Download presentation
Presentation is loading. Please wait.

1
Budesonide/formoterol as effective as prednisolone plus formoterol in acute exacerbations of COPD A double-blind, randomised, non-inferiority, parallel-group, multicentre study Done by: Khalid Al-Rashdi R3 Khalid Al-Rashdi R3

2
Non-inferiority is a kind of similarity within a limit. The limit is the degree of tolerable inferiority of the new drug compared with the standard treatment. if the non-inferiority limit is set at 7 · 5%, an increase in the incidence of serious events or deaths — say 7% instead of the 5% currently established for the comparator — is not seen as large enough to mark a difference between the new and the control drug. The new drug will therefore be considered non-inferior to the old drug.

3
Introduction: - Chronic obstructive pulmonary disease (COPD) is a major health problem and cause of death and disability. - up to 90% of all COPD patients with exacerbations can be treated at primary health care centres and thereafter return home with intensified therapy. - oral corticosteroids represent standard treatment for COPD exacerbations.

4
- 2-week course of inhale budesonide/formoterol would be equally effective for treatment of acute COPD exacerbations as standard therapy in patients judged by the investigator not to require hospitalisation. - - the initial 2-week treatment would influence the rate of exacerbations during a subsequent 12-week open-label treatment period with the fixed combination of budesonide and formoterol at a standard dose of 320/9 μg bid.

5
- Department of Public Health and Caring Sciences, Family Medicine and Clinical Epidemiology, Uppsala University, Sweden. -done in one hospital and 29 health centers. Published: 19 February 2009 Respiratory Research 2009, 10:11 doi:10.1186/1465-9921- 10-11 This article is available from: http://respiratory- research.com/content/10/1/11

6
Methods: -double-blind, randomised, non-inferiority, parallel- group, multicentre study comparing two treatment strategies. -double-blind, randomised, non-inferiority, parallel- group, multicentre study comparing two treatment strategies. -two weeks' treatment with inhaled budesonide/formoterol (320/9 μg, qid) was compared with prednisolone (30 mg once daily) plus inhaled formoterol (9 μg bid) in patients with acute exacerbations of COPD attending a primary health care centres. -two weeks' treatment with inhaled budesonide/formoterol (320/9 μg, qid) was compared with prednisolone (30 mg once daily) plus inhaled formoterol (9 μg bid) in patients with acute exacerbations of COPD attending a primary health care centres.
 was compared with prednisolone (30 mg once daily) plus inhaled formoterol (9 μg bid) in patients with acute exacerbations of COPD attending a primary health care centres. -two weeks treatment with inhaled budesonide/formoterol (320/9 μg, qid) was compared with prednisolone (30 mg once daily) plus inhaled formoterol (9 μg bid) in patients with acute exacerbations of COPD attending a primary health care centres..")
7
Inclusion criteria: - ≥ 10 pack years,aged ≥ 40 years, with moderate COPD corresponding to GOLD stage IIa or IIb,COPD for ≥ 6 months prior to study entry. -dyspnoea for less than one week -FEV1 30 – 60% of predicted normal after acute treatment with a single dose of oral corticosteroid plus nebulised salbutamol/ipratropium bromide -no requirement for subsequent immediate hospitalisation. -subsequent open-label budesonide/formoterol (320/9 μg bid) for another 12 week. -subsequent open-label budesonide/formoterol (320/9 μg bid) for another 12 week.
 for another 12 week. -subsequent open-label budesonide/formoterol (320/9 μg bid) for another 12 week..")
8
Exclusion criteria: - diagnosis of asthma. - a previous COPD exacerbation within 30 days prior to the study. - oxygen saturation < 92% after the initial acute treatment. - Requirement for oxygen therapy. - a need for immediate hospitalisation as judged by the investigator. - treatment with any inhaled corticosteroid in doses > 1000 μg/day at study entry. - use of or need for treatment with a non-selective β- receptor.

9
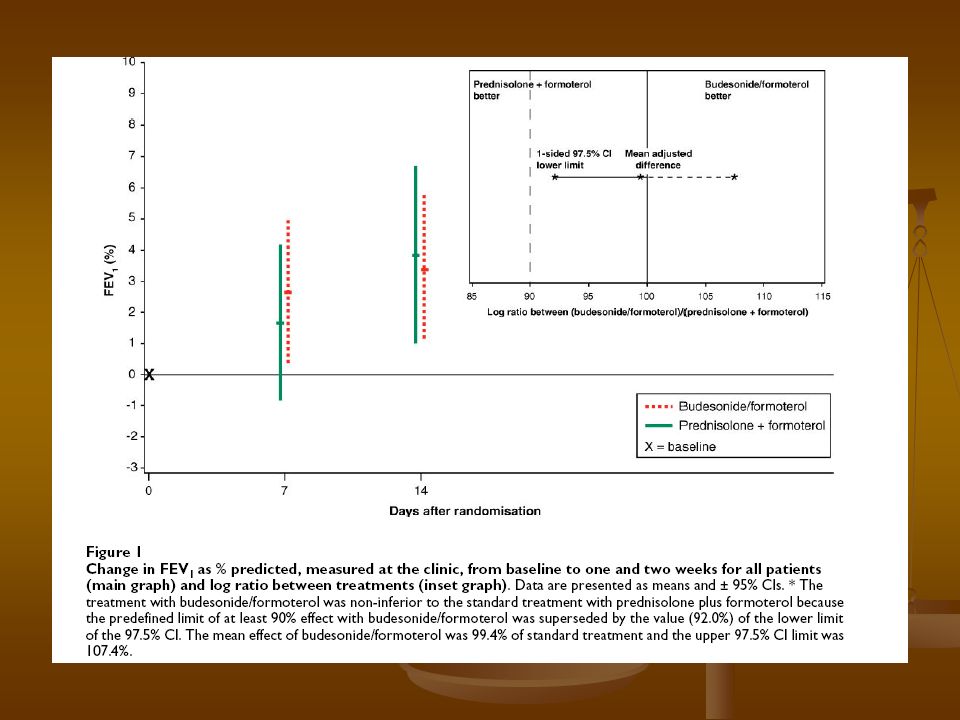
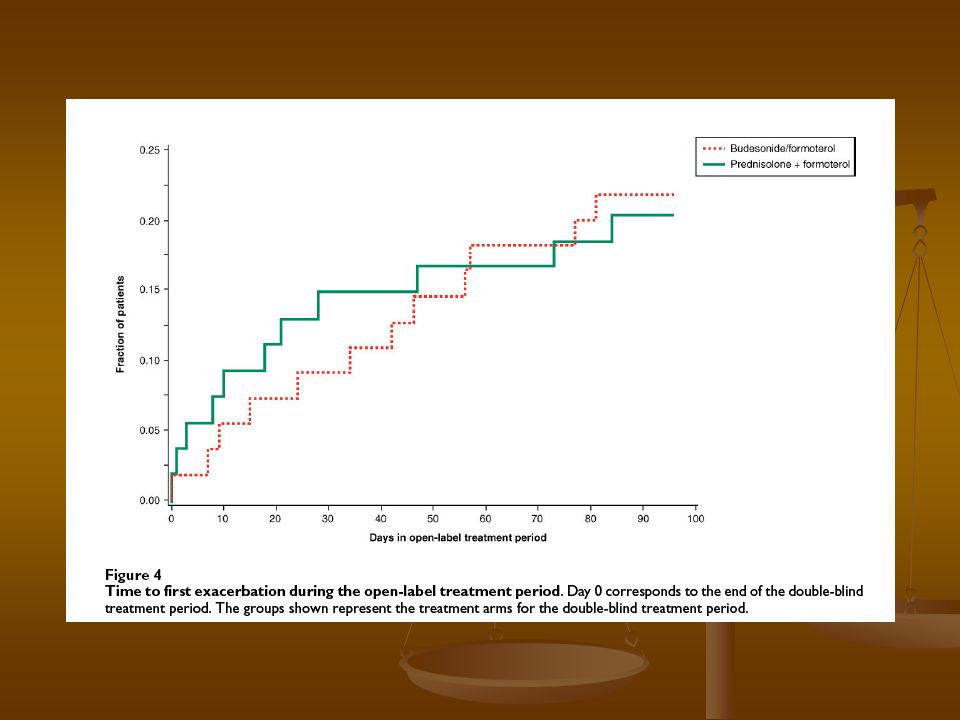
Assessments: - end of weeks one and two, and at the end of the - end of weeks one and two, and at the end of the open follow-up period. open follow-up period. - The primary efficacy variable → change in FEV1 from baseline to treatment. - The primary efficacy variable → change in FEV1 from baseline to treatment. - Other efficacy variables were treatment failures,FEV1 measured twice daily at home with a Piko-1 ® electronic peak flow meter, the number of patients with an - Other efficacy variables were treatment failures,FEV1 measured twice daily at home with a Piko-1 ® electronic peak flow meter, the number of patients with an exacerbation and the time to first exacerbation during the follow-up period. exacerbation and the time to first exacerbation during the follow-up period.

10
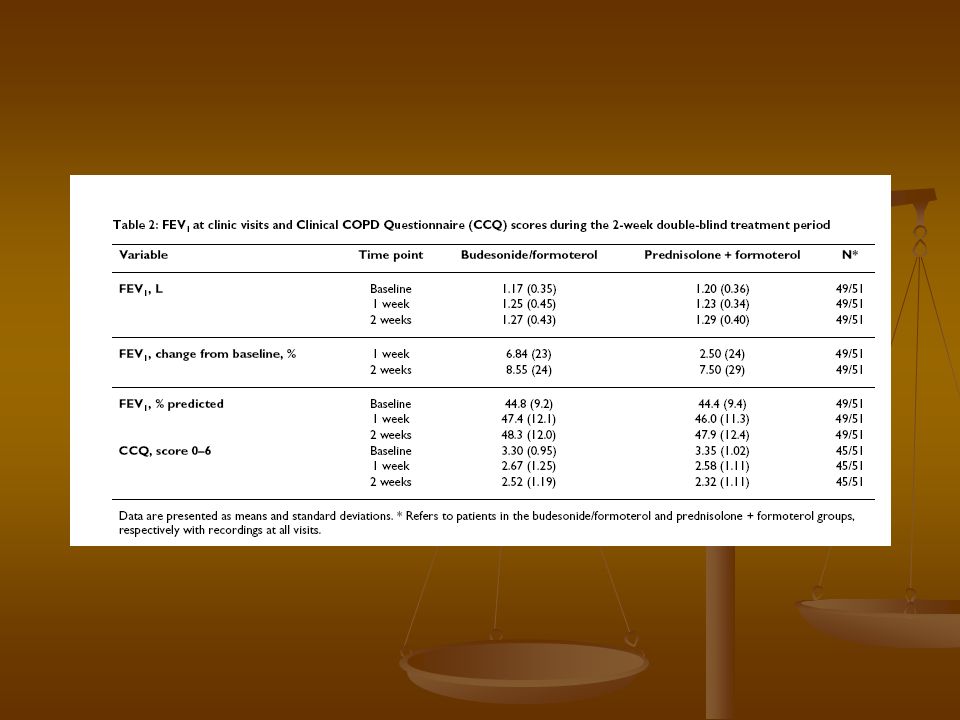
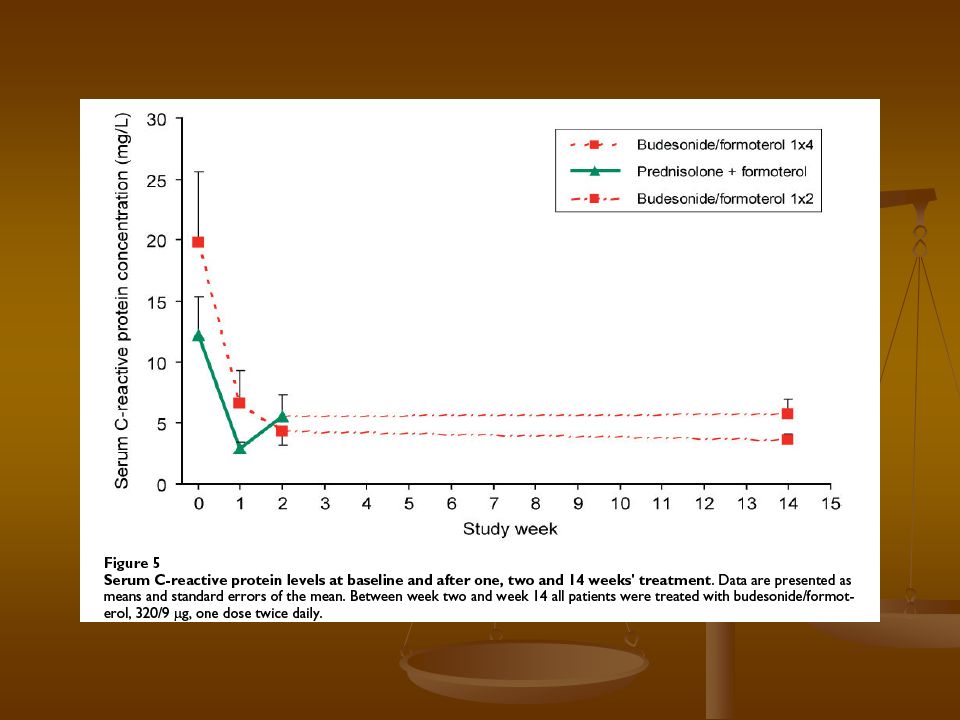
-A self administered Clinical COPD Questionnaire (CCQ)was completed at the start of the study, after one week and at the end of the double-blind period. -At all visits serum C-reactive protein (CRP) concentrations. -Safety was monitored by reporting of adverse events, serious adverse events and discontinuations due to adverse events.
 concentrations. -Safety was monitored by reporting of adverse events, serious adverse events and discontinuations due to adverse events..")
14
Results:

18
- treatment failure: - treatment failure: 2 cases in first group 2 cases in first group -Use of reliever medication -Use of reliever medication patients in the budesonide/formoterol and prednisolone plus formoterol groups used 1.8 and 2.1 inhalations per day of reliever medication, respectively. patients in the budesonide/formoterol and prednisolone plus formoterol groups used 1.8 and 2.1 inhalations per day of reliever medication, respectively.

19
Critical appraizal: Were the Pts in the two groups similar at the start of the trial with respect to prognostic factors? Were the Pts in the two groups similar at the start of the trial with respect to prognostic factors? Were Pts analysed in the groups to which they were randomized Were Pts analysed in the groups to which they were randomized

20
Blinding : Were Pts aware of group allocation? Were clinicians aware of group allocation? Were outcome assessors aware of group allocation? Were statisticians aware of group allocation?

21
Were the follow up of Pts sufficiently long & complete ? Were the follow up of Pts sufficiently long & complete ?

22
Absolute Risk Reduction (ARR): The absolute arithmetic difference in events rate. ARR= EER – CER after 1 week =6.84 % -2.5% = 4.34% after 1 week =6.84 % -2.5% = 4.34% after 2 week =8.55 % -7.5% = 1.05% after 2 week =8.55 % -7.5% = 1.05%

23
Relative Risk Reduction (RRR): Proportional reduction in rates of bad events between experimental & control group in trial. RRR =(EER-CER)/CER first week=(6.84 % -2.5 % ) /2.5% =173% first week=(6.84 % -2.5 % ) /2.5% =173% second =(8.55% -7.50)/7.50 =14% second =(8.55% -7.50)/7.50 =14%
/CER first week=(6.84 % -2.5 % ) /2.5% =173% first week=(6.84 % -2.5 % ) /2.5% =173% second =(8.55% -7.50)/7.50 =14% second =(8.55% -7.50)/7.50 =14%.")
24
Number Need to Treat ( NNT ): The number of Pts who need to be treated to achieve one additional favourable outcome. NNT = 1/ ARR =1/4.34% = 23.04 =1/4.34% = 23.04 =1/1.05%=95.24 =1/1.05%=95.24

25
Will the results help me in caring for my Pts? Were the study Pts similar to Pts in my care? Were all clinically important outcomes considered? Are the likely benefits worth the potential harms & costs?

26
discussion: - The risk of systemic side effects when using oral prednisolone – even short courses – has been well recognised and the total steroid burden may be heavy in patients with frequent exacerbations. - The risk of systemic side effects when using oral prednisolone – even short courses – has been well recognised and the total steroid burden may be heavy in patients with frequent exacerbations. - Short-term increases in the doses of inhaled budesonide have been found safe and well tolerated - Short-term increases in the doses of inhaled budesonide have been found safe and well tolerated

27
Limitation: - lack of a placebo. - this study included only patients who had a deterioration of their clinical status during the last week prior to entry. - all treatment effects were due to the initial single dose of oral steroid plus the nebulisation of bronchodilators. -duration of the prednisolone course (2 weeks) -3-month follow-up period to be sufficient to evaluate the incidence of further exacerbations. -coast effective.
 -3-month follow-up period to be sufficient to evaluate the incidence of further exacerbations. -coast effective..")
28
Conclusion: - High dose budesonide/formoterol was as effective as prednisolone plus formoterol for the ambulatory treatment of acute exacerbations in non-hospitalized COPD patients. - An early increase in budesonide/formoterol dose may therefore be tried before oral corticosteroids are used.

29
END END

Similar presentations


>")
>")
 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")















 Presented by Ali Naqvi, MD.>")
