Download presentation
Presentation is loading. Please wait.

2
VI Fracture Recognition and Classification

4
Radiologic Interpretation of Fractures Physical Therapy Considerations Prescribing appropriate modalities based upon: Recognition and classification of fractures Determining fx stability. Recognizing normal osseous healing vs. delayed or nonunion of bone Understanding the biomechanical function of internal fixation hardware. Identifying proper placement of internal fixation hardware

5
1. Fractures tend to follow sharp geometric lines rather than smooth, rounded or curved lines. 2. Fractures are normally congruent at the fracture lines: the two, or more, pieces fit one another. 3. Fractures will show bone resorption at the apposed surfaces within 1 week. 4. Fracture lines do not extend beyond the cortex of the bone. If it does think superimposition. 5. Stress or March fractures are often radiographically invisible for 7-10 days post injury.

6
Early fractures.

7
Avulsion Fracture of Distal Phalanx This fracture demonstrates congruence of the fragments

8
CT scan. Note both sharp geometric lines and congruence.

9
Fracture Base of 1 st Metacarpal 1.The sesamoid bone is an example of a commonly identified fracture/fragment. But note it is round and non congruent. If we had a follow-up film no resorption would be noted, a tip- off to the dx. 2.The fragments are sharp, congruent and no resorption is seen indicating a new, less than one week, fracture. Resorption becomes visible within a week or two. 3.Possible foolers: note the overlap of the dorsal and palmar joint surfaces giving the appearance of a fracture.

10
Reabsorption at the proximal tibial fracture.

11
Here is a common misinterpretation of a fracture where none exists.

12
Intra-operative image. Again note the characteristics of a fracture.

13
Fracture?

14
Stress Fractures do not become visible for about 10 days. This fx is about 2 weeks post. The appearance of callus is the diagnostic sign. Note the fuzzy, cotton- like appearance of bone callus formation.

15
1 day post jumping out of a tree. CC: pain in foot. Your diagnosis?

16
Tibial Stress Fracture: No bone callus seen because there has been no motion. But increased density is visible.

17
Diagnosis? What is your next step if you are not sure?

18
Technetium Bone Scan of same patient seen in previous film. Now what is your dx? Stress Fracture Left tibia

19
Fracture Age? Stability? PT implications?

20
Fracture Classification Scheme 1.Open or closed? 2.Incomplete? 1.Bowing, torus, greenstick 3.Complete? 1.Simple or comminuted 4.Transverse, Oblique, Spiral or Longitudinal 5.Medial, lateral, anterior or posterior displacement (of the distal fragment)? 6.Distraction? 7.If no fracture line is visible 1.Impaction or depression
. 6.Distraction. 7.If no fracture line is visible 1.Impaction or depression.")
21
Closed oblique fx of the third metatarsal, midshaft, non-displaced.

22
Compression Fracture of T12 Note the lateral view: does a great job with vertebral body fractures.

23
Open Spiral Fracture of midshaft tibia with posterior displacement.

24
Eponyms Many fractures have two names, a descriptive name and a Proper Noun name. The next slides demonstrate some of the more common eponyms that you should become familiar with and be able to identify and describe. There are many more; we have noted only some of the more common.

25
Common Fracture Eponyms Boxer’s: 4 th or 5 th metacarpal Colle’s Fracture: distal radius (wrist) often with ulnar styloid fx Galeazzi: distal radial fx with dislocation at distal radioulnar joint Segond: avulsion at lateral margin of the lateral tibial plateau Hill-Sachs fracture: impaction of the posterolateral humeral head Bankart: impaction of the anteroinferior glenoid H-S and Bankart associated with anterior dislocations Jones: proximal 5 th metatarsal Chauffeur’s: distal radial styloid, eversion mechanism.
 often with ulnar styloid fx Galeazzi: distal radial fx with dislocation at distal radioulnar joint Segond: avulsion at lateral margin of the lateral tibial plateau Hill-Sachs fracture: impaction of the posterolateral humeral head Bankart: impaction of the anteroinferior glenoid H-S and Bankart associated with anterior dislocations Jones: proximal 5 th metatarsal Chauffeur’s: distal radial styloid, eversion mechanism.")
26
More Fracture Eponyms Monteggia: proximal ulnar shaft associated with radial head dislocation Lisfranc: avulsion at medial base of 2 nd met often with lateral displacement of 2-5 metatarsals Bennet: base of 1 st metacarpal Jefferson: 1 st C vertebrae secondary to axial loading injury like diving Hangman’s: pedicles of C2 secondary to hyperextension Chance: upper lumbar vertebrae, usually L2, aka “seatbelt” injury secondary to hyperflexion of the lumbar spine over a fixed fulcrum Maissoneuve: medial malleolus and proximal fibular

27
Boxer’s Fracture

28
Colles Fracture aka: transverse fx of distal radius with dorsal tilt of distal fragment. A fall on the outstretched hand during a soccer match resulted in this injury.

29
Colles: the “dinner fork” appearance noted on the lateral view and clinically

30
Colles Loss of normal 10 degree volar tilt of distal radius

31
Galeazzi Fracture More proximal the Colle’s fx.

32
Segond FX

33
Hill-Sachs lesions Posterolateral aspect of humeral head

34
CT- axial view- of Hill- Sachs Lesion Anterior- Right shoulder Posterior

35
Bankart Fracture: anterior inferior glenoid Bankart lesion: detachment of anterior inferior portion of glenoid. Same mechanism of injury-anterior dislocation- with injury either to humerus and/or glenoid. Axial CT of Bankart Fx

36
Ant. Dislocation of humerus with Bankart Fx Note: CT’s, like MRI’s, are viewed as if looking at the patient in supine position, from the patient’s feet up to the head. This is a R shoulder with anterior at the top. A L

38
Pediatric Fractures Fractures involving Epiphyseal plates are usually described with the Salter-Harris Classification system. There are 5 major types of S-H fractures, with a 6 th through 9th sometimes used.

39
Classification of Epiphyseal Fractures I - pure epiphyseal separation if non-displaced, jt effusion may be only sign II- metaphyseal fracture + epiphyseal separation III -epiphyseal fracture IV- vertically oriented fx thru epiphysis + metaphysis V- crush injury of epiphysis (not detected acutely) Most common: type II type I (best) type V (worst)-may result in premature closure of epiphyseal plate.
 Most common: type II type I (best) type V (worst)-may result in premature closure of epiphyseal plate.")
40
Salter-Harris Classification Clinically the S-H classification would be used to describe a fracture, for example, “a Salter Harris 1 fracture is noted at the medial aspect of the distal tibia” etc. Refer to these fractures in conversation as “Salter Harris 2’s or 3’s” and so on.

42
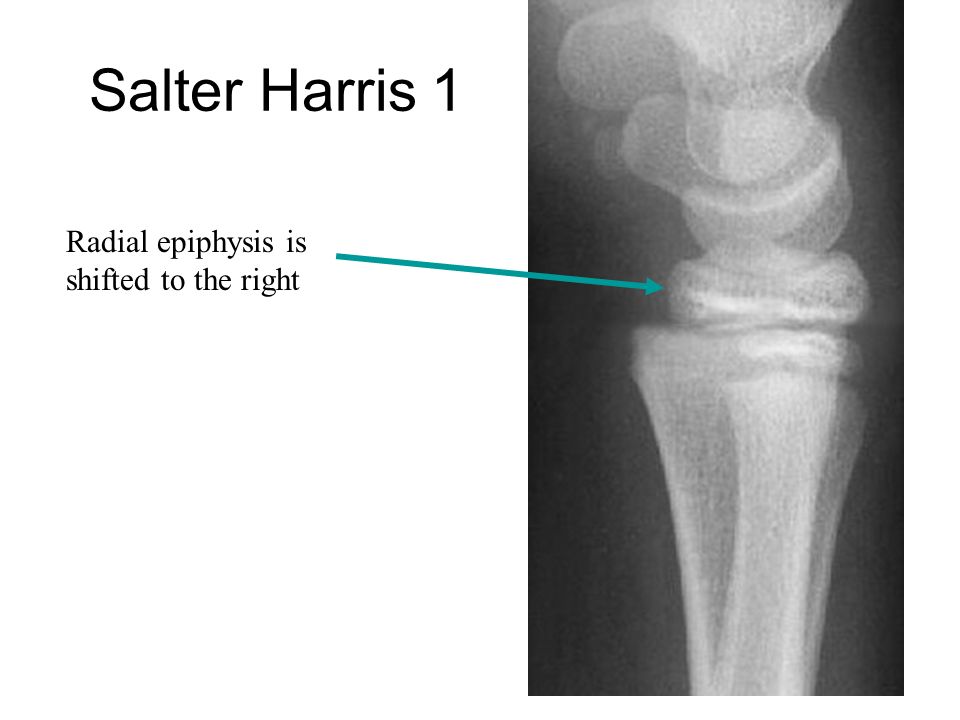
Salter Harris 1 Radial epiphysis is shifted to the right

43
Salter Harris 2

44
Salter Harris 3

45
Salter Harris 4

46
Salter Harris 5

Similar presentations