000 IE/d x 12 weeks in insufficency 4000 IE/d x 12 weeks in deficiency 8000 IE/d x 4 weeks, then 4000 IE/d x 8 weeks severe deficiency (DOQI)
 2000 IE/d x 12 weeks in insufficency 4000 IE/d x 12 weeks in deficiency 8000 IE/d x 4 weeks, then 4000 IE/d x 8 weeks severe deficiency (DOQI).")
9
Calcium-Phosphate Ca 2.6 mmol/l (2.2-2.7) Phosphate 1.9 mmol/l (1.25-2.1) 25(OH)D 35 nmol/l (10-20) PTH 105 pg/ml (19-80) X-ray left wrist: no periosteal resorption zones, no metaphyseal abnormalities ? ?

10
Recommendation 8: Marked hyperparathyroidism should be prevented in children with CRF prior to dialysis Low doses of active Vitamin D Metabolites Normal PTH with strictly controlled Pi (GFR> 30): normal iPTH/whole PTH normal AP (Waller 2003)
: normal iPTH/whole PTH normal AP (Waller 2003)")
11
Waller S 2006 crea. 140µmol/l phosphate 0.84 ULN height SDS-1.73

12
Recommendation 10: If PTH is elevated in CRF stage 3 or more than 2-3 times normal in stage 4- 5 in the presence of Pi < 2 mmol/l, active vitamin D metabolites should be administered orally.... in the evening (Tsuruoka 2003) less hypercalcemia more effective suppression of PTH..... 20-40 ng/kg/d (lowest effective dose)
 less hypercalcemia more effective suppression of PTH ng/kg/d (lowest effective dose).")
13
Concept: Why elevated PTH in CKD V? PTHRmRNA reduced in bone and growth cartilage cells Picton ML 2000, Sanchez 1998 ADBD with PTH levels up to 3x ULN Kuizon 1998 Risk of hypercalcemia with low normal PTH Klaus 1991

14
Treatment with active Vitamin D- Metabolites: PTH-levels (pg/ml) CKD-StageEPDWGK/DOQIDose(k/DOQI) 2-310-6535-70 4130-19570-110 20kg 0.25µg/d 5130-195200-300 0.0075-0.025µg/kg (2-3x ULN) (3-5x ULN) max 1µg/d European Dose :..... 20-40 ng/kg/d (lowest effective dose)
.")
15
Control of Mineral Metabolism in 620 Children on PD % patients meeting pediatric KDOQI guidelines

16
PTH and Growth in Children on Chronic PD

17
Bone Histology prior to RRT Waller et al, Pediatr Nephrol 2008 N=11, follow-up prior histolgy 1.1 year Policy: phosphate control 50.pc, PTH within normal range Results: Low turnoverPTH within normal range, n=2 mixed lesionsPTH 1.1-1.4 ULN, n=4 high tunoverPTH > 2.9 ULN, n=4

18
EU DOQI Pi, AP x ULNCa mmol/l, Calcidiol µg PTH pg/ml Case: 2 y-old, PD, PEG GH

19
Calcimimetics Persistent decrease of PTH levels in comb. with Vitamin D upregulates decreased calcium-sensing receptor expression level in parathyroid glands Mizobuchi 2004 Reduced CVR expected - decreases extraosseous calcifications in uremic rats treated with calcitriol Lopez 2006 - marked and sustained antihypertensive effect (rat) Odenwald 2006 Risk of hypocalcemia First data in pediatric patients
 Odenwald 2006 Risk of hypocalcemia First data in pediatric patients.")
20
Effect of cinacalcet on PTH in children Muscheites 2008

21
Calcium-Phosphate 1 year later Ca 2.3 mmol/l (2.2-2.7) Phosphate 2.1 mmol/l (1.0-1.95) PTH 151 pg/ml (19-80) AP 335 (-281)
 Phosphate 2.1 mmol/l ( ) PTH 151 pg/ml (19-80) AP 335 (-281)")
22
High Phosphate is a risk factor Myocardial fibrosis Hyperparathyroidism Parathyroid adenoma Soft tissue calcification áCardiovascular mortality

23
Effect of Phosphate on Vascular Calcification In vitro calcification of smooth muscle Expression of osteoblastic markers (Jono S., Circulation Res 2000) in vivo: calcification of the media (Ibels LS et al., Am J Med 1979) + expression of osteoblastic markers (Moe SM., Kidney Int 2002)
 in vivo: calcification of the media (Ibels LS et al., Am J Med 1979) + expression of osteoblastic markers (Moe SM., Kidney Int 2002)")
24
Recommendation 4: If plasma phosphate is elevated, phosphate intake should be limited to the recommended levels Dietary counselling by a trained dietician Protein intake reduced to recommended levels (Coleman 2001) rule of thumb: normal + 50% in PD Dietary training with patients and parents
 rule of thumb: normal + 50% in PD Dietary training with patients and parents")
25
Recommendation 5: In case of hyperphosphatemia, the dialysis efficacy should be optimised increase dwell volume to 1000-1400 ml/m 2 BSA avoide a too short dwell time a daytime dwell should be added prolong time on dialysis (PD) increase frequency (daily HD)
 increase frequency (daily HD)")
26
Recommendation 6: For control of hyperphosphatemia, aluminium- free phosphate binders should be administered Calcium containing phosphate binder CaCO 3 elemental calcium content 40%, can be crushed CaAc, elemental calcium content 25% higher Pi-Binding potency independent of pH upper intake level of elemental calcium is suggested to be 2500 mg/d for children above 4 years of age to be taken with meals dietary supervision and training Check serum calcium and Ca x P Check compliance

27
Ca-containing PB Efficacy Established Risks High dose=high calcium load Adynamic bone disease Hypercalcemia (less with CaAcetate) Vascular calcification Benefits cheapest PB Reduction of sHPT Correction of hypocalcemia
 Vascular calcification Benefits cheapest PB Reduction of sHPT Correction of hypocalcemia")
28
Effect of Type of Phosphate Binder on Mortality Block GA 2007

29
Sevelamer in Children crossover Sevelamer and Calcium-Acetate n=18 Equal serum phosphate control More metabolic acidosis with sevelamer (p>0.005) More hypercalcemia in CaAc (p<0.0005) Decreased total (-27%) and LDL cholesterol (- 34%) Pieper 2006
 More hypercalcemia in CaAc (p<0.0005) Decreased total (-27%) and LDL cholesterol (- 34%) Pieper 2006")
30
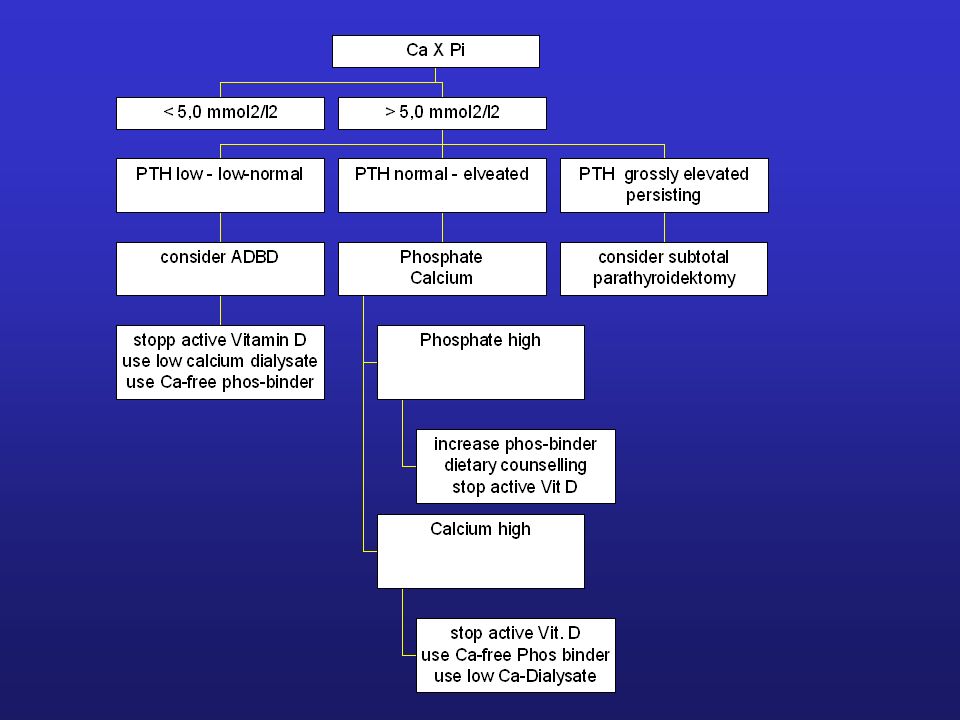
Recommendation 13: The calcium phosphorus product should be kept within the normal range, at least below 5.0 mmol 2 /l 2 (60 mg 2 /dl 2 ). stop active vit. D use low-calcium dialysate reduce Ca-cont. phos-binder PTH low -low normal continue current phos-binder and active vit D therapy PTH=1-3 x normal increase active vitamin D PTH elevated above target range < 5,0 mmol2/l2 stopp active Vitamin D use low calcium dialysate use Ca-free phos-binder consider ADBD PTH low - low-normal increase phos-binder dietary counselling stop active Vit D Phosphate high stop active Vit. D use Ca-free Phos binder use low Ca-Dialysate Calcium high Phosphate Calcium PTH normal - elveated consider subtotal parathyroidektomy PTH grossly elevated persisting > 5,0 mmol2/l2 Ca X Pi

31
Bilginer 2007 cIMT and CaxPi Transplanted children (n=24) IMT ~ with time on dialysis CaxPi product before transplantation
 IMT ~ with time on dialysis CaxPi product before transplantation")
32
Effect of cinacalcet on CaxPi Muscheites 2008

34
Summary/Perspective Prevention of CKD-BMD: Vitamin D deficiency is to be avoided Ca, Pi and CaxPi should be kept in the normal range Administration of a too high amount of Ca should be prevented New data suggest stricter control of PTH target levels (1-2 (-3) x ULN?) (Opinion-based) guidelines are usefull to aid in therapy to stimulate new studies
 x ULN ) (Opinion-based) guidelines are usefull to aid in therapy to stimulate new studies")
35
Klaus@med.uni-marburg.de EPDWG A.Watson, A. Edefonti, M. Fischbach, K. Rönnholm, F. Schaefer, E. Simkova, C.J. Stefanidis, V. Strazdins, J. Vande Walle, C. Schröder, A. Zurowska, M. Ekim

36
CaxPi-Product stop active vit. D use low-calcium dialysate reduce Ca-cont. phos-binder PTH low -low normal continue current phos-binder and active vit D therapy PTH=1-3 x ULN increase active vitamin D PTH elevated above target range < 5.0 mmol2/l2

Similar presentations












>")


>")



