Download presentation
Presentation is loading. Please wait.

1
Choosing a reference group Louise Coole Sources: EPIET courses (from 1995 to 2011) J Stewart, A Moren
 J Stewart, A Moren")
2
Objectives Define source population Explore the meaning of representativeness Understand the importance of a reference group in analytical studies Describe advantages and disadvantages of selecting different types of controls

3
Compare –disease incidence in exposed and unexposed (cohort studies) –exposure in cases and controls –disease incidence in different time-periods in a population Epidemiologists.... compare Measure and compare

4
Comparison / Reference group Unexposed in cohort studies Controls in case control studies Focus on controls since selection of controls can be an important source of bias.

5
Cohort study: Purpose of the comparison group The comparison group serves to provide an estimate of the expected disease incidence in the exposed group if the exposure had been absent. Rothman KJ, 1986

6
Cohort study - Challenge To identify a population similar to the exposed population and only differing by the absence of exposure

7
Cohort - Well defined population Nursing home, school, wedding e.g. food borne outbreak Retrospectively identify have eaten % disease did not eat% disease

8
Does HIV infection increase risk of developing TB among a population of drug users? Population TB Cases HIV + 215 8 HIV - 289 1 Source: Selwyn et al., New York, 1989

9
Reference group in case control studies

10
Reference group in a case control study = control group The comparison group serves to provide an estimate of the exposure distribution in the source population from which the cases originate. Rothman KJ, 1986

11
Controls Controls should be representative of population from which cases arise (source population)
")
14
Rothman KJ, Oxfort Univ Press, 2002

15
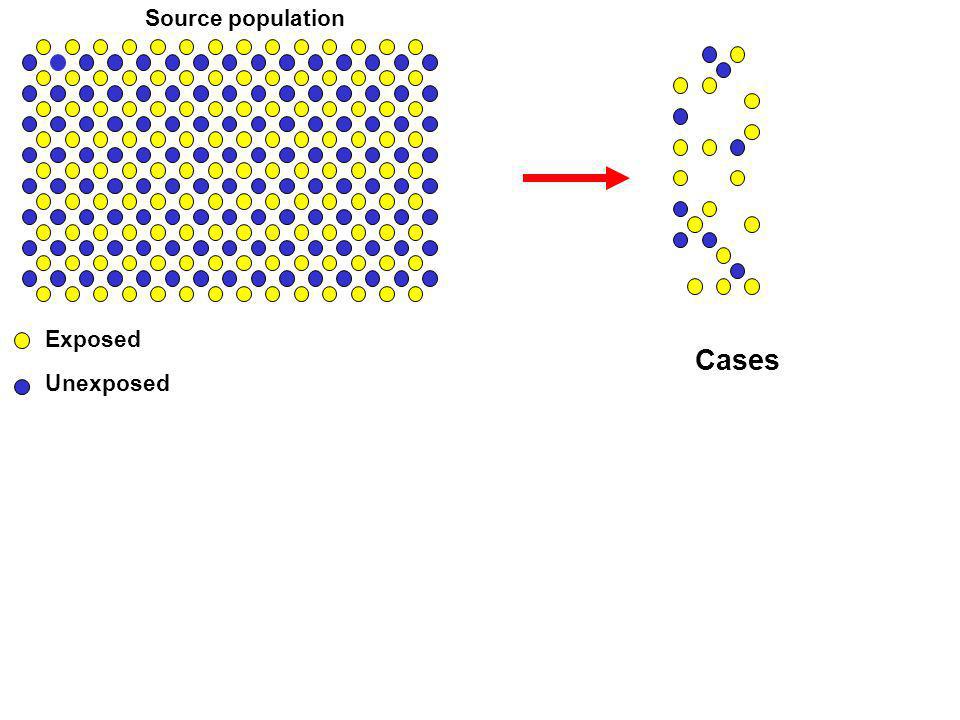
Cases Exposed Unexposed Source population Controls: Sample of the denominator Representative with regard to exposure Controls Sample Case control studies

16
Control characteristics If controls represent source population be representative of exposures in source population be identified as cases if they had disease under study have same exclusion and restriction criteria as cases

17
Case control study Outbreak 32 cases of Salmonella Enteritidis North Yorkshire(population 500,000) onset through April 2012 age range 15 – 48 years 19 male, 13 female no recent travel abroad
 onset through April 2012 age range 15 – 48 years 19 male, 13 female no recent travel abroad")
18
Who are the right controls?

19
Who is source population? Start with your case definition

20
Case definition Resident of North Yorkshire aged above 14 years with isolate of Salmonella Enteritidis in faecal sample during April 2012 Exclusion: Travel abroad in week before illness What is source population?

21
Source population Residents of North Yorkshire aged above 14 years during April 2012 who have not recently travelled abroad Controls should then be representative of this population

22
How to select controls? Aim for random sample of source population Not always feasible Case control studies

23
Selecting controls (examples) Population random from register/list/directory stratified (age/sex/general practice) Friends Neighbourhood Hospital
 Population random from register/list/directory stratified (age/sex/general practice) Friends Neighbourhood Hospital")
24
Population / community controls Is there a list or register of source population? Such a list should –be complete –contain all cases –be readily accessible –identify specified characteristics e.g. age Take random sample

25
or... random digit dialling using residential directories or mobile numbers (e.g. add 5 to case number) quick and easy but may be biased in selection –telephone ownership –availability –geographical area –participation
 quick and easy but may be biased in selection –telephone ownership –availability –geographical area –participation.")
26
Friends / family controls Advantages Good matching for social and genetic factors Can be quick and easy Disadvantages Effectively link the cases and controls May not be able to detect a diference in exposure of importance Co-operation may be limited

27
Neighbourhood controls Advantages –no need for population register –similar socio-economic status and environmental exposure Disadvantages –might be too similar to cases –low co-operation –may be time consuming, expensive

28
Hospital controls Advantages –useful if all cases identified from hospital register –easily identified –cost and time efficient Disadvantages –different catchments for different diseases –May not be representative of source population –overmatching on exposures for other diseases Tobacco / lung cancer and controls with CVD

29
Controls may not be easy to find

30
Case control study Outbreak 32 cases of Salmonella Enteritidis North Yorkshire(population 500,000) onset through April 2012 age range 15 – 48 years 19 male, 13 female no recent travel abroad
 onset through April 2012 age range 15 – 48 years 19 male, 13 female no recent travel abroad")
31
Source population Residents of North Yorkshire aged above 14 years during April 2012 who have not recently travelled abroad Controls should then be representative of this population

32
Which reference group ? You are in charge of the case control study! How would you select controls ? No population register or list is available Please discuss with a person next to you (2 minutes!)
.")
33
Some common questions Immune populations 100% exposure 100% ill Non-cases as controls

34
Immune subjects Not eligible as cases –so not in source population Difficult to identify May have been cases in the past May have similar level of exposure to risk factor as current cases in study May introduce bias and under-estimation of effect.

35
What if 100% exposure ? What if close to 100% of population exposed? e.g. foodborne disease outbreaks where little choice in menu Try to measure dose response Reference group lowest level of exposure

36
Which control group if 100% ill ? What if close to 100% of population ill? Try to have severity –Cases: severe cases –Control group: less severe cases

37
Outbreak of S. enteritidis in a Kebab restaurant, North East London February 2005 Food specific attack rates of severe case (AR), relatives risks (RR), 95% confidence intervals (95%) amongst cases. Food eatenFood not eaten SevereTotalAR% Severe TotalAR%RR95% CI Salad 101283.3327145.1 1.9 1.3-2.7 Chips 111478.5316944.9 1.8 1.2-2.6 Sauce 315952.5112445.8 1.2 0.7-1.9 Salad 315754.4112642.3 1.3 0.8-2.1 Giraudon I et al, EPIET, London HPA
, relatives risks (RR), 95% confidence intervals (95%) amongst cases. Food eatenFood not eaten SevereTotalAR% Severe TotalAR%RR95% CI Salad Chips Sauce Salad Giraudon I et al, EPIET, London HPA.")
38
Controls are non cases Low attack rate: non-cases likely to represent exposure in source pop Non- cases Source popn High attack rate: non-cases unlikely to represent exposure in source population Cases Non- cases endstart endstart

39
Non- cases as controls If attack rate high –non-cases unlikely to represent exposure in source population If attack rate low –non-cases likely to represent exposures in source population –can use as controls

40
Cases E E 4 Source Population 60 40 36 ARe = 60% ARue = 10% RR = 6 24 36 Non cases Cohort Outbreak of food borne disease in a nursing home. 100 residents, 40 cases

41
Cases E E 4 Source Population 60 40 Outbreak of food borne disease in a nursing Home. 100 residents, 40 cases 36 RR = 6 24 36 Non cases Cohort Sample Non cases 1212 18 OR = 13.5 Potential control groups

42
Cases Sample Non cases E E 1212 4 18 Source Population 60 40 Outbreak of food borne disease in a nursing home. 100 residents, 40 cases 36 Sample Source Population 30 20 RR = 6OR = 13.5 OR = 6 24 36 Non cases Potential control groupsCohort

43
A member of the source population is a suitable control

44
What if: Only non-cases as controls? If attack rate is low non-cases likely to represent exposures in source population can use them as controls If attack rate is high, non-cases unlikely to represent exposure in source population OR may be over-estimated More accurate not to exclude cases from control group Concept of case-cohort studies!

45
Case-cohort design Control group estimates the proportion of the total population that is exposed Controls selected from all individuals at risk at the start of the study –sampled regardless whether or not they will fall ill Case may also be selected as a control and vice versa -> kept in both groups No need to document disease status among controls OR estimates relative risk

46
Key points in choosing controls Define source population –Think of the cohort you could have done Aim for representative sample Review pros and cons of available options

47
Characteristics of good controls Come from the same population as the cases May be exposed like cases Can develop the disease Could be recruited as cases if diseased Have exposure window identical to cases Are adapted to study objectives

48
Dealing with imperfect control groups Examine the limitations of your control group with respect to each criteria Assess in which way the limitation will affect the odds ratio Interpret your results in light of this review

49
Conclusions No control group is perfect Consider the advantages and disadvantages of the available options Aim to minimise error within constraints of resources and urgency of study

50
Be prepared to defend your choice…

51
References Rothmann KJ, Greenland S. Modern epidemiology. Lippincott- Raven 1998. Hennekens CH, Epidemiology in Medicine. Lippincott-Williams and Wilkins 1987.

Similar presentations







 Chris Williams (adapted from EPIET slides)>")












