Download presentation
Presentation is loading. Please wait.

1
Research

2
Deficiencies of Health Care in the United States
Barbara Starfield, M.D., MPH, John Hopkins School of Hygiene and Public Health stated in the July 26, 2000 issue of JAMA the following: New studies indicate that 20-30% of patients receive contraindicated care. An estimated 44,000 to 98,000 people die per year as a result of medical errors.

3
Of 13 countries in a recent comparison, the United States ranks an average of 12th (second from the bottom for 16 available health indicators) The poor performance of the U.S. was recently confirmed by the World Health Organization, which uses different indicators, ranked the United States as 15th among 25 industrialized countries. "The health care system also may contribute to poor health through its adverse effects."

4
For example: 12,000 deaths/year due to unnecessary surgery
7,000 deaths/year from medication errors in hospitals 20,000 deaths/year from other errors in hospitals 80,000 deaths /year from nosocomial infections in hospitals 106,000 deaths/year from non-error, adverse effects of medications "These total to 225,000 deaths/year from iatrogenic causes."

5
"In any case, 225,000 deaths/year constitutes the third leading cause of death in the United States, after deaths from heart disease and cancer."

6
Dangers of Medical Care (updated)
Hospital adverse drug reactions-106,000 deaths and costing 12 billion. Medical errors-98,000 deaths, costing 2 billion Bedsores 115,000 deaths, costing 5 billion Malnutrition-108,000 deaths Outpatient adverse drug reactions-199,000 deaths costing 77 billion Surgery related deaths 32,000 deaths, 9 billion

7
Dangers of Medicine (continued)
Unnecessary procedures-37,136 deaths costing 122 billion dollars Total number of iatrogenic deaths each year in the United States hits 783,936 deaths at a cost of $282 billion dollars! Deaths from heart disease annually are 669,697. Deaths from cancer annually are 553,251.

8
Dangers of Medicine (continued)
Information gleaned from an article entitled-”Medicine Found to be the Number One Cause of Death in the United States” This study was reported in the book Death By Medicine by Gary Null and can be found at The Chiropractic Journal June 2005 David Singer

9
Chronic Cervicogenic Headaches
Australia: Chronic Cervicogenic Headaches. Whittingham et al, from RMIT University, Melbourne determined the efficacy of cervical adjustments (toggle recoil 3 times per week over a 3 week period) for chronic cervicogenic headache (experienced for 6 months or more) by randomly assigning 105 patients to either a treatment group or a control group which received 9 sham adjustments.
 for chronic cervicogenic headache (experienced for 6 months or more) by randomly assigning 105 patients to either a treatment group or a control group which received 9 sham adjustments.")
10
The treatment group had significant improvement on all measures including headache pain, headache intensity, pressure algometry scores, and cervical range of motion - whereas the control or placebo group improved on one measure only.

11
It was concluded that upper cervical spine adjustment using toggle recoil technique is effective for patients with chronic cervicogenic headache. (Whittingham W, Dacosto C et al. Abstract, Proceeding of the 6th Biennial Congress, 2001, World Federation of Chiropractic, ).
..")
12
Natural course of Low-Back Pain
Denmark: Natural course of low-back pain. There have been several studies over the past few years refuting the traditional claim that "9O% of low-back pain patients get well within a month if left untreated."

13
In this study Hestbaek, Leboeuf-Yde, et. al
In this study Hestbaek, Leboeuf-Yde, et. al. from the University of Southern Denmark further investigated the myth of natural remission, firstly by doing a systematic literature review and secondly by reporting with data from 2,000 LBP patients they have been studying for more than five years. They conclude it is now clear "that low back pain does not resolve itself when ignored". Supporting data includes:

14
In their new study in Denmark, only 10% of people with LBP report they are pain-free both 1 and 5 years after their initial episode of pain and care. On a systematic: review of all the literature, 62% of LBP patients report that they still have pain one year after their initial episode. (Hestbaek L, Lehoeuf Yde C, Engbeq M , et al. Abstract, Proceedings of the 6th Biennial Congress, 2001, World Federation of Chiropractic, 247).
.")
15
JMPT Changes in Brain Function after Manipulation of the Cervical Spine Fredrick Carrick DC PhD October 1997 Manipulation of the cervical spine may be associated with an increase or decrease in brain function depending upon the side of the manipulation and the cortical hemisphericity of a patient.

16
Upper Cervical Protocol For Ten Meniere’s Patients By Michael Burcon, D.C.
Copyrighted Journal of Vertebral Subluxation Res. Meniere’s is characterized by vertigo, nausea, inner ear pressure, low frequency hearing loss, and tinnitus. HA’s,depression, neck stiffness, and “brain fog” are associated symptoms. A Blair series of cervical x-rays were taken along with standard upper cervical testing procedures. It is noteworthy that each of the Meniere’s patients had a posterior inferior displacement (subluxation) of the C-1 segment. Conclusion: All patients responded favorably to side posture spinal adjustments. The odds that ten consecutive Meniere’s patients would have a posterior and inferior atlas listing with laterality on the opposite side of ear involvement is over one million to one!
 of the C-1 segment. Conclusion: All patients responded favorably to side posture spinal adjustments. The odds that ten consecutive Meniere’s patients would have a posterior and inferior atlas listing with laterality on the opposite side of ear involvement is over one million to one!")
17
The Most Effective Therapy for So-called Whiplash Injuries Manual Medicine 1989
This paper was originally presented to the International Congress of the Federation Internationale in which Bohm followed five patients who had upper cervical rotary instability after traumatically induced ligament damage. Tx included drugs, immobilization, infiltration of C-0-2 facets, and chiropractic manipulation. It was found that a unique form of treatment called “atlas therapy” was the most effective and often the only procedure that helped the patients. Bohm P. Atlastherapy (A. Arlen)
")
18
Upper Cervical Management of a Multiple Sclerosis Patient Erin Elster, D.C.
A 47 y/o female experienced Sx of MS for three years when she noticed cognitive problems and loss of bladder control. The neurologist noticed lesions (MS plaque) on the MRI and weakness in the legs with numbness in both the arms and legs developed as her condition worsened without remission. The chiropractic examination revealed radiographic evidence of an UC subluxation and paraspinal digital imaging confirmed disturbances at the C-1 level. After four months of UC care, all signs of MS were absent. After a year of being asymptomatic, a follow-up MRI showed no new lesions and reduction of intensity of original lesions. JVSR Journal of Vertebral Subluxation Research June 2001
 on the MRI and weakness in the legs with numbness in both the arms and legs developed as her condition worsened without remission. The chiropractic examination revealed radiographic evidence of an UC subluxation and paraspinal digital imaging confirmed disturbances at the C-1 level. After four months of UC care, all signs of MS were absent. After a year of being asymptomatic, a follow-up MRI showed no new lesions and reduction of intensity of original lesions. JVSR Journal of Vertebral Subluxation Research June")
19
Masked Rotatory Subluxations of the Atlas Associated with Fx of the Clavicle American Journal of Orhtopedics 1998 Al-Etanik, et al The authors discuss how the spines of children have no osseous stability at the C-1,2 level. The authors note that the head of a child reaches 90% of adult size by age 2. Minor trauma and/or sudden rotatory neck movement can cause the articulation to exceed the cartilaginous boundaries. Torticollis may result from this condition and if the deformity persists, fibrosis can result in a fixed subluxation.

20
The Thalamic Neuron Theory (TNT) postulates that the central nervous system (CNS) is involved in all disease processes, as the CNS not only processes incoming physical and chemical information from the periphery, it also sends out physiological commands to the periphery in order to maintain homeostasis for the entire body. Inherent in its capacity to learn and adapt (i.e. to habituate) is the CNS’ ability to learn to be sick (pathological habituation) by looking certain deranged central neural circuitries, leading to chronic disease states Medical Hypothesis T.N. Lee.

21
Anterior Cervical Subluxation: An Unstable Position American Journal of Roentgenology 1979 Scher AT
Scher describes the radiographic signs of cervical anterior subluxation as subtle, yet “the most unstable cervical spinal injury”. This statement shows the seriousness attached to the condition. Note-Many chiropractic methods fail to recognize anterior displacement in the cervical spine.

22
Dystonia Associated with Atlantoaxial Subluxation Clinical Neurological Neurosurgery 2000 Al-Jishi, A, et al This case study reports on a patient with primary dystonia and associated atlanto-axial subluxation. Primary dystonia is an isolated movement disorder without involving the pyramidal & cerebellar systems or the cerebral cortex. This 46 y/o man has had the condition since childhood. Imaging studies showed severe cervical spondylosis & C-1,2 subluxation. This study is the first report in medical literature showing the relationship between primary dystonia and C-1,2 subluxations.

23
C-1 Adjustments This study investigated if a statistically significant difference in symptomatic improvement existed between patients in two groups with different amounts of initial corrections in cervical misalignment, as shown by x-ray analysis.

24
First Adjustment Best Adjustment
Patients had better outcomes, based on the improvement of clinical signs and the reduced need for follow-up adjustment, when the occipito atlantoaxial subluxation complex was reduced by at least 50% after the first adjustment. Chiro. Research Jour. Spring 1997

25
Suboccipital Stretch increases Hip Flexion
Sixty university students between 18 and 35 years of age were studied to compare the effectiveness of a spinal (suboccipital) stretching technique.
 stretching technique.")
26
The two stretching treatments resulted in increased flexion ROM at the hip.SLR was primary test. Statistical analysis revealed that only the suboccipital stretching procedure increased hip flexion ROM significantly. Manual therapy of the neck may have a role to play in the treatment of extraspinal, lower-limb musculoskeletal conditions. JMPT September 1997

27
Leg Check an Accurate Clinical Test?
Fifty-five subjects were studied in an attempt to abstract the essential elements of chiropractic prone leg checking. Subjects were lowered to the prone position on the table to detect dynamic leg positions. On average right legs showed a greater response under distractive and compressive loads.

28
These findings give support to the clinical reality of the functional short leg. The prone leg check can be used as a loading procedure to detect non-weight-bearing functional asymmetry in loading responses caused by differences in left-right muscle tone, joint flexibility and tissue stiffness. JMPT January 1998

29
ACTIVE C.R.O.M. INCREASES AFTER TOGGLE RECOIL MANIPULATION Wayne Whittingham, D.C., PhD & Niels Nilsson, D.C., MD, PhD Objective: To study changes in active CROM following spinal manipulation of the C-sp. Method: 105 patients with cervicogenic headache were randomized into two groups with one group receiving an am toggle recoil while the other group received sham adjustments. After each trial phase, active CROM was measured by strap-on head goniometer by two blinded examiners. Results: After receiving spinal manipulation, active range of motion in the cervical spine increased significantly compared to the sham group that showed very little change. Conclusion: Spinal manipulation of the cervical spine increases active range of motion. Journal of Manipulative and Physiological Therapeutics Nov./Dec 2001 Volume 24, Number 9

30
Determining the relationship between cervical lordosis and neck complaints
Jeb McAviney, MS (Chiro); Dan Schultz BSc; Richard Bock, MS(Chiro);Deed E. Harrison, DC; Burt Holland, PhD Objective: To investigate the presence of a “functionally normal” cervical lordosis. Methods: Drawing a line of the posterior C-2 and C-7 vertebral bodies on 277 lateral cervical x-rays. Results: Patients with lordosis of 20 degrees or less were more likely to have cervicogenic symptoms. Clinically normal range was found to be degrees Dynamic Chiropractic June 18, 2005
; Dan Schultz BSc; Richard Bock, MS(Chiro);Deed E. Harrison, DC; Burt Holland, PhD. Objective: To investigate the presence of a functionally normal cervical lordosis. Methods: Drawing a line of the posterior C-2 and C-7 vertebral bodies on 277 lateral cervical x-rays. Results: Patients with lordosis of 20 degrees or less were more likely to have cervicogenic symptoms. Clinically normal range was found to be degrees. Dynamic Chiropractic June 18,")
31
Innocuous Mechanical Stimulation of the Neck and Heart Rate Changes Autonomic Neuroscience Aug ;19(1-2):96-9 This study examined the effects of cervical manipulation on heart rate of healthy young adults. Authentic manipulations vs sham produced significant + changes in both heart rate and heart-rate variability. Results may reflect a shift between sympathetic and parasympathetic output of the heart. WARNING- A DC using the Blair Technique started care for a pt with high BP and after a C-1 correction, the BP dropped from 160/90 to 80/50. Once the MD deleted the meds the level was 120/80 Dan Murphy

32
Hearing Loss After Blunt Neck Trauma Otology and Neurotology 2003: 24(5):734-737 Segal, et al
Objective-to report for the 1st time hearing impairment from blunt neck trauma involving 83 patients. 51.5% had hearing loss, 55.4% noted tinnitus within three months of the trauma. A reflexogenic disturbance of the neck via divergent afferent proprioceptive activity to the central auditory nervous system might be an explanation.” The medical prognosis is poor with only 10% showing spontaneous improvement within a year.

33
Cervicogenic Hearing Loss M
Cervicogenic Hearing Loss M. Hulse, Professor of ENT, Heidelberg University Source: Greg Buchanan Findings in 62 patients suffering from vertebragenic hearing disorders are reported before and after chiropractic management. Results indicate that hearing disorders are reversible… the therapy of choice is chiropractic manipulation of the upper cervical spine.

34
B.J. Palmer

35
Brief synopsis of his life.
B.J. Palmer,D.C. Brief synopsis of his life. 1910 introduced X-ray to the profession 1925 Neurocalometer 1935 Electroencephaloneuromentimpograph 1938 Spalteholze Labs in Dresden, Germany "wet specimen" (Monkey experiments regarding spinal cord irritation)
")
36
Clearview Sanitarium by Dr. Ted Koren
In 1934, in North Dakota, a number of medically incurable patients were transferred to Forest Park Sanitarium and, within a year, a cure rate of more than 50 percent was reported. The results so impressed Richland County, N.D., Probate Judge A.W. Ponath that he consistently refused to commit a patient to the state mental hospital unless that patient first had at least three months care in the chiropractic sanitarium.

37
He published a pamphlet, Facts: What Chiropractic Has Done For Insanity, which compared the records at Jamestown (N.D.) Mental Hospital and the Forest Park Sanitarium. He reported that, during the years , the state mental hospital achieved percent cures or satisfactory discharges, while Forest Park reported a 65 percent cure satisfactory discharge rate. The judge attempted to persuade the state hospital in North Dakota to include chiropractors on its staff, but he was unsuccessful.

38
Clearview Patient “Acute mania. Male medical student, age 22. Became violent after an accident to his neck while playing football. Suffered acute hallucinations. M.D. diagnosed acute mania. Papers signed for subject’s commitment. Mother, who had visited asylums in the course of church work, vigorously objected, declaring, in effect, that her son would be better off dead. Patient came under chiropractic care…immediate improvement noted following first adjustment. Subject recovered in four weeks. Returned to Harvard University to complete studies.

39
Dr. Charles Mayo Dr. Ted Frigard DC PhC
In the early 20th century, Dr. Charles Mayo, physician, surgeon, and co-founder of the famed Mayo Brothers Clinic in Rochester, Minnesota, brought his wife for treatment to the Dr. B.J. Palmer Chiropractic Research Clinic in Davenport, Iowa.

40
Dr. Mayo had taken his wife to other physicians, including doctors in Europe, all distinguished diagnosticians and specialists. Dr. P.L. Poulsen of the BJPCC staff informed me that those medical specialists had agreed upon a diagnosis – osteochondromatosis of the knee joint. They had tried everything medical to heal Mrs. Mayo, but all treatment had failed.

41
Mrs. Mayo received chiropractic care for several months and returned home well. Dr. Mayo stated that it was impossible to get well with what Dr. Palmer did, yet he also admitted that she was well.

42
Palmer vs Mayo I was on the staff of the B.J. Palmer Chiropractic Clinic in Although “Dr. Charlie” had passed away in 1939, during that time, 60 to 80 percent of our patients were referred by “someone” on the staff of the Mayo Clinic.

43
Innate Adaptation Spinal cord or brain stem will conform to shape of foramen magnum and posterior atlas ring, anterior malformation little change.

44
Upper Cervical Neurology
There are 10 times more joint mechanoreceptors from C-1-3 than any other area of the spine. These receptors from C-1-3 synapse monosynaptically to the cerebellum and vestibular nucleus. These centers have a huge influence on equilibrium and relating the spine to the position of the skull. By synapsing monosynaptially the upper cervical spine has a major influence on these centers (more so than any other are of the spine). Dr. Dan Murphy Beacon June/July 2001
. Dr. Dan Murphy Beacon June/July")
47
Current Concepts of Causes Of Vertebral Subluxations
1) Meniscoids interarticular adhesions were first found in joints Synovitis, inflammation of the lubricating sacs in the joints, allows the cartilage called meniscoid flaps to shift and fold into the joints when bending, causing the joint to lock. Sensory nerves within the joints can produce pain. Spinal adjustments open the joints and allows the meniscoids to withdraw. 2) Joint Adhesions Fibrotic tissue/sear tissue develops in the joints that have restricted motion. Fibrosis limits motion, attracts calcium ions, and does not adapt to abrupt weather changes. Chiropractic adjustments break the adhesions and gradually restores mobility to the joint structures. 3) Capsular Fibrous Crosslinkings - Collagen fibers restrict pliability of the joints. New collagen tissue forms bridges across crossing fibers resulting in adhesions that hamper stretching. Foreman and Croft "Acceleration/Deceleration syndrome.
 Meniscoids interarticular adhesions were first found in joints Synovitis, inflammation of the lubricating sacs in the joints, allows the cartilage called meniscoid flaps to shift and fold into the joints when bending, causing the joint to lock. Sensory nerves within the joints can produce pain. Spinal adjustments open the joints and allows the meniscoids to withdraw. 2) Joint Adhesions Fibrotic tissue/sear tissue develops in the joints that have restricted motion. Fibrosis limits motion, attracts calcium ions, and does not adapt to abrupt weather changes. Chiropractic adjustments break the adhesions and gradually restores mobility to the joint structures. 3) Capsular Fibrous Crosslinkings - Collagen fibers restrict pliability of the joints. New collagen tissue forms bridges across crossing fibers resulting in adhesions that hamper stretching. Foreman and Croft Acceleration/Deceleration syndrome.")
48
Soft Tissue Repair Healing of ligaments (and other soft tissues) occurs with fibrous repair (scar tissue) rather than by regeneration of damaged tissue (26).
 occurs with fibrous repair (scar tissue) rather than by regeneration of damaged tissue (26).")
49
Phase 1 (acute inflammatory phase): lasts up to 72 hours.
Phase 2 (repair phase): lasts from 48 hours to six weeks Phase 3 (remodeling phase): lasting from three weeks to 12 months or more Healed ligaments contain immature type III collagen which is deficient in cross-links and the quantity of fibers is less than in a normal ligament which is composed chiefly of type I collagen (26).
: lasts from 48 hours to six weeks. Phase 3 (remodeling phase): lasting from three weeks to 12 months or more. Healed ligaments contain immature type III collagen which is deficient in cross-links and the quantity of fibers is less than in a normal ligament which is composed chiefly of type I collagen (26).")
53
A D.C., Palmer West graduate, called me on and stated that she would like to observe and learn more about upper cervical and Blair. She said that 3 of her classmates had set up practice in the Korean section of L.A. and had established hospital privileges in the Orthopedic Surgical Ward at a local hospital. They are producing such remarkable results that the surgical rates are dropping and the hospital is starting to lose money. Recently they were out to dinner and received an urgent call to return to the hospital. After rushing back to the hospital they were shown a paraplegic patient that had been unable to walk for 7 years and observed him ambling down the hallway. The entire staff and doctors all wondered aloud "What did you do to him?".

54
Chiropractic Facts MRI and Asymptomatic Patients
MRI examinations were performed on 98 asymptomatic patients. Only 36% had normal discs at all levels. 52% had a bulge at one level. 27% had a disc protrusion, 38% had abnormalities at more than 1 disc level. New England Journal of Medicine July 14,1994

55
Smoking and Chiropractic
A patient I had known for 10 years had her husband call in to cancel her remaining appointments due to the fact that she had been diagnosed with terminal lung cancer. After smoking 2 packs/day the cigarettes took their toll and she was told to pick out her gravesite. Upon having exploratory surgery, the doctors were able to arrest the condition and give her a new lease on life. She returned to my office two months later-reeking of smoke!

56
X-ray All Patients Years ago an elderly man entered my office complaining of a stiff neck similar to one his chiropractor quickly fixed 10 years earlier. The patient did not want x-rays. After some heated exchanges, I x-rayed his C-sp and discovered he suffered from an osteolytic cancer of the bone that had consumed the entire posterior ½ of the axis. Needless to say he was not adjusted, was referred to his family physician, and unfortunately died 1 week later. The lesson: If I had adjusted him-the family and community would blame both me and the profession of chiropractic for his demise. Always xray before you adjust!

57
Functional MRI A new diagnostic tool known as a functional MRI may be on the market soon. This MRI shows the actual electrical firing of the brain and should be a great tool for disorders such as epilepsy, learning disabilities,... A volunteer was asked to wiggle his ankle while they performed the MRI. Massive firing was noted on the contralateral side with minimal firing on the ipsilateral side of the brain while performing ankle motion. Following an adjustment, he wiggled the same ankle and this MRI showed no firing on the ipsilateral side and minimal on contralateral. It seems that when a patient is subluxated, the body is forced to inefficiently rewire the circuits. The conclusion of the study "Adjustments improve brain efficiency" Christopher Kent, D.C.

58
Cerebellar Function and Emotional Disturbances
Dr. Nicholi Bogduk performed studies injecting chemicals into the facets of the cervical spine and found that the pathways are disturbed ascending up the cord, to the thalamus, and into the cerebellum. This area was originally thought to merely control gait and balance. Now the thinking seems to relate that region to emotion, joy, happiness,... Therefore, disturbances to the C-sp could certainly produce emotional disturbances, depression,.. and Dr. Bogduk concluded that correction of these cervical lesions could help reverse these emotional disturbances. Dr. Dan Murphy Whiplash and Spinal Trauma Seminar

59
Monkey Experiments on the Brain Stem
While discussing the short leg syndrome or contractured leg with a neurologist, he stated that they did research at his university in which a stylus was used to destroy the brain stem cells and each of the monkeys has their arm draw up claw-like across their chest and the pelvis contract extensively. This is permanent spinal cord damage. Then they took another group of monkeys and irritated the brain stem cells but did not destroy them. Each of these monkeys had one shoulder and the pelvis contract unilaterally. Dr. Sateesh Apte

60
UPPER CERVICAL MYTHS (1) Patients won't accept upper cervical concept. This really means the Dr. doesn't accept upper cervical concepts. Patients don't care what therapy is invoked. They just want results! (a) eg Patient on thyroid would not accept increased dosages with each office visit. They would demand objective testing be done to determine the NEED for treatment. (b) Come back when your in pain. How do I know when I'm out? First sx of cardiac problem is a fatal infarction in 31 % of the cases.
 Patients won t accept upper cervical concept. This really means the Dr. doesn t accept upper cervical concepts. Patients don t care what therapy is invoked. They just want results! (a) eg Patient on thyroid would not accept increased dosages with each office visit. They would demand objective testing be done to determine the NEED for treatment. (b) Come back when your in pain. How do I know when I m out First sx of cardiac problem is a fatal infarction in 31 % of the cases.")
61
(c) Adjustment means fix, treatment means therapy!
(d) If patient is adjusted each visit = therapy. Do they really need adjustments 3 times a week for 6 months? Dr. Crowder said "Upper Cervical is the only full spine technique." After you have made 5 full spine adjustments, how do you know you didn't miss one.
 If patient is adjusted each visit = therapy. Do they really need adjustments 3 times a week for 6 months Dr. Crowder said Upper Cervical is the only full spine technique. After you have made 5 full spine adjustments, how do you know you didn t miss one.")
62
(3) Upper Cervical is hard on you physically.
(2) Patients like to hear/feel the adjustments. My father used to try rotary type adjustments and I'd tense too much. (Who would you trust more than a parent) Toggle was no problem. (3) Upper Cervical is hard on you physically. (a) Must keep yourself fit. (b) Do uc exercises daily (c) Not doing lumbar rolls (d) Don't be afraid to refer out those not responding. EG Bud had a bad disc from jumping of ramp. No change in 2 weeks with constant lb and antalgic. Kaiser hadn't taken MRI. Referred to full spine D.C. keep it in the family.
 Patients like to hear/feel the adjustments. My father used to try rotary type adjustments and I d tense too much. (Who would you trust more than a parent) Toggle was no problem. (3) Upper Cervical is hard on you physically. (a) Must keep yourself fit. (b) Do uc exercises daily. (c) Not doing lumbar rolls. (d) Don t be afraid to refer out those not responding. EG Bud had a bad disc from jumping of ramp. No change in 2 weeks with constant lb and antalgic. Kaiser hadn t taken MRI. Referred to full spine D.C. keep it in the family.")
63
(4) Everyone isn't for you
(4) Everyone isn't for you. Have you ever met someone you disliked immediately? This will happen occasionally for you patients regarding you. How do you spot it? (a) Your answers aren't fulfilling. Each of your answers bring up 2 questions. (b) Looks for discounts
 Everyone isn t for you. Have you ever met someone you disliked immediately This will happen occasionally for you patients regarding you. How do you spot it (a) Your answers aren t fulfilling. Each of your answers bring up 2 questions. (b) Looks for discounts.")
64
(5) Patient’s have different Priorities
(a) eg Mr. L -ins doesn't cover. Lives in 2 million dollar house, retired at 50 and drive a Lamborghini. Value of care isn't there in his mind. Left after re-exam. Returned a week later because of return of sx. Able to run 3 miles for the first time in years but still doesn't value care. (b) Mr H., janitor, felt upper cervical was so special he had wife and children under Dr. Muncy's care despite cost and didn't request any discount. He valued the care!
 eg Mr. L -ins doesn t cover. Lives in 2 million dollar house, retired at 50 and drive a Lamborghini. Value of care isn t there in his mind. Left after re-exam. Returned a week later because of return of sx. Able to run 3 miles for the first time in years but still doesn t value care. (b) Mr H., janitor, felt upper cervical was so special he had wife and children under Dr. Muncy s care despite cost and didn t request any discount. He valued the care!")
65
(c) Ask transfers if they were pleased with their previous care and then have them describe the care. Try to refer that patient to a similar D.C. in your community that you trust.(When I practiced in SF, first couple I saw wanted a diversified Palmer D.C. with PT-they weren't pleased with Upper Cervical. Refunded much needed money and referred out). If they were satisfied with previous care dodge the "negative bricks" and send them to a DC who does similar work.
. If they were satisfied with previous care dodge the negative bricks and send them to a DC who does similar work..")
66
(5) Patients want to be addicted to adjustments.
(a) From a business standpoint, patient can't afford to bring in other family members (using up all disposable income) Often that family member is a "test case" for the remaining family. If the first member isn't substantially better, the rest of the family doesn't get to benefit from chiropractic. Getting better vs getting well. (b) Dr. can't take time off because of patients needing that weekly adjustment.
 From a business standpoint, patient can t afford to bring in other family members (using up all disposable income) Often that family member is a test case for the remaining family. If the first member isn t substantially better, the rest of the family doesn t get to benefit from chiropractic. Getting better vs getting well. (b) Dr. can t take time off because of patients needing that weekly adjustment.")
67
(6) Patients want you to spend more time with them
(6) Patients want you to spend more time with them. Patients are in as much of a hurry as you are. They have 20 things to do the day of their visit and you are # 5 on that list. They don't want to talk about their golf game or your skiing skills. They want to talk about their condition, get their care, and get out of there. Handful of patients leave the rest area early and can't figure out why they don't hold well. Do not keep them waiting in your reception room! Do some kind of post check so you don"t hear. "you didn't get it"& I shouldn't be charged". (7) Can't make a living. Many upper cervical doctors see patients per day with minimum stress.
 Patients want you to spend more time with them. Patients are in as much of a hurry as you are. They have 20 things to do the day of their visit and you are # 5 on that list. They don t want to talk about their golf game or your skiing skills. They want to talk about their condition, get their care, and get out of there. Handful of patients leave the rest area early and can t figure out why they don t hold well. Do not keep them waiting in your reception room! Do some kind of post check so you don t hear. you didn t get it & I shouldn t be charged . (7) Can t make a living. Many upper cervical doctors see patients per day with minimum stress.")
68
Glaucoma and Chiropractic
Recently a patient stated to me that she was dissatisfied with her progress. This 77 year old female suffers from advanced degenerative osteoarthritis that is especially troublesome in both shoulders. Because cartilage cannot regenerate, it is questionable that the constant shoulder pain can resolve. Medications are of little value. On her most recent office visit she stated that "I'm in so much pain, I don't know why I'm still coming in!"

69
I told her that despite the minimal progress in the shoulders, it is imperative that the remainder of her body have a proper nerve supply so that those areas also don't degenerate. She was not pleased or satisfied with this comment. On her next visit she said she had something to tell me. She suffers from glaucoma and stated that despite 4 years of medication she couldn't get the interocular pressure below 23 lbs. (17 is the high normal) Continued high ocular pressure damages the retina and causes loss of visual field) On her most recent visit to the opthomologist, he was startled to find that the pressure had dropped from 23 to 9 lbs. He knew the medication wasn't responsible for the change because she had been on it for years with little results.
 Continued high ocular pressure damages the retina and causes loss of visual field) On her most recent visit to the opthomologist, he was startled to find that the pressure had dropped from 23 to 9 lbs. He knew the medication wasn t responsible for the change because she had been on it for years with little results..")
70
The patient stated that at that moment she remembered what I had said about all cells needing a proper nerve supply. She personally feels the chiropractic care is the reason for the changes in her glaucoma. The lesson is that there is "limitation of matter" but keep focused on the objective-bringing the body to maximum potential!

71
Wednesday Morning I usually take Wednesdays off but traditionally stop by the office while heading out of town. We had three messages on the recorder and they went as follows:

72
(1) One patient had his wife call because he was lying flat on the bathroom floor since 4: 00 am. He had gotten up to go to the bathroom and while making the turn into the bathroom, felt a sharp pain in the L. SI region and fell to his knees. When I came into the tiny room he was on his back with an ice pack wedged underneath. I removed the ice pack and straightened him as best I could to get an NCM scan on his neck-definitely in pattern! The leg check showed a R 5/8" short leg (usually it is 3/8") Based on all I'd seen, a PIR adjustment was given. It took all my strength and his wife's to turn him over, lift him up, and gradually move him to a firm chair. He received a lecture about missing his appointment 2 days earlier. The pain subsided quickly.
 Based on all I d seen, a PIR adjustment was given. It took all my strength and his wife s to turn him over, lift him up, and gradually move him to a firm chair. He received a lecture about missing his appointment 2 days earlier. The pain subsided quickly..")
73
(2) This patient is a top notch engineer in the wireless industry and travels the world as a representative of his company. When his neck subluxates, travel "pile drives" his neck producing cervicogenic pain and intense headaches. He got a last minute call that he was flying to Hong Kong and knew his neck wasn't right. The ASR atlas adjustment produced rapid easing of the neck muscles and he knew the flight wouldn't be his undoing.

74
(3) This 55 year old female is highly ranked in her firm but has had to perform the duties of three people over the past year and the emotional stress was taking a heavy toll. Constant neck pain, dizziness, T-sp and L-sp. Pain, migraines, and depression resulted from this persistent onslaught. She stated that her husband was going away the next weekend and she was considering suicide because she couldn't take the pressure and felt she wouldn't be missed. She was examined, adjusted, a MFC/psychologist was called, and she was placed on 4 weeks TTD. All in a days work!

75
Neurophysiologic Basis
Infrared imaging detects and analyzes the cutaneous infrared emissions of the body. These surface thermal patterns are a direct reflection of the sympathetic and sensory nervous system's control over the dermal microcirculation (1, 4, 10, 15, 16). The main controlling factor, however, is the sympathetic division. This division of the autonomic nervous system controls the vasodilatory and vasoconstriction action of the body's arterial supply. Theories espoused around the turn of the century, and before, professed that the source of this surface heat came from internal areas of the body (chiropractic - heat from nerves, medicine - heat from diseased organs).
. The main controlling factor, however, is the sympathetic division. This division of the autonomic nervous system controls the vasodilatory and vasoconstriction action of the body s arterial supply. Theories espoused around the turn of the century, and before, professed that the source of this surface heat came from internal areas of the body (chiropractic - heat from nerves, medicine - heat from diseased organs).")
76
Landmark research on the origin of skin surface temperature regulation has since clarified these theories (17). In several studies, independent heat sources of significant magnitude were placed at varying depths under the skin and an attempt to detect the heat source was made with sensitive thermal instruments. It was found that if a heat source was placed 5 mm or more under the skin it could not be detected. Consequently, if skin surface temperatures are altered in any way, it must be a direct reflection of the controlling factors involved in the regulation of the dermal microvasculature.

77
In the absence of thermal symmetry, there are two types of temperature variations seen on infrared imaging: hyperthermia (increased thermal emissions) or hypothermia (decreased thermal emissions). This absence of thermal symmetry is defined as a difference in temperature when one side of the body is compared to the other, in specific terms a temperature differential, or Delta-T. These differentials produce characteristic thermal patterns that can be recorded, analyzed, and graphically displayed by digital infrared imaging systems. A simplified mechanism for these two thermal displays is summarized below. Hypothermic Emissions - Activation of sympathetic nerve fibers, via reflexogenic responses from afferent mechanoreceptor and/or nociceptor input from spinal joints (subluxation/ biomechanical aberration) (Figure A), causes vasoconstriction along the dermal
 (Figure A), causes vasoconstriction along the dermal.")
78
microcirculation of one or more neurotomes
microcirculation of one or more neurotomes. This will result in a decreased thermal emission (hypothermia) at the paraspinal and dermatome level. This is the most common result of chronic spinal neuropathophysiologic conditions (i.e. long-standing subluxations, etc.).
 at the paraspinal and dermatome level. This is the most common result of chronic spinal neuropathophysiologic conditions (i.e. long-standing subluxations, etc.).")
80
Figure A - Paraspinal sensory and vasomotor nerve pathways
Figure A - Paraspinal sensory and vasomotor nerve pathways. Afferent somatic sensory neurons ( ) may dichotomize, sending axons into different nerves. Somatic sensory nerves may also send branches to synapse with postganglionic sympathetic nerves (-----), or they may even branch to innervate visceral organs (---- ), thus transmitting both visceral and somatic sensation. Afferent visceral nociceptive fibers (- • -) may send branches to synapse with postganglionic sympathetic nerve cells, producing vasomotor responses. Preganglionic sympathetic fibers (••••••); postganglionic fibers ( ). (Reprinted with permission from J. Christiansen, Ph.D)
 may dichotomize, sending axons into different nerves. Somatic sensory nerves may also send branches to synapse with postganglionic sympathetic nerves (-----), or they may even branch to innervate visceral organs (---- ), thus transmitting both visceral and somatic sensation. Afferent visceral nociceptive fibers (- • -) may send branches to synapse with postganglionic sympathetic nerve cells, producing vasomotor responses. Preganglionic sympathetic fibers (••••••); postganglionic fibers ( ). (Reprinted with permission from J. Christiansen, Ph.D)")
81
Hyperthermic Emissions
Hyperthermic emissions are mainly caused by one of two neurophysiologic mechanisms. In the acute stage of an injury, or spinal neural irritation (as outlined in the paragraph above), antidromic stimulation of nociceptive C-fibers cause a peripheral release of Substance P. Substance P acts upon the arterial receptors causing vasodilatation. This in turn causes an increase in surface temperatures. Christiansen (18) was the first to recognize the involvement of Substance P and the axon reflex in the production of a thermographic image. The second cause of hyperthermic emissions is a decrease or cessation of sympathetic activity. This results in vasodilatation due to a loss of normal dermal vascular control.
, antidromic stimulation of nociceptive C-fibers cause a peripheral release of Substance P. Substance P acts upon the arterial receptors causing vasodilatation. This in turn causes an increase in surface temperatures. Christiansen (18) was the first to recognize the involvement of Substance P and the axon reflex in the production of a thermographic image. The second cause of hyperthermic emissions is a decrease or cessation of sympathetic activity. This results in vasodilatation due to a loss of normal dermal vascular control.")
82
In summary, it can be simply stated that the purpose of infrared imaging is to monitor the function of the nervous system. Since the amount of blood passing through the skin is directly controlled by the nervous system, the temperature of any one area of the skin becomes a direct reflection of the neurologic control of that area. Abnormal or normal temperatures of the skin then become an indicator of normal or abnormal. neurologic function.

83
Physiologists advise that there is no normal skin temperature, only a normal temperature range. Skin temperatures continually change within a very limited range as the amount of excess internal heat changes with an ever-shifting metabolic rate and adaptation to environmental changes. With all physiologic systems: normal function is a continuing adaptive process (homeostasis).
..")
84
This physiologic process can be monitored with digital infrared imaging systems. Patients with normal neurologic function will display almost no thermal differentials (straight-line readings) or very minor deviations that change from office visit to office visit. When interference to normal neurologic control (homeostasis) occurs, these changing differentials become static. Once these temperature differentials no longer display normal adaptations, the patient is said to be "in pattern".
 or very minor deviations that change from office visit to office visit. When interference to normal neurologic control (homeostasis) occurs, these changing differentials become static. Once these temperature differentials no longer display normal adaptations, the patient is said to be in pattern ..")
85
Due to the unique functional anatomy of the sympathetic nervous system, the exact locations of abnormal temperature differentials cannot be used as indicators for the precise source of neural dysfunction. Thus, using abnormal paraspinal Delta-Ts as segmental indicators for spinal adjusting, without correlative examination procedures, would be incorrect. However, these infrared readings serve as the single most valuable diagnostic entity indicating when neuropathophysiology exists, and perhaps more importantly when it has been eradicated.

86
Consequently, the use of paraspinal infrared imaging becomes a sensitive outcome measure for the value of the adjustment. We are able to monitor the nervous system's function as an indicator as to when an adjustment is needed, when an adjustment was actually made, and when an adjustment is not indicated.

87
Thermographically Measured Normal Skin Temperature Asymmetry in Human Male Cancer 1975 Silberstein EB, Bahr GK, Kattan J. Inasmuch as skin temperature is always changing in response to multiple inputs, absolute skin temperature measurements have little significance. However, departures from “normal” body symmetry may have diagnostic importance… Note-Thermal symmetry assessment has been used in the chiropractic profession since Hippocrates with his statement, “Should one part of the body be hotter or colder than the rest, then disease is present in that part.”.

88
Safety in Cervical Spinal Adjusting Arterial Dissections
A paper published in the October 2, 2001 issue of the Canadian Medical Association Journal (CMAJ) by Scott Haldeman, D.C.w M.D., Ph.D.. Paul Carey, et al (Arterial Dissections following Cervical Manipulations; The Chiropractic Experience") reports that the chances of arterial dissection after cervical manipulation is approximately 1 in 5.85 million manipulations,
 by Scott Haldeman, D.C.w M.D., Ph.D.. Paul Carey, et al (Arterial Dissections following Cervical Manipulations; The Chiropractic Experience ) reports that the chances of arterial dissection after cervical manipulation is approximately 1 in 5.85 million manipulations,")
89
“The likelihood that a chiropractor will be made aware of an arterial dissection. following a cervical manipulation is approximately 1:806 million office visits, 1:585 million cervical manipulations, 1:1430 chiropractic practice careers."

90
Dr. Carey said that the study supports recent research published in the Canadian Medical Association Journal by the Institute for Clinical Evaluation Studies, which found that the incidence of stroke associated with neck adjustments is so rare that it was not possible for the researchers to establish a meaningful rate of occurrence for the high number of. adjustments that are performed. Dynamic Chiropractic November 5, 2001

91
C-6.7 Degeneration Linked to Cervical Pain
Degeneration in the cervical spine occurs as patients get older,even if they have no initial symptoms. Research has not established whether pain is more likely to develop in relation to those with degeneration. In this 10 year study, 200 asymptomatic subjects (Half men, half women) had initial lateral radiographs taken.
 had initial lateral radiographs taken.")
92
10 years later, 159 of the participants were included in the follow-up involving additional roentgenograms and a pain questionnaire. Results: Subjects who developed degenerative changes at C-6,7 were four times more likely than their peers to suffer cervical pain. Pain developed in 15% of the follow-up participants, and there was an increase in subluxations and degenerative changes overall, as the author suspected. The average age of those with degenerative changes was 52 years.

93
The author concludes, “Intuitively, most clinicians believe that there is a connection between degenerative changes and symptoms; however, establishing that as a fact has been frustratingly elusive.” Gore DR Roentgenographic findings in the cervical spine in asymptomatic persons: A ten-year follow-up study. Spine 2001:26(22) PP
 PP")
94
A Three Dimensional Model of Vertebral Subluxation Dr
A Three Dimensional Model of Vertebral Subluxation Dr. Christopher Kent December The Chiropediatric Times

95
Dyskinesia-Dyskinesia refers to distortion or impairment of voluntary movement. Spinal motion can be reliably measured and alterations of regional ranges of motion may be associated with vertebral subluxations. Dysponesis-Dvsponesis is evidenced by abnormal tonic muscle activity. Dysponesis refers to a reversible physiopathological state consisting of errors in energy expenditure, which is capable of producing functional disorders. Dysautonomia-The autonomic nervous system regulates the actions of organs, glands, and blood vessels. Acquired dysautonomia may be associated with a broad array of functional abnormalities. Autonomic dystonia may be evaluated by measuring skin temperature differentials.

96
B.J. Palmer developed and used a system of skin temperature analysis called ``pattern analysis." Persons free of neurological interference tend to display skin temperature readings which continually change, but when the vertebral subluxation and interference to normal neurological function appear on the scene, these changing differentials become static. They no longer display normal adaptability and the patient is said to be "in pattern."

97
Director of the BJ Palmer Chiropractic Research Clinic
Dr. Lyle Sherman Director of the BJ Palmer Chiropractic Research Clinic

98
Lyle Sherman,D.C. Head of the B.J. Palmer Research Clinic
BJ Palmer’s Personal Chiropractor 1) Sherman College of Straight Chiropractic named after him 2) X-ray professor excited about this new condyle concept 3) Stated directly to Dr. Blair that the Blair Torqued adj. was the correction was the adjustment required to be admitted into B.J.'s Clinic.
 Sherman College of Straight Chiropractic named after him. 2) X-ray professor excited about this new condyle concept. 3) Stated directly to Dr. Blair that the Blair Torqued adj. was the correction was the adjustment required to be admitted into B.J. s Clinic.")
99
Drugs vs. Alternative Health Care
Dr. Ronald Lawrence, assistant clinical professor, UCLA School of Medicine, noted: "The big drug companies routinely provide medical schools with free equipment; computers, supplies, seminars; as well as large grants of money. In return for this support, the medical schools refuse to teach courses of natural medicine and nutritional therapy. This is tragic, because these kinds of safe, natural alternatives can help alleviate many types of health problems without dangerous side effects. As a result, most physicians only learn to treat symptoms without addressing the underlying disease.

100
Drugs vs. Alternative Health Care
Whenever doctors suggest some kind of pharmaceutical drug as the solution to medical problems, remember that they are only doing what they were taught in school: "Treat medical problems with drugs and if that doesn't work, well, there's always surgery."

101
Patient Satisfaction A study released in 1995 by the Foundation for Chiropractic Education and Research (FCER) reveals that patients are very satisfied with care they receive from their chiropractors. Research Dimensions, Inc. (RDI), a Richmond, Virginia-based firm, completed the study in December of 1994. Major findings of the RDI study are: (1) 99% of the respondents indicated that they were either confident or very confident that their chiropractor had diagnosed their problem correctly;
 reveals that patients are very satisfied with care they receive from their chiropractors. Research Dimensions, Inc. (RDI), a Richmond, Virginia-based firm, completed the study in December of Major findings of the RDI study are: (1) 99% of the respondents indicated that they were either confident or very confident that their chiropractor had diagnosed their problem correctly;")
102
Patient Satisfaction (2) 99% of the respondents indicated that they were satisfied, or very satisfied with the chiropractic treatment they received; (3) 93% responded that their physical problem or condition had improved as a result of chiropractic care; (4) 93% of the responding said that chiropractic care contributes to a healthier, more fit lifestyle; (5) 71% of those responding indicated that they were taking less medication as a result of chiropractic care.
 99% of the respondents indicated that they were satisfied, or very satisfied with the chiropractic treatment they received; (3) 93% responded that their physical problem or condition had improved as a result of chiropractic care; (4) 93% of the responding said that chiropractic care contributes to a healthier, more fit lifestyle; (5) 71% of those responding indicated that they were taking less medication as a result of chiropractic care.")
103
LIMITATIONS TO MOTION PALPATION
Manual palpation techniques have been used for more than a century to assess joint motion. While articular facet asymmetry of the upper cervical spine has been considered in relation to joint disease, the effects of such asymmetry on joint motion require further investigation.

104
To that end, a study of six human cervical spine specimens explored motion palpation of joint restrictions and the implied link to disease at the C1/C2 level. Forces (5-25N) were applied along the mediolateral axes, and the corresponding displacement along three axes was documented. Specimen geometry and asymmetry were obtained by way of plain radiographic film and gimbal apparatus. Results: Each of the six specimens displayed different behavior and different degrees of asymmetry; asymmetrical and discontinous force-displacement correlations were linked to anatomic asymmetry that appeared to be of natural occurrence.

105
The authors caution that clinicians attempting to palpate vertebral motion should not assume that perceived restriction indicates pathological motion; it may in fact reflect normal anatomy. The results of this study challenge the assumptions of palpation theory that joints are symmetrical and therefore should feel symmetrical upon motion palpation. Ross JK, Bereznick DE, McGill SM. Atlas-axis facet symmetry: implications in manual palpation. Spine, June 15, 1999:24(12), pp
, pp")
106
Gutmann One name which crops up in nearly every German bibliography of chiropractic is that Dr. G. Gutmann, of Hamm. He tells how he selected two types of cases. The first type was the chronic case of low back disability, previously given special baths, massage, novocaine injections, a corset, a disc operation, and other methods-all without result. In a series of 38 such cases, 30 were so greatly improved that they could throw away their corset, and, of these, 16 remained entirely free from pain. The average number of adjustments per case was 2.3. It is worthy of note that 12 of the 16 cases obtaining complete relief received only upper cervical adjustments.

107
In a second series of cases of the same type, 57 cases who not did have compensation claims pending, complete recovery or marked improvement resulted in 66.6%, after an average of only 2.8 adjustments per patient. This he rightly considers all the more remarkable because of the neurotic tendency of many such patients to hold on to their symptoms in the hope of getting a favorable financial settlement. Gutmann's voluminous case histories and penetrating interpretation reflect a long period of intensive clinical research. In a particularly valuable study lie summarizes his conclusions regarding the influence of upper cervical subluxations on disease.

108
In a separate paper of his own, Sollman makes an important contribution to chiropractic theory. Bearing in mind the contention of certain chiropractors that the chief cause of subluxation is trauma, he inquired into the history of a large series of clinic patients exhibiting spinal changes to ascertain whether they, or any one connected with them, could recall any instance of major trauma in there experience. He found that in 95% of the cases no such history could be elicited.

109
1. Sudden or prolonged stimuli to the skin cold, heat, a blow, a draft) ;
2. Any chemical or thermal stimulus above the neural threshold to the mucous membranes of the gastro-intestinal tract (ice water, very hot drinks, alcohol); 3. A sudden intense stimulus of light to the eyes; 4. An explosive noise provoking a defensive reflex movement; 5. Any sharp concussion, to the head, producing upper cervical lesions;
; 3. A sudden intense stimulus of light to the eyes; 4. An explosive noise provoking a defensive reflex movement; 5. Any sharp concussion, to the head, producing upper cervical lesions;")
110
6. Any infectious focus affecting the corresponding spinal segment by long-sustained stimulation above the neural threshold; 7. Any rapid movement, like a look backward while driving a car; 8. Inhaled tobacco smoke, a micro-trauma to the vegetative nerves of the bronchial tree; 9. Intensive overwork-especially one-sided, prolonged and repetitive muscular activity; 10. Pressure conditions accompanying menstruation and pregnancy (venous stasis).
.")
111
What is FMS? FMS (fibromyalgia syndrome) is considered to be a widespread musculoskeletal pain and fatigue disorder for which the cause is still unknown. The term fibromyalgia means pain in the muscles, ligament and tendons-in other words, the fibrous tissues in the body. FMS used to be called the fibrositis syndrome, implying that there was inflammation in the muscles, but that has not been born out by research.
 is considered to be a widespread musculoskeletal pain and fatigue disorder for which the cause is still unknown. The term fibromyalgia means pain in the muscles, ligament and tendons-in other words, the fibrous tissues in the body. FMS used to be called the fibrositis syndrome, implying that there was inflammation in the muscles, but that has not been born out by research.")
112
Fibromyalgia and Neck Injury
A recent study from Israel found an increased prevalence of fibromyalgia among workers after a neck injury. "Fibromyalgia syndrome was 13 times more frequent following neck injury than following lower extremity injury," according to file new study. The results did not appear related to workers' compensation, litigation issues, or pre-existing chronic pain. (See Buskila et al ) Arthritis Rheumatism 1997
 Arthritis Rheumatism")
113
Mechanisms of C-0, C-1 Subluxations

114
Panjabi, Dvorak et al in 1998 stated that the average atlas rotation (nodding) is 24 degrees.
 is 24 degrees.")
115
Dvorak states that the total saggital angle of the two condyles (two convergence angles added together) is degrees. Inglemark 1947, Bernhard 1976

116
Dvorak states that the average angle between condyle to condyle (both slope angles from A-P) is 124 degrees in males and 127 degrees in females.
 is 124 degrees in males and 127 degrees in females.")
117
The Cervical Syndrome Jackson R.. Fourth Edition, 1977
The sympathetic nervous system plays a definite role in the picture of cervical nerve root irritation. The cervical nerve roots and their accompanying structures are subjected to irritation or compression within the canals which may be manifested by radicular symptoms. Normally nerve roots are free to move within the IVF ¼ to ½” as the dural sleeves are attached to the proximate bones. Nerve roots that have been injured or compressed by capsular thickening or bony encroachments cannot move within the IVF until they are freed by sharp dissection.

118
Tethering of the Central Nervous System Journal of Bone and Joint Surgery, Wall,EJ 1992
In 24 rabbits, the tibial nerve was exposed and stretched by 0%, 6%, or 12%. The strain was maintained for one hour. At 6% strain, the amplitude of the action potential had decreased by 70%. At 12% strain, conduction was completely blocked by one hour and showed minimal recovery. Note- This study also concluded that the neurological dysfunction was caused by mechanical deformation as opposed to anoxia.

119
Cross Section of the Spinal Cord

120
Dentate Ligament Cord Distortion Hypothesis It is probable that the elasticity of the dentate ligament dissipates with some stress, but chronic tension on a ligament may produced thickening and strengthening of the ligament, decreasing the ligament’s ability to damp the distortive forces before they can deform the cord. Kirk Eriksen, Upper Cervical Subluxation Complex

121
Anatomy and Hemodynamics Mechler FP, Review of Anatomy, Histology, and Clinical Significance of the Vertebral Artery in Health and Disease Chiropractic Research Journal (2);17-33 Between the atlas and axis, the vertebral arteries are directly covered by the obliquus capitus inferior and intertransversarii muscles, either of which can compress the artery during rotational movements. The compression may produced brainstem ischemia and transient neurological symptoms. Techniques of choice then, would be Gonstead (where tension is taken mainly by lateral flexion) or toggle recoil (which appears traumatic but has had NO accidents ascribed to it).
 or toggle recoil (which appears traumatic but has had NO accidents ascribed to it).")
122
An Anatomical Basis for Neck Tongue Synd
An Anatomical Basis for Neck Tongue Synd. Journal of Neurological Neurosurgical Psychiatry Bogduk N (3) ; The C-2 nerve roots and rami were dissected in five cadavers to explore the pathogenesis of Neck-Tongue Syndrome. The most likely cause of the simultaneous occurrence of suboccipital pain and ipsilateral numbness of the tongue is an abnormal subluxation of one lateral atlanto-axial joint with impaction of the C-2 ventral ramus against the subluxated articular processes. Thus the sensation of “numbness” in both Bell’s Palsy and Neck-Tongue Syndrome does not imply loss of touch and pain sensation but rather reflects the impaired function of the deep proprioceptive afferents.
 ; The C-2 nerve roots and rami were dissected in five cadavers to explore the pathogenesis of Neck-Tongue Syndrome. The most likely cause of the simultaneous occurrence of suboccipital pain and ipsilateral numbness of the tongue is an abnormal subluxation of one lateral atlanto-axial joint with impaction of the C-2 ventral ramus against the subluxated articular processes. Thus the sensation of numbness in both Bell’s Palsy and Neck-Tongue Syndrome does not imply loss of touch and pain sensation but rather reflects the impaired function of the deep proprioceptive afferents.")
123
Neck-Tongue Syndrome Journal of Manipulative and Physiological Therapeutics Cameron Borody, BSc,DC, June 2004, Vol. 27, Number 5 There are two categories of NTS: complicated-NTS due to the presence of an underlying disease process (inflammatory or degenerative) and uncomplicated-NTS (idiopathic or trauma related) This is a case study of a 24 year old female dancer with recurrent episodes of right sided neck pain associated with ipsilateral numbness of her tongue. Physical examination revealed a mildly painful restriction of rotation a the C-1-C-2 level with no muscular hypertonicity. Conclusion: UC manipulation can be efficacious for NTS.
 and uncomplicated-NTS (idiopathic or trauma related) This is a case study of a 24 year old female dancer with recurrent episodes of right sided neck pain associated with ipsilateral numbness of her tongue. Physical examination revealed a mildly painful restriction of rotation a the C-1-C-2 level with no muscular hypertonicity. Conclusion: UC manipulation can be efficacious for NTS.")
124
Arnold-Chiari Malformation Effects of Upper Cervical Subluxation Concominant with mild Arnold-Chiari malformation: a case study, Smith JL Chiropractic Research Journal Vol 1V, No. 2 Fall 1997 Arnold-Chiari (A-C) malformation is a variable congenital defect of the brainstem originally described in 1894. A 39 y/o female complained of intermittent bouts of fatigue, dizziness, facial numbness, ataxia, headaches, difficulty speaking, and diffuse arthralgias for 2 years. A type 1 A-C was discovered, determined to be incidental, and unresponsive to medical Tx. Use of manual side-posture upper cervical adjusting, the patient experienced substantial relief of her symptoms making medical intervention unnecessary.
 malformation is a variable congenital defect of the brainstem originally described in A 39 y/o female complained of intermittent bouts of fatigue, dizziness, facial numbness, ataxia, headaches, difficulty speaking, and diffuse arthralgias for 2 years. A type 1 A-C was discovered, determined to be incidental, and unresponsive to medical Tx. Use of manual side-posture upper cervical adjusting, the patient experienced substantial relief of her symptoms making medical intervention unnecessary.")
125
Epileptic Seizures, Nocturnal Enuresis, ADD Langley C Chiropractic Pediatrics Vol 1, No. 1 April 1994 Case study: An 8 y/o female with a history of epilepsy, heart murmur, hypoglycemia, nocturnal enuresis, and Attention Deficit Disorder (ADD) had been seen by five pediatricians, six psychiatrists, and 10 hospitilizations. The child was on Depakote, Depakene, Tofranil, and Tegretol. Difficult birth with cesarean section. MD’s told the mother that the girl would never ride a bike, nor have a normal childhood. She would wet the bed every night and have seizures per day. C-1,2 adjustments were given 3X/wk, eneuresis started to clear in two weeks and resolved in 6 mo. Seizures after a year reduced to 8-10 per week, released from psychiatric care “self managing”, and can now ride a bike, ice skate, roller blade,…like a normal child.
 had been seen by five pediatricians, six psychiatrists, and 10 hospitilizations. The child was on Depakote, Depakene, Tofranil, and Tegretol. Difficult birth with cesarean section. MD’s told the mother that the girl would never ride a bike, nor have a normal childhood. She would wet the bed every night and have seizures per day. C-1,2 adjustments were given 3X/wk, eneuresis started to clear in two weeks and resolved in 6 mo. Seizures after a year reduced to 8-10 per week, released from psychiatric care self managing , and can now ride a bike, ice skate, roller blade,…like a normal child.")
126
Cessation of Seizure Disorder: Correction of the Atlas Subluxation Complex Goodman R. Proceedings of the National Conference on Chiropractic and Pediatrics (ICA) 1991:46-56 When beginning chiropractic care a five year old girl was experiencing up to 70 seizures a day. She is now seizure-free and has her spine checked every 2-3 months.

127
Multiple Sclerosis (MS) and Parkinson’s Disease (PD) Reversed Progression with Upper Cervical Care Elser E, Journal of Vertebral Subluxation (JVSR) The Chiropractic Journal Sept. 2004 Data was compiled from 44 MS patients and 37 PD patients treated over the past five years. After treating upper neck injuries in 81 patients, 91% of the MS patients and 92% of the PD patients improved, suggesting a correction of neck injuries stimulated a reversal of MS and PD. Similar studies by this author have focused on migraine and cluster headaches, seizures, bipolar disorder, Tourette Syndrome, and ADHD, all of which have been linked to head and neck trauma by medical researchers.

128
Neurocalometer, Neurocalograph, Neurotempometer Research as Applied to Eight B.J. Palmer Chiropractic Clinic Cases L.W. Sherman Case # 1560 Epliepsy (grand mal) Age 24. He has had seizures since age 7, most convulsions occur at night averaging 1-5 every 24 hours. Phenobarbital had been taken for 17 years. Medication was discontinued at the start of care at the BJP Clinic. “Much of the reaction following reduction of nerve pressure was, in our opinion, withdrawal symptoms.” Following the first atlas adjustment, the seizures increased to 12,26,51,41,54,78,97, /day. The patient then reported five seizure-free months. Symptoms returned following dental work but after adjustment, disappeared. Patient eventually remained seizure-free.
 Age 24. He has had seizures since age 7, most convulsions occur at night averaging 1-5 every 24 hours. Phenobarbital had been taken for 17 years. Medication was discontinued at the start of care at the BJP Clinic. Much of the reaction following reduction of nerve pressure was, in our opinion, withdrawal symptoms. Following the first atlas adjustment, the seizures increased to 12,26,51,41,54,78,97, /day. The patient then reported five seizure-free months. Symptoms returned following dental work but after adjustment, disappeared. Patient eventually remained seizure-free.")
129
Neurocalometer, Neurocalograph, Neurotempometer, Research as Applied to Eight B.J. Palmer Chiropractic Clinic Cases L.W. Sherman Case #2348 Epilepsy Boy age 5 years March 1944 child has streptococci infection in inner ear. Started falling many times each day: often hurt himself. Child had a tonsillectomy, appendectomy, and hernia operation “since the trouble started.” Child had first adjustment and immediately post adjustment “child became more alert and his eyes started getting clearer.” Child was discharged and advised to be monitored by local chiropractor and if the NCM (pattern) returns, be re-adjusted. Patient held ORIGINAL adjustment and became seizure-free.
 returns, be re-adjusted. Patient held ORIGINAL adjustment and became seizure-free.")
130
Neurocalometer, Neurocalograph, Neurotempometer Research as Applied to Eight B.J. Palmer Chiropractic Clinic Cases L.W. Sherman Hydrocephalus Case #2887 Baby was diagnosed as hydrocephalus in a large university hospital and was brought in for Chiropractic soon after the diagnosis. Delay would have produced permanent distortion. MD noticed enlarged head on delivery and stated that there was “no hope for recovery.” A few days following the first adjustment, the skin on the head was looser and he was able to “wrinkle his brow.” Bowel and urine developed a strong odor, skin breaks out from poison in urine. The head reduced 1 ¾” in size. After a month, child was released to local chiropractor. A year later the child continued to do well. The child had one adjustment.

131
Autism- case study Rubinstein, HM Chiropractic Pediatrics Vol 1, No
Autism- case study Rubinstein, HM Chiropractic Pediatrics Vol 1, No.1 April 1994 This is a case study of a 7 y/o female diagnosed with Autism. The child has a history of sexual and physical abuse. The little girl would slowly turn in circles in place while singing an incomprehensible song with a glazed stare and blank expression. Spinal examination revealed a right posterior and superior C-1 with a frequency of about once a week. After ten months of care she was able to carry on conversations, carry out commands, dress and groom herself. Cognitive development progressed to where she was able to learn, read, and participate in public school.

132
Spinal Cord Stimulation for Palsies Waltz J. M
Spinal Cord Stimulation for Palsies Waltz J.M. Patient Care : Dr J. M. Waltz (M.D.) Director Department of Neurological Surgery, St. Barnabas Hospital, New York “In patients with cerebral palsy, upper cervical stimulation has repeatedly obtained unexpected benefits, such as decreased spasticity and marked improvement in motor control. Stimulation of C-2, C-3, and C-4 offers the best chance for overall improvement.”
 Director Department of Neurological Surgery, St. Barnabas Hospital, New York. In patients with cerebral palsy, upper cervical stimulation has repeatedly obtained unexpected benefits, such as decreased spasticity and marked improvement in motor control. Stimulation of C-2, C-3, and C-4 offers the best chance for overall improvement.")
133
Die Kopfgelenksblockierung des Neugeborenen Seifert J
Die Kopfgelenksblockierung des Neugeborenen Seifert J., Lewit K, Gutmann G Rehabilitacia Vol 8 Prague 1975 Among 1093 newborn 298 had upper cervical subluxation and early signs of infantile scoliosis.

134
Blocked Atlantal Nerve Syndrome in Infants and Small Children
Blocked Atlantal Nerve Syndrome in Infants and Small Children. Gutman G ICA Review 1990 July Originally published in German Manuelle Medzin (1987) Three case reports are reviewed to illustrate a syndrome that has so far received far too little attention, which is caused and perpetuated in babies and infants by blocked nerve impulses at the atlas. Included in the clinical picture are lowered resistance to infection, especially to ear, nose and throat infections, two cases of insomnia, two cases of cranial bone asymmetry, and once case each of torticollis, retarded locomotor development, retarded linguistic development, conjunctivitis, tonsilitis, rhinitis, earache, extreme neck sensitivity, insipient scoliosis, delayed hip development, and seizures.
 Three case reports are reviewed to illustrate a syndrome that has so far received far too little attention, which is caused and perpetuated in babies and infants by blocked nerve impulses at the atlas. Included in the clinical picture are lowered resistance to infection, especially to ear, nose and throat infections, two cases of insomnia, two cases of cranial bone asymmetry, and once case each of torticollis, retarded locomotor development, retarded linguistic development, conjunctivitis, tonsilitis, rhinitis, earache, extreme neck sensitivity, insipient scoliosis, delayed hip development, and seizures.")
135
The Atlas Fixation Syndrome in the Baby and Infant Gutmann G Manuelle Medizin 1987 25:5-10
Seven month old male baby with facial and skull asymmetry since the eighth week of life. After spinal adjustment slept well in all positions for the first time. “Skull becoming more symmetrical, facial symmetry cannot be noticed anymore.”

136
Kinematic Imbalances due to Suboccipital strain in Newborns (KISS Syndrome) Biedermann H. J. Manual Medicine ; More than 600 babies have been treated for suboccipital strain. The suboccipital strain included torticollis, fever of unknown origin, loss of appetite, and other symptoms of CNS disorders, asymmetrical development of the skull , hips, and extreme sensitivity of the neck to palpation. Most of the patients in the series required one to three adjustments before returning to normal. “Removal of the suboccipital strain is the fastest and most effective way to treat the symptoms…one session is sufficient in most cases. Manipulation of the occipito-cervical region leads to disappearance of problems…”

137
Upper Cervical Adjustment upon Normal Physiology of the Heart
Upper Cervical Adjustment upon Normal Physiology of the Heart. Tran AT, Kirby JD Journal of the American Chiropractic Association 1977 Adjustments of the upper cervical spine were found to have a hypotensive effect. A similar study from the Journal of the American Osteopathic Association 1969 entitled Effect of osteopathic manipulative therapy on autonomic tone as evidenced by blood pressure changes and activity of the fibrinolynic system by Fichera AP; Celander DR Manipulation of the cervical and thoracic vertebrae reduces moderate hypertension.

138
The efficacy of upper cervical chiropractic care on children and adults with cerebral palsy: a preliminary report. Collins KF et al Chiropractic Pediatrics (1) 13-15 Cerebral Palsy (CP) is the most prevalent lifelong development disability in the United States. Seven patients were tested-2 children, 5 adults All subjects in the study had improvements in many areas-decreased muscle spasticity, improved sleep patterns, decreased irritability/pain, and increased resistance towards infections. One child had four unsuccessful eye surgeries for strabisimus which cleared after two neck adjustments. The children were able to hold their heads up longer and made more attempts towards crawling. There was also improved clarity an d volume of speech in patients with speech and hearing problems.
 is the most prevalent lifelong development disability in the United States. Seven patients were tested-2 children, 5 adults. All subjects in the study had improvements in many areas-decreased muscle spasticity, improved sleep patterns, decreased irritability/pain, and increased resistance towards infections. One child had four unsuccessful eye surgeries for strabisimus which cleared after two neck adjustments. The children were able to hold their heads up longer and made more attempts towards crawling. There was also improved clarity an d volume of speech in patients with speech and hearing problems.")
139
Tourette Syndrome-a case study LaBarbera JA, ICA Pediatric Association Newsletter March/April 1998
A six y/o boy was diagnosed with Tourette syndrome whose presentation included eye-blinking, head shaking, mouth stretching, lateral eye movements, and some vocalizations occurring at a frequency of several times per minute. History revealed a head injury one month before he was diagnosed. Chiropractic evaluation included x-rays and heat pattern analysis which revealed C-0-2 subluxations. The C-1 subluxation was particularly large. “There was a noticeable change within 3 weeks of care. Symptoms continued to steadily improve. Within 4 months the patient was asymptomatic a majority of the time.”

140
The atlas fixation in the baby and infant Gutmann G
The atlas fixation in the baby and infant Gutmann G. Manuelle Medizin :5-10 Examination of 1,250 infants five days after birth showed over 25% were suffering from vomiting, irritability, and sleeplessness. Examination showed that 75% of these infants had cervical (neck) strain. Treatment frequency resulted in an immediate relief of the symptoms.
 strain. Treatment frequency resulted in an immediate relief of the symptoms.")
141
Sudden Deafness and Craniocervical Junction Hormann K, Weh L et al Laryngo-Rhino-Oto/ Morphological alterations of the craniocervical junction as a basilar impression, a ponticulus posterior, an atlas assimilation, an intervertebral narrowing, and spondylosis deformans were found radiologically…there was a statistically significant reduced mobility in the upper cervical spine in patients suffering from sudden deafness. There were especially high standards of deviation in the atlanto-occipital and atlanto-dental joints. These results indicate a correlation between sudden deafness and functional pathology of the craniocervical junction.

142
Brain Function; Chiropractic Medicine for the Rejuvenation of the Mind Gorman RF, 1983 Academy of Chiropractic Medicine Gorman, an ophthalmologist with interest in migraine, worked with Eric Milne, M.D. (a GP) who had interest in spinal manipulation. They discovered a wide range of physical and psychological conditions responding to chiropractic care and believed that most people are suffering from decreased brain functioning due to decreased flow of blood to the brain and that chiropractic spinal manipulation could relieve this problem. They feel that many people are functioning with diminished mental potential or are disabled by “mental illness” which has a simple physical cause.
 who had interest in spinal manipulation. They discovered a wide range of physical and psychological conditions responding to chiropractic care and believed that most people are suffering from decreased brain functioning due to decreased flow of blood to the brain and that chiropractic spinal manipulation could relieve this problem. They feel that many people are functioning with diminished mental potential or are disabled by mental illness which has a simple physical cause.")
143
PET and SPECT in whiplash syndrome: a new approach to a forgotten brain? Otte A et al Journal of Neurosurgical Psychiatry 1997;63: Whiplash patients have traditionally reported a number of symptoms that are related to brain function-i.e. loss of memory, vision changes, emotional changes. This study involved six patients suffering from whiplash syndrome and 12 normal controls. They gave everyone chemicals that reveal brain function when viewed by specialized equipment (PET & SPECT) which is similar to a CAT scan for the brain. In the patient group, there was “significant hypometabolism” or decreased brain function and hypoperfusion (anoxia) in the parieto-occipital regions on the r. & l. compared to the control group. “It is hypothesized that parieto-occipital hypometabolism may be caused by activation of nociceptive nerves from the UC spine.”
 which is similar to a CAT scan for the brain. In the patient group, there was significant hypometabolism or decreased brain function and hypoperfusion (anoxia) in the parieto-occipital regions on the r. & l. compared to the control group. It is hypothesized that parieto-occipital hypometabolism may be caused by activation of nociceptive nerves from the UC spine.")
144
Intervertebral Disc: Normal Age-Related Changes in MR Signal Intensity Radiology :385-8 Sether et al Discs without radial tears retain their normal height, color, and contour into the 7th and 8th decades of life. Discs with radial tears develop bulging and lose height, stability, color, and signal intensity. Therefore, we accept that a radial tear of the annulus fibrosis is the most reliable criterion of disc degeneration.

145
Specific Upper Cervical Chiropractic Care and Lung Function Kessinger R. Chiropractic Research Journal Vol IV 1997 This was a study of 58 patients to determine whether upper cervical (knee chest adjustment) as developed by Dr. B.J. Palmer, influenced pulmonary function. FEV-1 and FVC were measured before care and two weeks after care on a computerized auto spirometer. Of the 58 patients, 33 (57%) were considered to have “abnormal” lung function before care. The rest were within the normal group. 42% of the abnormal patient population actually tested within normal limits after the two week study. The normal group showed predictable improvement but not as dramatic as the abnormal group.
 as developed by Dr. B.J. Palmer, influenced pulmonary function. FEV-1 and FVC were measured before care and two weeks after care on a computerized auto spirometer. Of the 58 patients, 33 (57%) were considered to have abnormal lung function before care. The rest were within the normal group. 42% of the abnormal patient population actually tested within normal limits after the two week study. The normal group showed predictable improvement but not as dramatic as the abnormal group.")
146
Athletic Performance and Physiological Measures in Baseball Players following Upper Cervical Chiropractic Care: a pilot study Schwartzbauer J, Kolbert J. Hart, Zhang JVSR Vol. 1 No The athletic performance of university baseball players were assessed before, during, and after chiropractic care. Twenty players participated, divided into control and experimental groups, and had three sessions of athletic ability and physiological tests performed. The results showed a positive correlation between chiropractic adjustments and athletic performance. The chiropractic group also showed significant improvement in capillary count (oxygenation of tissues) at 5 and 14 weeks of care.
 at 5 and 14 weeks of care.")
147
The Effect of Manipulation (toggle recoil technique) for Headaches with Upper Cervical Joint Dysfunction: a pilot study Whittingham W et al JMPT July/Aug (6): Twenty-six patients (16 males, 10 females) all had chronic headaches with upper cervical joint dysfunction. Significant diminishing of severity and frequency of headaches reported in a large majority of the subjects (24 out of 26)
 all had chronic headaches with upper cervical joint dysfunction. Significant diminishing of severity and frequency of headaches reported in a large majority of the subjects (24 out of 26)")
148
The Effects of Specific Upper Cervical Adjustments on the CD4 Counts of HIV Positive Patients Selano JL et al Chiropractic Research Journal (1): 32-39 Five patients were adjusted and five were controls. After 6 months, in the control groups (not under chiropractic care) the CD4 levels declined by 7.96% while the group receiving chiropractic adjustments experienced a 48% increase in the CD4 cell counts. This indicates that correction of upper cervical subluxation could improve immunocompetence.
 the CD4 levels declined by 7.96% while the group receiving chiropractic adjustments experienced a 48% increase in the CD4 cell counts. This indicates that correction of upper cervical subluxation could improve immunocompetence.")
149
Multiple Sclerosis: The Effects of Chiropractic on MS
Multiple Sclerosis: The Effects of Chiropractic on MS. Kirby SL Chiropractic Research Journal 1994 Vol 3, No. 1 This is a case study of a 24 y/o female with the chief complaints of parethesia and tingling in the upper and lower extremities, stiffness in left arm and hand, and chronic fatigue. Neurologist diagnosed probable MS. Management of a case with symptomatology indicative of Multiple Sclerosis. The condition, which currently has no cure, responded favorably to chiropractic care using upper cervical approach to reduced a specific subluxation complex.

150
Visual Disturbances Bogduk stated that “stimulating the sympathetics results in pronounced decrease in carotid artery flow” and further said stimulation has been shown to “reduced blood supply to the retina in human subjects” Cephalgia 1981 Stephans and Gorman studied links between recoveries of vision and spinal manipulation suggesting that cerebral hypoperfusion (anoxia) “has been confirmed to be part of the upper spinal derangement”. JMPT June 1997 Vol. 19, Number 6
 has been confirmed to be part of the upper spinal derangement . JMPT June 1997 Vol. 19, Number 6.")
151
Visual Disturbances continued
Kessinger and Boneva carried out a study involving 67 subjects which investigated the relationship between upper cervical “specific” chiropractic care and changes in visual acuity. Results indicated “considerable evidence attests an association between visual disorders and head/cervical neck trauma.” Of the 67 subjects in this case, 59 had demonstrated a C-1 listing and 8 a C-2 listing. NB- Blair x-ray analysis was utilized by Dr. Kessinger. Journal of Vertebral Subluxation Research Jan

152
Visual Disturbances continued
Zhang et al provided information regarding improvement of visual disturbances in 83% of 111 cases treated over a period of seven years. Included in this group were 9 cases out of 12 in which blind eyes regained vision. The authors found a correlation between poor posture of the cervical spine and head (anterior head bearing) and visual disturbances. Journal of Traditional Chinese Medicine Sept. 1994 Murphy indicates that the posture control mechanism is affected in whiplash subjects causing vertigo, disturbed eye movements, and reading problems. Whiplash and Vision American Journal Clinical Chiro.1999
 and visual disturbances. Journal of Traditional Chinese Medicine Sept Murphy indicates that the posture control mechanism is affected in whiplash subjects causing vertigo, disturbed eye movements, and reading problems. Whiplash and Vision American Journal Clinical Chiro")
153
Visual Disturbances continued
Terrett and Gorman reported a news article in which a 4 year old girl, blind since age 9 months who recovered her sight after an adjustment of the first cervical segment (C-1) and discuss research with rabbits in which the removal of superior cervical ganglion in the neck resulted in disappearance of fluorescent fibers in the iris. In other words, the sympathetic nerve fibers affecting the iris originate in the nerve ganglion in the cervical spine! Thus, visual disturbances may well be caused by irritation of the sympathetic chain in the neck which may be corrected by cervical adjustments. Chiropractic Technique (2):43-54
 and discuss research with rabbits in which the removal of superior cervical ganglion in the neck resulted in disappearance of fluorescent fibers in the iris. In other words, the sympathetic nerve fibers affecting the iris originate in the nerve ganglion in the cervical spine! Thus, visual disturbances may well be caused by irritation of the sympathetic chain in the neck which may be corrected by cervical adjustments. Chiropractic Technique (2):")
154
Dermathermographic Scanning of an Infant
When using an infrared scanner on an infant or younger child, it is advantageous to have the patient draped over the parent’s lap. Often a child will arch his/her head backwards while being scanned. Forward movement of the head negates the effectiveness of the scan, whereas backward movement should have no impact. Start scanning at the C-7 level and stop when reaching base of the skull.

Similar presentations



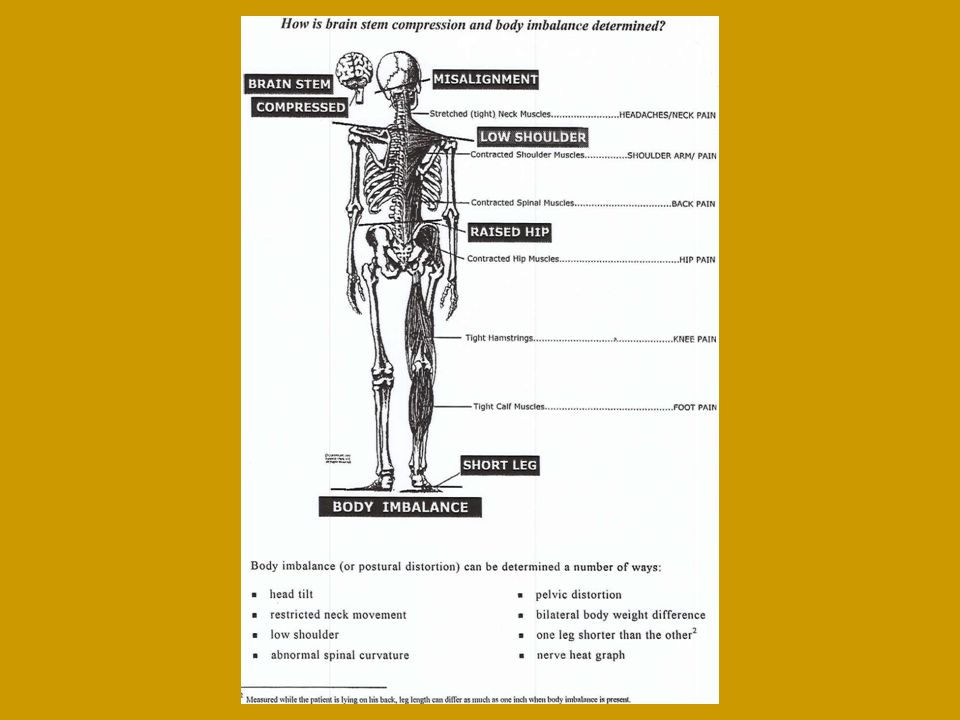
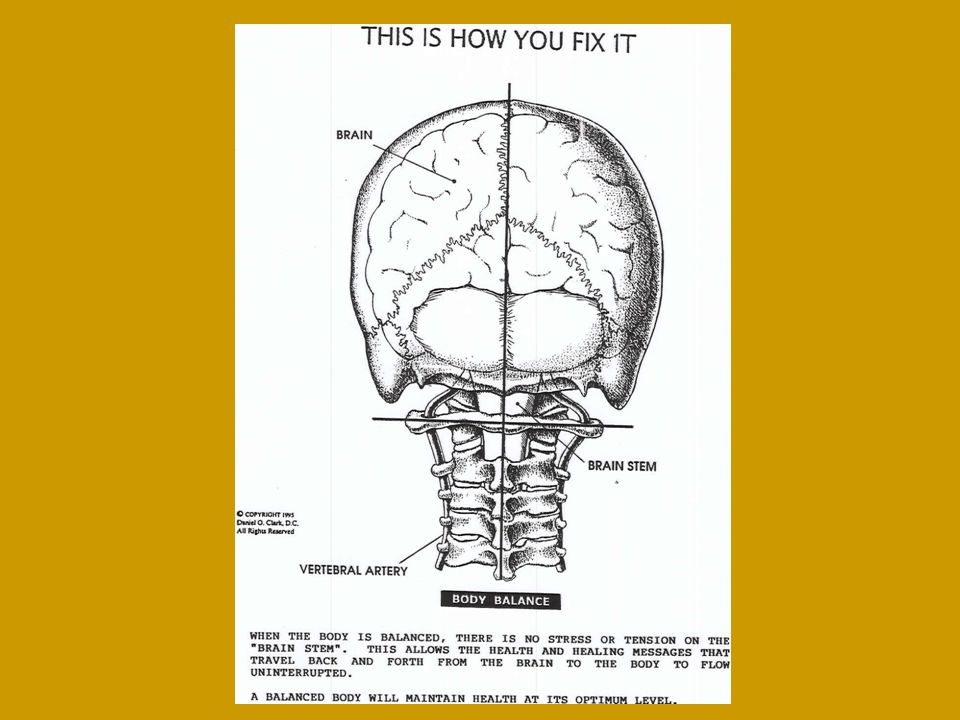




 and pulsating in nature, lasting from 4 to 72 hours; symptoms include.>")















