Download presentation
Presentation is loading. Please wait.

1
The Basics of Safely Prescribing SSRIs/SNRIs & Other Medications for Depression and Anxiety Symptoms with Job Corps Students David Kraft, MD, MPH Boston Regional Mental Health Specialist

2
Outline Overview of psychotropic drugs Diagnostic categories (DSM-5) Clinical indications (e.g., starter doses, follow-up doses, etc.) Black box warnings Side effects Indications and strategies to stop medications Ongoing frequency of follow-up Drug interactions
 Clinical indications (e.g., starter doses, follow-up doses, etc.) Black box warnings Side effects Indications and strategies to stop medications Ongoing frequency of follow-up Drug interactions")
3
Overview Most frequent mental health problems in Job Corps where medications are prescribed are depression and anxiety issues. The next most common problem is ADHD at many centers. Most frequent psychoactive medications with Job Corps youth are antidepressants, which are also good for anxiety issues.

4
Overview (continued) Fewer students will require other psychotropic medications, such as are used with Bipolar Disorder, Schizophrenia, and other disorders –Usually such students will arrive already on these medications, so the Center Physician may only be asked to continue the prescriptions –Many Job Corps centers are not located near a psychiatric clinic or provider who can prescribe for the student while on center
 Fewer students will require other psychotropic medications, such as are used with Bipolar Disorder, Schizophrenia, and other disorders –Usually such students will arrive already on these medications, so the Center Physician may only be asked to continue the prescriptions –Many Job Corps centers are not located near a psychiatric clinic or provider who can prescribe for the student while on center")
5
Diagnostic Symptoms of Depression (DSM-5) Criteria for Depression (5 of 9 symptoms) –Depressed mood nearly every day –Decreased interest/pleasure in activities –Significant change in weight (not trying +/-) –Insomnia or hypersomnia most days –Psychomotor agitation or retardation –Fatigue/loss of energy most every day –Feelings worthlessness/excessive guilt –Reduced ability to think or concentrate –Recurrent thoughts of death/suicidality
 Criteria for Depression (5 of 9 symptoms) –Depressed mood nearly every day –Decreased interest/pleasure in activities –Significant change in weight (not trying +/-) –Insomnia or hypersomnia most days –Psychomotor agitation or retardation –Fatigue/loss of energy most every day –Feelings worthlessness/excessive guilt –Reduced ability to think or concentrate –Recurrent thoughts of death/suicidality")
6
Depression Symptoms (continued) Symptoms cause clinically significant distress or impairment Episodes not due to physiological effects of a substance or another medical condition Other Depressive Diagnoses –Persistent Depressive Disorder (Dysthymia) –Premenstrual Dysphoric Disorder –Substance/Medication Induced Depression
 Symptoms cause clinically significant distress or impairment Episodes not due to physiological effects of a substance or another medical condition Other Depressive Diagnoses –Persistent Depressive Disorder (Dysthymia) –Premenstrual Dysphoric Disorder –Substance/Medication Induced Depression")
7
Diagnostic Symptoms of General Anxiety Disorders Worry about specific situation for at least 6 months, plus 3/6 symptoms: –Restlessness, all keyed up –Being easily fatigued –Trouble concentrating or mind goes blank –Irritability –Muscle tension –Sleep disturbance Treat with Psychotherapy plus Meds –Cognitive Behavioral Therapy, Relaxation, Rebreathing, Meditation

8
Diagnostic Symptoms of Other Anxiety Disorders Specific Phobia and Social Phobia Panic Disorder Agoraphobia (marked fear/anxiety about not being able to avoid dangers) Obsessive Compulsive Disorder and Related Disorders Post-Traumatic & Acute Stress Disorder Eating Disorders
 Obsessive Compulsive Disorder and Related Disorders Post-Traumatic & Acute Stress Disorder Eating Disorders")
9
General Principles Most medications take 1-2 weeks to work effectively (absorbed in GI tract, then transferred to cerebrospinal fluid in brain to begin working) Side-effects often noticed shortly after taking medication (mainly in blood in sufficient levels) Some side-effects can be useful, e.g. sedation if someone has trouble getting to sleep Most antidepressants are good for treating anxiety disorders as well

10
General Principles in Job Corps Most students on medications when they arrive will want to stay on the medication during their training. Consult with the Center Mental Health Consultant (CMHC) when a student seems to need an adjustment in one of his/her medications. Major changes in medication should be done during vacations, if possible.
 when a student seems to need an adjustment in one of his/her medications. Major changes in medication should be done during vacations, if possible..")
11
Clinical Indications Major Depression (single and recurrent types, not Bipolar) Severe Anxiety Disorders, e.g. Obsessive Compulsive Disorder Sleep hygiene, not complicated, though may need to add sedating antidepressant (e.g. trazodone) and follow
 and follow.")
14
Dosing: SSRIs Medication (generic/trade) Starting doseUsual doseCategory citalopram (Celexa) 10 mg qd20-40 mg qdSSRI escitalopram (Lexapro) 10 mg qd10-20 mg qdSSRI fluoxetine (Prozac) 10 mg qam20-60 mg qdSSRI fluvoxamine (Luvox) 50 mg qd100-300 mg qdSSRI paroxetine (Paxil) 10 mg qhs20-60 mg qdSSRI sertraline (Zoloft) 25 mg qd50-200 mg qdSSRI trazodone (Desyrel) 25 mg qhs25-150 mg qhsSSRI
 Starting doseUsual doseCategory citalopram (Celexa) 10 mg qd20-40 mg qdSSRI escitalopram (Lexapro) 10 mg qd10-20 mg qdSSRI fluoxetine (Prozac) 10 mg qam20-60 mg qdSSRI fluvoxamine (Luvox) 50 mg qd mg qdSSRI paroxetine (Paxil) 10 mg qhs20-60 mg qdSSRI sertraline (Zoloft) 25 mg qd mg qdSSRI trazodone (Desyrel) 25 mg qhs mg qhsSSRI")
15
Half-Life, Features, and Side Effects (SSRIs) Generic (Brand)Half-LifeFeaturesSide- effects fluoxetine (Prozac) 60 hrsStimulating, not sedating Used for OCD, depression, once a day dosing GI upset sertraline (Zoloft) 26 hrsIncreased plasma level with food Used for depression and anxiety, has a more linear dose/response relationship than other SSRIs Sexual side effects citalopram (Celexa) 35 hrsNot as good with high levels of anxiety Sedation may impede higher dosing
 Generic (Brand)Half-LifeFeaturesSide- effects fluoxetine (Prozac) 60 hrsStimulating, not sedating Used for OCD, depression, once a day dosing GI upset sertraline (Zoloft) 26 hrsIncreased plasma level with food Used for depression and anxiety, has a more linear dose/response relationship than other SSRIs Sexual side effects citalopram (Celexa) 35 hrsNot as good with high levels of anxiety Sedation may impede higher dosing")
16
Half-Life, Features, and Side Effects (SSRIs) Generic (Brand)Half-LifeFeaturesSide-effects escitalopram (Lexapro) 35 hrs2x stronger by dose than citalopram Fewer side effects than citalopram fluvoxamine (Luvox) 15.6 hrsGiven in divided doses Known for being approved for Obsessive Compulsive Disorder, though not really better than other SSRIs Some weight gain paroxetine (Paxil) 26 hrsMore sedative side effects and weight gain
 Generic (Brand)Half-LifeFeaturesSide-effects escitalopram (Lexapro) 35 hrs2x stronger by dose than citalopram Fewer side effects than citalopram fluvoxamine (Luvox) 15.6 hrsGiven in divided doses Known for being approved for Obsessive Compulsive Disorder, though not really better than other SSRIs Some weight gain paroxetine (Paxil) 26 hrsMore sedative side effects and weight gain")
18
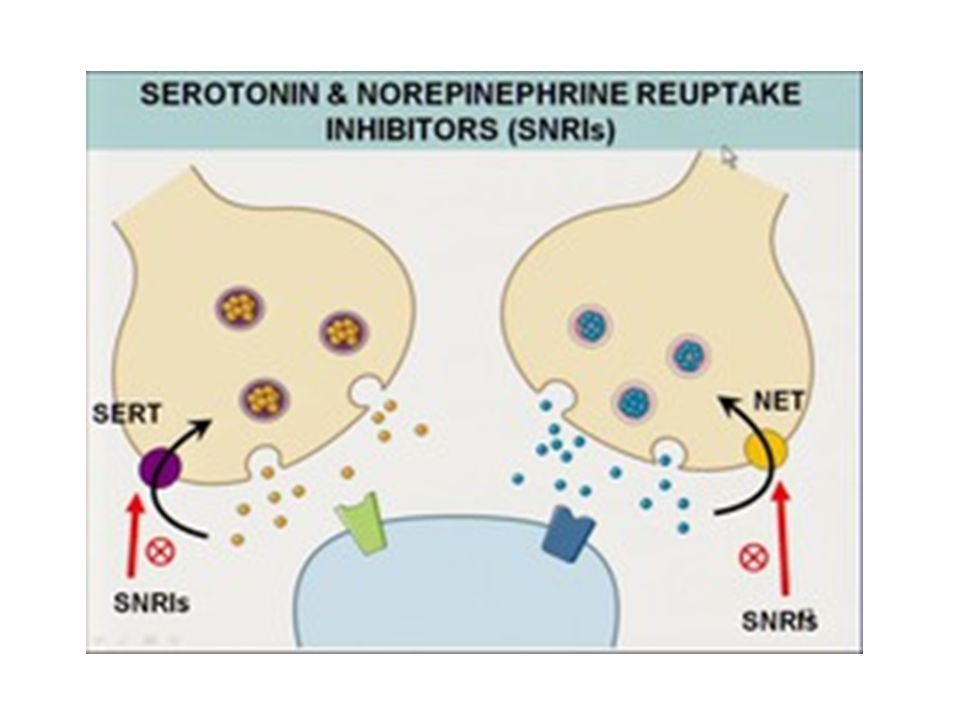
Dosing: SNRIs Medication (generic/trade) Starting doseUsual doseCategory venlafaxine (Effexor) 25 mg qd75-375 mg qdSNRI duloxetine (Cymbalta) 20 mg qd60-120 mg qdSNRI desvenlafaxine (Pristiq) 50 mg qd50-100 mg qdSNRI
 Starting doseUsual doseCategory venlafaxine (Effexor) 25 mg qd mg qdSNRI duloxetine (Cymbalta) 20 mg qd mg qdSNRI desvenlafaxine (Pristiq) 50 mg qd mg qdSNRI")
19
Half-Life, Features, and Side Effects (SNRIs/NDRI) Generic (Brand)Half-LifeFeaturesSide- effects desvenlafaxine (Pristiq) 9-11 hrsWell absorbed from GI tract Studies have shown that SNRI treatment of both outpatients with major depression and inpatients with melancholia have proven better than treatments with SSRIs and other agents Monitor BP duloxetine (Cymbalta) 12 hrsSuperior results with Generalized Anxiety Disorder (GAD) Studies of SNRIs with various anxiety disorders and pain conditions seems to be improving treatment options that used to be responsive to tricyclic antidepressants (TCAs), but with fewer side effects. Not tolerated as well as SSRIs venlafaxine (Effexor) 4-6 hrsSuperior results with chronic pain, with fewer side effects than TCAs Not tolerated as well as SSRIs bupropion (Wellbutrin) 9.8hrsnorepinephrine-dopamine reuptake inhibitor (NDRI), rapid absorption, metabolized by liver (use carefully if liver damage is evident), usual starter dose 100mg in AM; daily doses 100-450mg daily
 4-6 hrsSuperior results with chronic pain, with fewer side effects than TCAs Not tolerated as well as SSRIs bupropion (Wellbutrin) 9.8hrsnorepinephrine-dopamine reuptake inhibitor (NDRI), rapid absorption, metabolized by liver (use carefully if liver damage is evident), usual starter dose 100mg in AM; daily doses mg daily.")
20
Other Common Agents Older agents (e.g., tricyclic antidepressants & MAOIs) not used without consultation with Specialist
 not used without consultation with Specialist")
21
Black Box Warnings Increased risk of suicidal thinking and behavior in children, adolescents, and young adults taking antidepressants Monitor for worsening and emergence of suicidal thoughts and behaviors, especially during the first two weeks of treatment

22
Black Box Warnings Antidepressants increased the risk compared to placebo of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults in short-term studies of major depressive disorder (MDD) and other psychiatric disorders. –Risk limited to persons under 24 years –Worse in first 10-14 days of treatment in most studies –May take at least 1 month to work –Suicidality NOT the same as suicide

23
Indications to Stop Medications Unacceptable side effects after 5 days. (Usually, mild sedation or activation disappears in a few days). Occurrence of mania/hypomanic symptoms when not already on Mood Stabilizers (lithium, divalproex, carbamazepine). Staff or other students complain about risky behaviors, different from behavior before medication. Report of suicidal ideas or plans (probably needs MSWR or hospitalization if concern about suicide).
. Occurrence of mania/hypomanic symptoms when not already on Mood Stabilizers (lithium, divalproex, carbamazepine). Staff or other students complain about risky behaviors, different from behavior before medication. Report of suicidal ideas or plans (probably needs MSWR or hospitalization if concern about suicide)..")
24
Stopping Medications When someone stops their psychotropic medications, it usually takes at least 5 days to get out of their system. –Most meds need to be tapered, to avoid withdrawal symptoms. –Exceptions to these general rules include stimulants and “benzos” (benzodiazepines), which work quickly and can usually be stopped quickly, though tapering is better.
, which work quickly and can usually be stopped quickly, though tapering is better..")
25
Drug Interactions SSRIs/SNRIs are generally safe and effective after at least 2 weeks Starting dose often all that is needed A few students treated with TCAs will need added side effect meds.* Students on MAOIs need careful monitoring to avoid dietary side effects.* Most other medications can be safely taken with usual SSRI/SNRI treatment.. *Consultation indicated.

26
Ongoing Follow-up Students should be monitored by the center physician (CP), CMHC, and health and wellness staff. If current medicine is not working –CP may consult with CMHC and adjust meds –Refer for consult with psychiatrist in community, if available –Refer back to original prescriber via leave or during breaks –MSWR should be considered if student is having acute symptoms interfering with participation in program

27
References Black, DW, & Andreasen, NC. (2014). Introductory Textbook of Psychiatry (sixth edition). Arlington, VA: American Psychiatric Publishing, a Division of the American Psychiatric Association. Maxmen, JS, Kennedy, SH, & McIntyre, RS. (2008). Psychotropic Drugs: Fast Facts, Fourth Edition. New York: WW Norton & Company, Inc. Schatzberg, AF, & DeBattista, C. (2015). Manual of Clinical Psychopharmacology, Eighth Edition. Arlington, VA: American Psychiatric Publishing, a Division of the American Psychiatric Association.
. Arlington, VA: American Psychiatric Publishing, a Division of the American Psychiatric Association. Maxmen, JS, Kennedy, SH, & McIntyre, RS. (2008). Psychotropic Drugs: Fast Facts, Fourth Edition. New York: WW Norton & Company, Inc. Schatzberg, AF, & DeBattista, C. (2015). Manual of Clinical Psychopharmacology, Eighth Edition. Arlington, VA: American Psychiatric Publishing, a Division of the American Psychiatric Association..")
Similar presentations

 Psychosocial Interventions.>")

















