Download presentation
Presentation is loading. Please wait.

1
ADVANCE ANGIOPLASTY 2004 LONDON, Jan 15-16 2004 LATEST CLINICAL EVIDENCE WITH DEXAMET GERMANO DI SCIASCIO, MD, FACC, FESC Professor and Chairman of Cardiology, Campus Bio-Medico University of Rome

2
Dexamet TM is the BiodivYsio PC coated stents preloaded with Dexamethasone BiodivYsio Interdependent cell design Non-inflammatory PC coating Non-thrombogenic PC coating Long term implant history 1 m Stent Strut } Targeted drug delivery direct to arterial wall 0.5 µg/mm 2 Dexamethasone PC coating Arterial Side Lumen Side Stent strut cross-section

3
is a potent anti-inflammatory agent that treats the first step of the neointima formation/restenosis process has also anti-proliferative action by affecting the inflammation process is non-cytotoxic and does not destroy healthy cells and does not reduce or slow down the re- endothelisation Dexamethasone 1 S.H.Park and A.M.Lincoff, Semin. Interv. Cardiol., 1998, 3, 191-195

4
is delivered (when it’s most needed) early to target the inflammatory cells has strong clinical experience in humans demonstrated clinical benefits preferably in unstable in STRIDE and SAFE Dexamethasone (II) 1 S.H.Park and A.M.Lincoff, Semin. Interv. Cardiol., 1998, 3, 191- 195

5
- A pilot Phase II trial, multi-centre, prospective, non- randomised study. Dexamethasone dose 0.5 ug/mm 2 - 71 patients in 8 centres in Belgium - PI: Ivan De Scheerder - Endpoints: - 30-day and 6-month MACE - In-stent restenosis 6 months - Clinical and QCA :Late loss, loss index, MLD Dexamet’s first clinical trial :STRIDE Study of anti-restenosis with BiodivYsio Dexamethasone-Eluting stent

6
STRIDE STudy of Anti-Restenosis with BIodivYsio Dexamethasone-Eluting Stent 71 patients with 6-month angiographic follow-up Stent: BiodivYsio stent (dexamethasone 45 μg) % in-stent stenosis Unstable anginaStable angina p=0.017 MACE at 30 days = 1% (TLR =1%) MACE at 6 months = 3% (TLR=3%) MACE at 12 months: 3% (TLR=3%)
 % in-stent stenosis Unstable anginaStable angina p=0.017 MACE at 30 days = 1% (TLR =1%) MACE at 6 months = 3% (TLR=3%) MACE at 12 months: 3% (TLR=3%)")
7
BiodivYsio Trials Late Loss Comparisons PC coated stents without Dexamethasone

8
- A multi-centre registry with Dexamet TM & Dexamet SV - PI: Dr Pieter Stella, Utrecht, Netherlands - 1000 “Real-world” patients with no specific inclusion/exclusion criteria - patients must meet the indications specified in the Directions For Use - 66 centres over 16 countries in Europe, Middle-East, Africa and Asia-Pacific - Endpoints are in-hospital, 30-day and 6-month MACE - Results available at JIM 2004 First registry of Dexamet TM : SAFE

9
DEXAMETHASONE-ELUTING STENTS IMPROVE SIGNS OF INFLAMMATION IN PATIENTS WITH UNSTABLE CORONARY SYNDROMES UNDERGOING PERCUTANEOUS CORONARY INTERVENTION G. Patti, A. D’Ambrosio, A. Carcagni’, M. Cortes-Morichetti, P. Carminati, G. Di Sciascio CAMPUS BIOMEDICO UNIVERSITY OF ROME

10
Study design: case-control study with prospective evaluation Population: 60 pts receiving dexamethasone-eluting stent (Dexamet, N=30) or Biodivysio phosphorylcholine-coated stent (N=30) Inclusion criteria: - unstable angina (IIB-IIIB) or angina post recent (< 1 mo) myocardial infarction - angiographic evidence of “complex” coronary lesions that could be covered by a single stent Plasma levels of CRP were measured at: - 3 to 6 hours before PCI - 6, 24, 48 hours and 7 days after PCI Follow-up assessment: occurrence of MACE (myocardial infarction, death, repeat revascularization) DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES Methods
 or Biodivysio phosphorylcholine-coated stent (N=30) Inclusion criteria: - unstable angina (IIB-IIIB) or angina post recent (< 1 mo) myocardial infarction - angiographic evidence of complex coronary lesions that could be covered by a single stent Plasma levels of CRP were measured at: - 3 to 6 hours before PCI - 6, 24, 48 hours and 7 days after PCI Follow-up assessment: occurrence of MACE (myocardial infarction, death, repeat revascularization) DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES Methods")
17
3.7 ** 5.4 * 3.6 5.2 2.8 2.3 3.2 5.8 9.8 11.4 0 3 6 9 12 15 18 Pre6 h post24 h post48 h post7 days post CRP mg/l Dexamet TM Non DES * P=0.041 vs non DES ** P=0.026 vs non DES DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES

18
0 50 100 150 200 250 300 350 400 24 h48 h7 days Non DES Dexamet TM 152 85 396 93 326 32 P=0.03 P=0.01 CRP % increase from baseline DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES

19
Baseline CRP <3 mg/l (N=19) Baseline CRP 3 mg/l (N=11) 0 40 80 120 160 200 24 h48 h7 days CRP percent increase from baseline P=0.009 121 69 199 40 96 14 DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES
 Baseline CRP 3 mg/l (N=11) h48 h7 days CRP percent increase from baseline P= DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES")
20
0 20 40 60 80 100 01234 % of patients Dexamet Non DES months after stenting 6 P=0.06 Event-free survival curves DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES

21
CONCLUSIONS Dexamethasone-eluting stents improve early inflammatory response after PCI; this effect is more evident in pts with higher baseline CRP status The sustained attenuation of CRP values at 7 days may suggest early plaque stabilization with dexamethasone-eluting stents in pts with unstable coronary syndromes Clinical follow-up at 6 months shows a trend towards favorable intermediate-term results Will steroid-eluting stents be the treatment of choice for pts with unstable coronary syndromes?

22
MACE during the follow-up (%) 1 2 3 4 Pre-procedural CRP Quartiles 0 5 10 15 20 25 30 16% P = 0.09 5 27 RESULTS Patti, Di Sciascio et al. – Am J Cardiol

23
From morphology................ To plaque “biology”

25
CRP (mg/dl) 0 0,40 0,80 1,20 Controls N=12 Stable angina N=49 Unstable angina N=57 P=0.046 P=0.66 P=0.07 Distribution of CRP plasma levels Patti, Di Sciascio et al. – IL-1Ra: a sensitive marker of instability in patients with coronary artery disease J Thromb Thrombol 2002; 14: 139

26
MACE during the follow-up (%) 1 2 3 4 Pre-procedural IL-1Ra Quartiles P = 0.008 33 0 Patti, Di Sciascio et al. Prognostic value of IL-1Ra in patients undergoing percutaneous coronary intervention– Am J Cardiol 2002; 89: 372

29
SMC Proliferation Migration Matrix secretion SMC receptors Arterial injury Growth Factors & cytokines ThrombusInflammation G0G0 G1G1 G2G2 S M Smooth muscle cell (SMC) Signal transduction Cell cycle Dual mechanism of action of: PC coating and Dexamethasone cell cycle Smooth muscle cell Growth Factors & cytokines Arterial Injury - Neutrophils - Monocytes - Macrophage - Lymphocytes Reduces SMC Proliferation Matrix secretion Migration Reduced Receptor activation PC reduces thrombus formation Dexamethasone reduces Inflammation: Signal transduction
 Signal transduction Cell cycle Dual mechanism of action of: PC coating and Dexamethasone cell cycle Smooth muscle cell Growth Factors & cytokines Arterial Injury - Neutrophils - Monocytes - Macrophage - Lymphocytes Reduces SMC Proliferation Matrix secretion Migration Reduced Receptor activation PC reduces thrombus formation Dexamethasone reduces Inflammation: Signal transduction")
30
THERMOGRAPHY in ACUTE CORONARY SYNDROMES Temperature of the plaque is inversely correlated to cap thickness (Casscells W, Lancet 1996) Pts presenting with AMI and unstable angina have significantly more temperature heterogeneity in their coronary atherosclerotic plaques than pts with stable angina (Stefanadis C, Circulation 1999). Temperature was found to be the most powerful predictor of outcome (Stefanadis C, Circulation 2000) and to have a significant correlation with CRP levels (Stefanadis C, J Mol Cell Cardiol 2000)
 and to have a significant correlation with CRP levels (Stefanadis C, J Mol Cell Cardiol 2000).")
31
Inflamed plaque

32
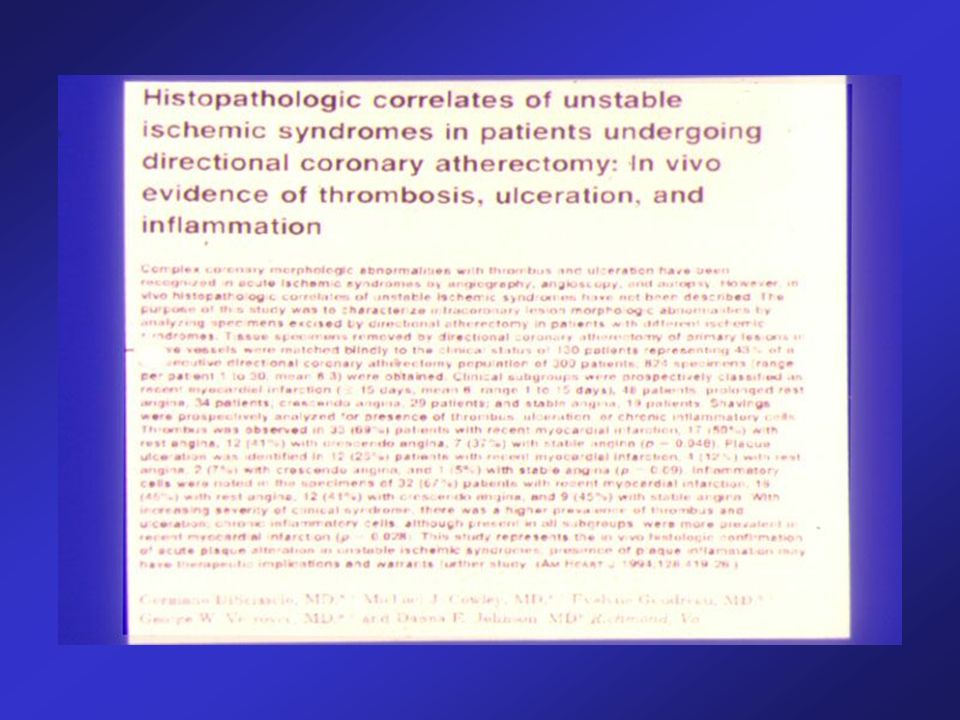
Di Sciascio et al. – Am Heart J 1994; 128: 419-26 Di Sciascio, Patti – Cardiologia 1999; 44: 333-9 300 pts, 824 specimens

33
0.002°C sensitivity

35
% Recurrent ischemia In-hosp. MACE UA and CRP <0.3 mg/dl UA and CRP >0.3 mg/dl Liuzzo, Maseri et al. The prognostic value of CRP and serum amyloid A protein in severe unstable angina. N Engl J Med 1994; 331: 417

36
IL1-Ra (pg/ml) Controls N=12 Stable angina N=49 Unstable angina N=47 0 100 200 300 400 500 P=0.038 P=0.002 P=0.99 IL-1Ra in ischemic syndromes Patti, Di Sciascio et al. – IL-1Ra: a sensitive marker of instability in patients with coronary artery disease J Thromb Thrombol 2002; 14: 139

37
0 20 40 60 80 100 0361218 months IL-1Ra (1st quart.) IL-1Ra (4th quart.) MACE-free survival % Patti, Di Sciascio et al. Prognostic value of IL-1Ra in patients undergoing percutaneous coronary intervention– Am J Cardiol 2002; 89: 372

38
Drug Eluting Stent Trials (stable AP)(unstable AP)(Non-drug) Late Loss (mm)
(unstable AP)(Non-drug) Late Loss (mm)")
39
Pepine CJ et al. A controlled trial of corticosteroids to prevent restenosis after coronary angioplasty. M-HEART Group – Circulation 1990; 81: 1753 - 915 patients undergoing PTCA randomized to placebo or 1 g methylprednisolone before the procedure - PTCA success rate 87% Placebo Steroids % Restenosis

40
Versaci et al. Immunosuppressive therapy for the prevention of restenosis after coronary Artery stent implantation (IMPRESS study) – JACC 2002; 40: 1935 Oral prednisone therapy for 45 days in pts with elevated (>0.5 mg/dl) CRP levels 72 hours post PCI
 – JACC 2002; 40: 1935 Oral prednisone therapy for 45 days in pts with elevated (>0.5 mg/dl) CRP levels 72 hours post PCI.")
Similar presentations









 study with the Sirolimus coated BX™ VElocity balloon expandable stent (CYPHER™)>")






 and of restenoses after stent deployment (ISR) still show.>")

 trial Prospective, multicenter, randomized, double blind trial investigating.>")
