Download presentation
Presentation is loading. Please wait.

1
Early Hearing Detection and Intervention How You Matter!
Laura Davis-Keppen, MD SD AAP EHDI Champion Professor of Pediatrics, USD Jessica J Messersmith, PhD, CCC-A, FAAA Associate Professor of Audiology, USD Pediatric and Cochlear Implant Audiologist

2
Why is early identification of hearing loss important?
Hearing loss is the most common birth condition Previous methods for detecting hearing loss have been ineffective Undetected hearing loss can delay speech, language, social & academic development Why is early identification of hearing loss important? Left untreated, hearing loss of even mild degrees interferes with speech and language development. In many cases, these delays can be long-term and lead to academic, social-emotional and behavioral consequences. When hearing loss is identified and treated early in life, these negative consequences can be prevented or minimized.

3
Hearing in Children Hearing loss is the most common birth abnormality
About 2 or 3 out of every children in the United States are born deaf or hard-of-hearing (NIDCD, ) ~ 12,000 per year ~ Another 4,000 to 6,000 infants and children are identified with hearing loss by age 3 years (NIDCD, ) WHY IS EARLY IDENTIFICATION OF HEARING LOSS IMPORTANT? One of the most elementary questions that must be answered is if it is important to identify hearing loss early. The surprising fact is that hearing loss is THE most common of the birth conditions that are typically screened for at birth. When compared with other congenital birth conditions, it is easy to see that hearing loss is much more prevalent than many birth defects that receive a great deal more attention. For example, of every 10,000 babies born, 30 will have a permanent hearing loss, while only 11 will have Down Syndrome, 5 will have spina bifida and only one will have PKU. INCIDENCE OF HEARING LOSS: Although estimates vary slightly, prevalence figures for hearing loss in children (from the CDC and NIDCD) indicate that 1 to 3 infants out of every 1000 will have some type or degree of permanent hearing loss. It is expected that 10/1000 infants from the NICU will be identified with hearing loss, whereas 1/1000 are expected from the well baby nursery. Prevalence rates are expected to increase by school age due to factors such as late onset, progressive hearing loss missed by screening and late identification of hearing loss in children.
 ~ 12,000 per year. ~ Another 4,000 to 6,000 infants and children are identified with hearing loss by age 3 years (NIDCD, 2013) WHY IS EARLY IDENTIFICATION OF HEARING LOSS IMPORTANT One of the most elementary questions that must be answered is if it is important to identify hearing loss early. The surprising fact is that hearing loss is THE most common of the birth conditions that are typically screened for at birth. When compared with other congenital birth conditions, it is easy to see that hearing loss is much more prevalent than many birth defects that receive a great deal more attention. For example, of every 10,000 babies born, 30 will have a permanent hearing loss, while only 11 will have Down Syndrome, 5 will have spina bifida and only one will have PKU. INCIDENCE OF HEARING LOSS: Although estimates vary slightly, prevalence figures for hearing loss in children (from the CDC and NIDCD) indicate that 1 to 3 infants out of every 1000 will have some type or degree of permanent hearing loss. It is expected that 10/1000 infants from the NICU will be identified with hearing loss, whereas 1/1000 are expected from the well baby nursery. Prevalence rates are expected to increase by school age due to factors such as late onset, progressive hearing loss missed by screening and late identification of hearing loss in children.")
4
Identification is crucial
Hearing is necessary to grow neural connections throughout the brain Crucial for development of spoken language, reading, and auditory learning [Gordon, Papsin, and Harrison, 2004] Even those with profound HL can achieve auditory brain access through use of current technology Allows developmental model of intervention rather than re/habilitative For auditory pathways to mature, acoustic stimulation must occur early and often -normal maturation of the CANS is a precursor to normal s/l development Kids receiving CI during 1st year of life may have greater benefit from plasticity of auditory pathways than those implanted later -plasticity is greatest during 1st 3.5 years of life -as we’ll see later, the has direct impact on the prognosis for s/l skill development when compared to HA use or later CI use Without stimulation of the auditory nerve, the brain reorganizes itself to get input from other senses, primarily vision process called cross-modal reorganization and reduces auditory neural capacity Early amp or CI stimulates the brain in its initial organization process and is therefore more receptive to auditory input results in greater auditory capacity

5
Early identification is critical
Children identified before 6 months of age have better developmental outcomes than those identified later (Yoshinaga-Itano et al., 1998) Expressive and receptive language skills Regardless of degree of hearing loss Higher vocabulary and verbal reasoning skills at age 5 for those children with hearing loss who began intervention by 11 months of age compared to children who began intervention later (Moeller, 2000)
 Expressive and receptive language skills. Regardless of degree of hearing loss. Higher vocabulary and verbal reasoning skills at age 5 for those children with hearing loss who began intervention by 11 months of age compared to children who began intervention later (Moeller, 2000)")
6
Neural projections are impacted
Gilley, Sharma, & Dorman, 2008 Left image: NH children: bilateral activation of the auditory cortical areas (superior temporal sulcus and inferior temporal gyrus) Middle image: early treatment: activation of the auditory cortical areas contralateral to their CI Right image: late treatment: activation outside the auditory cortical areas (in the visual, insula, and parietotemporal areas)
 Middle image: early treatment: activation of the auditory cortical areas contralateral to their CI. Right image: late treatment: activation outside the auditory cortical areas (in the visual, insula, and parietotemporal areas)")
7
Newborn Hearing Screening
Considerations for implementing universal screening (World Health Organization) Is the problem significant? To the individual To society Is there good evidence on an effective treatment once the problem is detected? Has the screening test been properly evaluated and shown to be appropriate in the setting where the screening is to be performed? Is there evidence that a screening program that leads to treatment is of greater benefit than waiting until symptoms develop? Have cost issues been considered and developed? Are there plausible strategies and sufficient resources to ensure implementation? Yes! Yes! Yes! PREREQUISITES FOR A POPULATION SCREENING PROGRAM: For any population screening program to be implemented, a set of criteria must be met in order for the costs of the screening to be justified. It has been determined that newborn hearing screening meets all four of these criteria: (hit mouse to have YES appear by each condition) – hearing loss is a sufficiently frequent condition in infants, it has serious consequences for development if untreated, developmental consequences can be prevented or treated through effective interventions, and effective follow up systems are in place. Yes! Yes! Yes!
 Is the problem significant To the individual. To society. Is there good evidence on an effective treatment once the problem is detected Has the screening test been properly evaluated and shown to be appropriate in the setting where the screening is to be performed Is there evidence that a screening program that leads to treatment is of greater benefit than waiting until symptoms develop Have cost issues been considered and developed Are there plausible strategies and sufficient resources to ensure implementation Yes! Yes! Yes! PREREQUISITES FOR A POPULATION SCREENING PROGRAM: For any population screening program to be implemented, a set of criteria must be met in order for the costs of the screening to be justified. It has been determined that newborn hearing screening meets all four of these criteria: (hit mouse to have YES appear by each condition) – hearing loss is a sufficiently frequent condition in infants, it has serious consequences for development if untreated, developmental consequences can be prevented or treated through effective interventions, and effective follow up systems are in place. Yes! Yes! Yes!")
8
Previous methods for detecting hearing loss have been ineffective
High risk screening failed to identify ~ 50% of the infants with hearing loss Large retrospective cohort study5, 6: mean age of diagnosis 21.6 months Similar findings reported in US7,8,9 WHY IS EARLY IDENTIFICATION OF HEARING LOSS IMPORTANT? In the past, methods for detecting hearing loss in newborns and infants were not as effective as they are today. Therefore, universal newborn hearing screening was not feasible. Those methods included high-risk registries and observing behavioral responses to loud sounds. A large retrospective cohort study5, 6 reported on the outcomes of 86 Australian children who were identified prior to the implementation of newborn hearing screening protocols. The average age of identification was 21.6 months and the average age of hearing aid fitting was 23.2 months. Similar findings have been reported in the US.7,8,9 Late identification of hearing loss has developmental and behavioral consequences for the child, and it places families in a reactive rather than a proactive position in managing the needs of the child.

9
EHDI: Early Hearing Loss Detection and Intervention
The process

10
Early Identification of Hearing Loss- Method
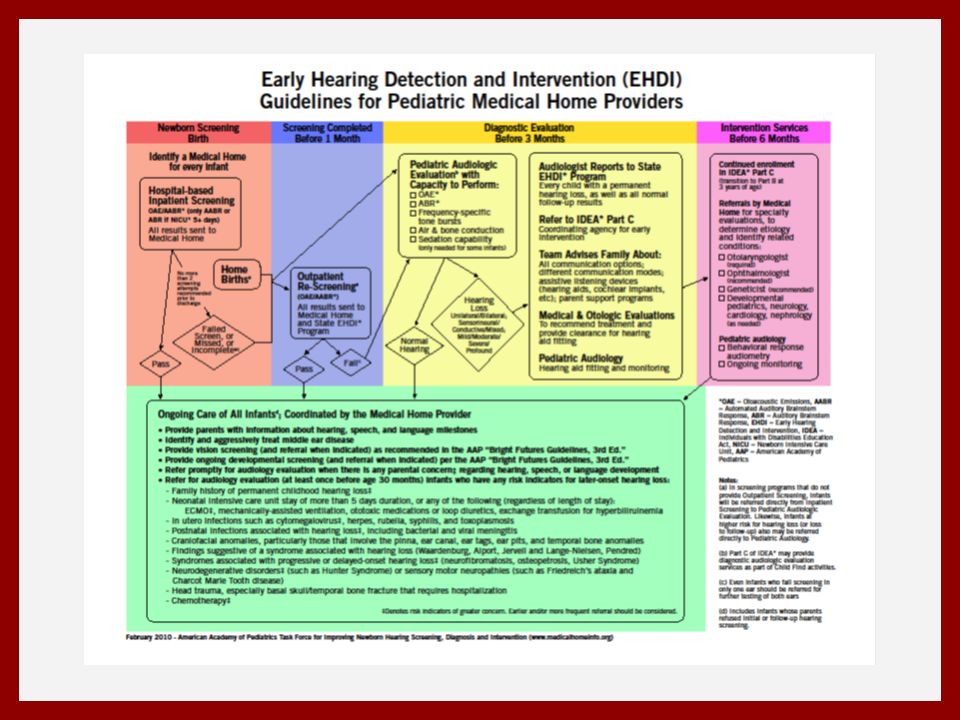
Screening No later than 1 month of age Diagnostic testing with Pediatric Audiologist No later than 3 months of age Early Intervention No later than 6 months of age Wednesday, December 22, 2010, the President signed into law the Early Hearing Detection and Intervention (EHDI) Act, providing state funding for EHDI programs. Medical and genetics evaluation if dx with HL Before newborn hearing screening was instituted universally, children with severe-to-profound hearing loss, on average, completed the 12th grade with a 3rd-to 4th-grade reading level and language levels of a 9-to 10-year-old hearing child. In contrast, infants and children with mild-to-profound hearing loss who are identified in the first 6 months of life and provided with immediate and appropriate intervention have significantly better outcomes than later-identified infants and children in vocabulary development, receptive and expressive language, syntax, speech production, and social-emotional development. Children enrolled in early intervention within the first year of life have also been shown to have language development within the normal range of development at 5 years of age. The goal of amplification-device fitting is to provide the infant with maximum access to all of the acoustic features of speech within an intensity range that is safe and comfortable. To accomplish this in infants, amplification-device selection, fitting, and verification should be based on a prescriptive procedure that incorporates individual real-ear measures that account for each infant’s ear-canal acoustics and hearing loss. As the hearing loss becomes more specifically defined through audiological assessments and as the child’s ear-canal acoustics change with growth, refinement of the individual prescriptive hearing-aid gain and output targets is necessary. CI should be consideration for any child who seems to receive limited benefit from a trial with appropriately fitted hearing aids. 1:3:6
 Act, providing state funding for EHDI programs. Medical and genetics evaluation if dx with HL. Before newborn hearing screening was instituted universally, children with severe-to-profound hearing loss, on average, completed the 12th grade with a 3rd-to 4th-grade reading level and language levels of a 9-to 10-year-old hearing child. In contrast, infants and children with mild-to-profound hearing loss who are identified in the first 6 months of life and provided with immediate and appropriate intervention have significantly better outcomes than later-identified infants and children in vocabulary development, receptive and expressive language, syntax, speech production, and social-emotional development. Children enrolled in early intervention within the first year of life have also been shown to have language development within the normal range of development at 5 years of age. The goal of amplification-device fitting is to provide the infant with maximum access to all of the acoustic features of speech within an intensity range that is safe and comfortable. To accomplish this in infants, amplification-device selection, fitting, and verification should be based on a prescriptive procedure that incorporates individual real-ear measures that account for each infant’s ear-canal acoustics and hearing loss. As the hearing loss becomes more specifically defined through audiological assessments and as the child’s ear-canal acoustics change with growth, refinement of the individual prescriptive hearing-aid gain and output targets is necessary. CI should be consideration for any child who seems to receive limited benefit from a trial with appropriately fitted hearing aids. 1:3:6.")
11
Screening method AABR OAE More $$$ than OAE
Sensitive to more types of HL Needed if baby in NICU >5 days Less $$$ than AABR Faster than AABR Not sensitive to all types of HL Can obtain invalid results from both if obstruction in middle or outer ear (e.g. fluid or vernix) Explain what each measure is. Each hospital that implements Universal Newborn Hearing Screening must decide which of the 3 screening program choices is most cost-effective for their population and region. Factors to consider include the number of births performed each year, the availability of trained personnel to perform screening, the ability of families to complete follow-up testing, and available services in the area.
 Explain what each measure is. Each hospital that implements Universal Newborn Hearing Screening must decide which of the 3 screening program choices is most cost-effective for their population and region. Factors to consider include the number of births performed each year, the availability of trained personnel to perform screening, the ability of families to complete follow-up testing, and available services in the area.")
12
2007 JCIH Position on Screening2
NICU >5 days in NICU ABR should be included to screen for neural loss Rescreen BOTH ears, even if only one ear fails Non pass – refer to Audiologist Readmission – rescreen before discharge Well baby nursery Screen with OAE or ABR Repeat screen when necessary before discharge When using 2 step protocol test order should be OAE then ABR Rescreen BOTH ears, even if only one ear doesn’t pass This slide summarizes the recommendations of the Joint Committee on Infant Hearing (2007) regarding screening of infants in the NICU vs. the newborn nursery. As noted on the slide, ABR should be included for all infants spending > 5 days in the NICU. This allows the audiologist to screen for Auditory Neuropathy in these infants. Repeat screening for non passes is recommended for both groups of newborns. This helps reduce false positive rates. If a baby refers for only one ear, BOTH ears should be rescreened.
 regarding screening of infants in the NICU vs. the newborn nursery. As noted on the slide, ABR should be included for all infants spending > 5 days in the NICU. This allows the audiologist to screen for Auditory Neuropathy in these infants. Repeat screening for non passes is recommended for both groups of newborns. This helps reduce false positive rates. If a baby refers for only one ear, BOTH ears should be rescreened.")
13
Does UNHS Improve the Age of Identification and Intervention?
Prior to UNHS (Harrison and Roush, 1996) Median age of identification without risk factors was 13 months for severe-to-profound SNHL Median age of identification with risk factors was 12 months for severe-to-profound SNHL After UNHS (NY State, 2000) Median age of identification was 3 months EHDI 10 years later- (Holte et al., 2012) only 32% children included in NIH OCHL study met all of the 1‐3‐6 benchmarks Harrison, Roush and Wallace Follow-Up (2001) 181 babies born between Dec and Dec. 2000 46% had hearing screening at birth – median age of ID was 3 months 54% did not have hearing screening at birth – similar median age of ID compared to 1996 study
 Median age of identification without risk factors was 13 months for severe-to-profound SNHL. Median age of identification with risk factors was 12 months for severe-to-profound SNHL. After UNHS (NY State, 2000) Median age of identification was 3 months. EHDI 10 years later- (Holte et al., 2012) only 32% children included in NIH OCHL study met all of the 1‐3‐6 benchmarks. Harrison, Roush and Wallace Follow-Up (2001) 181 babies born between Dec and Dec % had hearing screening at birth – median age of ID was 3 months. 54% did not have hearing screening at birth – similar median age of ID compared to 1996 study.")
14
What is the role of the provider and nurse?
Initial hospital Pass No pass Discuss results Facilitate visit for rescreen Like any newborn screen, the initial screen is not diagnostic As the primary care physician, how should you react when a child doesn’t pass a newborn hearing screening? Statistically, we know that 3/1000 babies will have some degree of permanent hearing loss. A good newborn hearing screening program will have a refer rate of about 3-4%, so about 10 times as many babies who have hearing loss will be referred. So it is reassuring for parents to know that most babies who receive a refer of the newborn hearing screening will actually have normal hearing. If a baby was screened in a good screening program, referral rates should be low, so the babies who really need it are receiving further testing. As physicians you want to find the right balance between reducing parental worries and emphasizing the importance of completing the recommended follow-up testing.

15
What is the role of the provider and nurse?
Initial hospital Pass No pass Ensure that family understands that a “pass” does not mean that a HL will not be dx later on Children who pass UNHS but have risk factor should have at least one dx audiology assessment by months of age (JCIH, 2007) JCIH (2007), recommends that infants who pass the neonatal screening but have a risk factor should have at least one diagnostic audiology assessment by months of age. Earlier and more frequency assessments may be indicated for CMV, syndromes, neurodegenerative disorders, trauma, or postnatal infections associated with SNHL, children who receive ECMO or chemotherapy
 JCIH (2007), recommends that infants who pass the neonatal screening but have a risk factor should have at least one diagnostic audiology assessment by months of age. Earlier and more frequency assessments may be indicated for CMV, syndromes, neurodegenerative disorders, trauma, or postnatal infections associated with SNHL, children who receive ECMO or chemotherapy.")
16
What is the role of the provider and nurse?
Initial hospital Pass No pass Rescreen Pass No Pass Effective communication achieves a balance between reassuring the family that the child might have normal hearing, but stressing the critical importance of follow up testing (“Your child may or may not have a hearing loss…but let’s be sure about it. If further testing shows hearing loss, the earlier we get started helping the child, the better.”) In a hospital with a 2% refer rate, a baby has a 1 in 10 chance of having a hearing loss. Minimizing the importance of a referral for further testing can have serious consequences in delaying the diagnosis of actual hearing loss. Ensure that the family takes the child for dx audiologic assessment Connect infants to audiologic follow-up
 In a hospital with a 2% refer rate, a baby has a 1 in 10 chance of having a hearing loss. Minimizing the importance of a referral for further testing can have serious consequences in delaying the diagnosis of actual hearing loss. Ensure that the family takes the child for dx audiologic assessment. Connect infants to audiologic follow-up.")
17
Who is an audiologist? Audiologist are the primary health care professional who diagnose, treat, and manage hearing loss, tinnitus, and/or balance disorders. Doctoral level education Licensure requirements Certification We work with individuals from birth through adulthood. Audiologists determine appropriate patient treatment of hearing and balance problems with a variety of specialized auditory and vestibular assessments. Audiologists dispense and fit hearing aids, cochlear implants, and other hearing assistive technology as part of a comprehensive re/habilitative program Of all the gifts bestowed upon humanity, the ability to communicate is one of the most important. Any impairment of this ability can have far-reaching consequences, affecting every aspect of a person's life, from learning, to work, to interactions with family, friends, and community. Audiologists and speech-language pathologists provide services to prevent, diagnose, evaluate, and treat communication disorders. Indicators for the Need for Audiologists (SLPs and SLH) Dramatic increases in referrals of preschool and school-age children for speech, language and hearing services Changes in U.S. demographics - growing aging population Larger bilingual populations: It is estimated that more than 5 million individuals from culturally and linguistically diverse backgrounds have a speech, language, or hearing disability National public health policy agenda for early identification (and intervention) and diagnosis of hearing disorders in infants and toddlers Greater success in the use of life-saving measures at birth of children with potential for communication disorders Greater emphasis on rehabilitation priorities as a result of an increased number of young adults with closed-head injuries, blast injury survivors and the "graying of America" Passage of federal laws and regulations addressing the needs of individuals with disabilities Individuals with Disability Education Act (IDEA) Americans with Disabilities Act (ADA) Rehabilitation Act of 1973 as Amended by the Rehabilitation Act of 1984 Health Professions Act - Title VII of the Public Health Service Act Disadvantaged Minority Health Improvement Act Medicare and Medicaid OR--- An audiologist is a professional who diagnoses, treats, and manages individuals with hearing loss or balance problems. Audiologists have received a master's or doctoral degree from an accredited university graduate program. Their academic and clinical training provides the foundation for patient management from birth through adulthood. Audiologists determine appropriate patient treatment of hearing and balance problems by combining a complete history with a variety of specialized auditory and vestibular assessments. Based upon the diagnosis, the audiologist presents a variety of treatment options to patients with hearing impairment or balance problems. Audiologists dispense and fit hearing aids as part of a comprehensive habilitative program. Audiologists may be found working in medical centers and hospitals, private practice settings, schools, government health facilities and agencies, as well as colleges and universities. As a primary hearing health provider, audiologists refer patients to physicians when the hearing or balance problem requires medical or surgical evaluation or treatment.
 Dramatic increases in referrals of preschool and school-age children for speech, language and hearing services. Changes in U.S. demographics - growing aging population. Larger bilingual populations: It is estimated that more than 5 million individuals from culturally and linguistically diverse backgrounds have a speech, language, or hearing disability. National public health policy agenda for early identification (and intervention) and diagnosis of hearing disorders in infants and toddlers. Greater success in the use of life-saving measures at birth of children with potential for communication disorders. Greater emphasis on rehabilitation priorities as a result of an increased number of young adults with closed-head injuries, blast injury survivors and the graying of America Passage of federal laws and regulations addressing the needs of individuals with disabilities. Individuals with Disability Education Act (IDEA) Americans with Disabilities Act (ADA) Rehabilitation Act of 1973 as Amended by the Rehabilitation Act of Health Professions Act - Title VII of the Public Health Service Act. Disadvantaged Minority Health Improvement Act. Medicare and Medicaid. OR--- An audiologist is a professional who diagnoses, treats, and manages individuals with hearing loss or balance problems. Audiologists have received a master s or doctoral degree from an accredited university graduate program. Their academic and clinical training provides the foundation for patient management from birth through adulthood. Audiologists determine appropriate patient treatment of hearing and balance problems by combining a complete history with a variety of specialized auditory and vestibular assessments. Based upon the diagnosis, the audiologist presents a variety of treatment options to patients with hearing impairment or balance problems. Audiologists dispense and fit hearing aids as part of a comprehensive habilitative program. Audiologists may be found working in medical centers and hospitals, private practice settings, schools, government health facilities and agencies, as well as colleges and universities. As a primary hearing health provider, audiologists refer patients to physicians when the hearing or balance problem requires medical or surgical evaluation or treatment.")
18
Only refer infants to a pediatric audiologist
Discuss audiology

19
A pediatric audiologist is best equipped to diagnose hearing loss in infants/children
Detailed history Diagnostic evaluation using a test battery No one single test can identify the type, degree, and configuration of HL Otoscopy Immitance Physiologic Behavioral Counsel parents Discuss impact of parent choice on treatment plan No age limit on fitting amplification

20
Treatment plan Mode of communication is parent(s) choice
If spoken- pursue amplification ASAP (pediatric audiologist) No age limit on fitting amplification Cochlear Implant Center should be involved in those case of severe or greater HL, bacterial meningitis, ANSD, those demonstrating limited benefit from amplification If sign- connect family with sign support
 No age limit on fitting amplification. Cochlear Implant Center should be involved in those case of severe or greater HL, bacterial meningitis, ANSD, those demonstrating limited benefit from amplification. If sign- connect family with sign support.")
21
What is the role of the provider and nurse?
Talk with family about results Review family history and examine child for craniofacial abnormalities or syndromes associated with hearing loss Refer to ENT Refer to ophthalmology Refer for genetic testing/consultation Audiologist No Dx HL Dx HL

22
National EHDI Data Universal Newborn Hearing Screening

23
Incidence of Children who are Deaf or Hard of Hearing
Infants Identified as Permanently Deaf or Hard Of Hearing , Total = 34,416 National EHDI Data Incidence of Children who are Deaf or Hard of Hearing

24
2012 National CDC EHDI Data % Screened: 96.6% (n=3,820,624) Prevalence of children who are deaf/hh: 1.6 per 1,000 screened (Range per 1,000) % of those identified receiving Early Intervention: 61.7% (n=3,527) % Screened before 1 month of age: 86.0% (n=3,287,614) % Diagnosed before 3 months of age: 69.1% (n=20,102) % Receiving Intervention before 6 months of age: 67.1% (n=2,367) % Loss to Follow-up or Documentation: 35.9% (n=19,006)
 % Screened before 1 month of age: 86.0% (n=3,287,614) % Diagnosed before 3 months of age: 69.1% (n=20,102) % Receiving Intervention before 6 months of age: 67.1% (n=2,367) % Loss to Follow-up or Documentation: 35.9% (n=19,006)")
25
2012 South Dakota EHDI Data % Screened: 97% (n=12,722) , 96.4% by 1 month Rescreened 65% Audiologist by 3 months 77.7% Birth to 3 only 18.75% 33.4% of South Dakota’s newborns who should have been rescreened did not have hearing evaluated. Based on national data 68.6% of SD infants who were deaf/HH did not receive early diagnosis and intervention. Early intervention should be considered a developmental emergency. Children identified as deaf/hh who begin services before 6 months develop language (spoken or signed) on a par with their hearing peers. 86.8% loss to follow-up/loss of documentation
 on a par with their hearing peers. 86.8% loss to follow-up/loss of documentation.")
26
The Role of Medical Home
DRAFT EHDI 101 PPT Early Hearing Detection and Intervention The Role of Medical Home The medical home plays a key role in the success of EHDI programs. A medical home can help families understand the EHDI process. The medical home ensures that appropriate and timely steps are taken to identify children who are deaf/hh and get them into an early intervention program. The medical home serves as the primary coordinating entity which can help significantly reduce loss to follow-up/documentation.

27
Medical Home: Strategies to Promote Follow Up
At prenatal visit, encourage families to identify you as follow-up care location Inform hospital to facilitate communication of results Provide checkbox on newborn well child form/patient chart for hearing screening results & risk factors AAP: The primary care provider must assume responsibility to ensure that audiological assessment is conducted on infants who do not pass screening and must initiate referral for medical specialty evaluations necessary to determine the etiology of the hearing loss. Set up tracking system for infants who do not pass hearing screening. If there is a prenatal visit, encourage families to state you will be the follow-up care location and to inform the hospital so that information sharing can occur more readily. Have a check box on the newborn well child form that includes results of hearing screening (this makes for a reminder to check on the results). Also developing a tracking system for hearing screening if children didn’t pass (or adding it to the metabolic screening tracking system in the office) to ensure children are not lost to follow-up.
. Also developing a tracking system for hearing screening if children didn’t pass (or adding it to the metabolic screening tracking system in the office) to ensure children are not lost to follow-up.")
28
Counseling Parents Effective communication of results to families has an influence on follow up behaviors Balance between reassurance and importance of follow up testing “Your infant may or may not have a hearing loss…but let’s be sure about it. If further testing shows hearing loss, the earlier we get started helping the child, the better.” Effective communication achieves a balance between reassuring the family that the child might have normal hearing, but stressing the critical importance of follow up testing (“Your child may or may not have a hearing loss…but let’s be sure about it. If further testing shows hearing loss, the earlier we get started helping the child, the better.”) In a hospital with a 2% refer rate, a baby has a 1 in 10 chance of having a hearing loss. Minimizing the importance of a referral for further testing can have serious consequences in delaying the diagnosis of actual hearing loss.
 In a hospital with a 2% refer rate, a baby has a 1 in 10 chance of having a hearing loss. Minimizing the importance of a referral for further testing can have serious consequences in delaying the diagnosis of actual hearing loss.")
29
Optimal Surveillance in the Medical Home (JCIH, 2007)2
If hearing loss is diagnosed, refer siblings of infant for audiological evaluation Refer infants with any RISK indicators for audiological assessment by months of age Carefully assess middle ear status at all well child visits; refer for otologic evaluation if persistent middle ear effusion lasts for > 3 months JCIH also recommends: -testing siblings of infants identified with hearing loss (because 50% of hearing loss may be of genetic origin) -referring any infants with RISK indicators (next slide) for audiological evaluations -and routine monitoring of middle ear status
 -referring any infants with RISK indicators (next slide) for audiological evaluations. -and routine monitoring of middle ear status.")
30
Risk Indicators of Delayed Onset or Progressive Hearing Loss
Caregiver concerns* about hearing, speech, language, development Family history* of permanent childhood hearing loss NICU stay > 5 days or any of following (regardless of length of stay): ECMO assisted ventilation* Ototoxic medications (gentamycin, tobramycin) Loop diuretics (furosemide, Lasix) Hyperbilirubinemia requiring exchange transfusion Risk factors for delayed onset or progressive hearing loss. JCIH, 2007
: ECMO assisted ventilation* Ototoxic medications (gentamycin, tobramycin) Loop diuretics (furosemide, Lasix) Hyperbilirubinemia requiring exchange transfusion. Risk factors for delayed onset or progressive hearing loss. JCIH,")
31
Risk Indicators for permanent congenital, delayed onset or progressive hearing loss2
In Utero infections CMV*, herpes, rubella, syphilis, toxoplasmosis Craniofacial anomalies Physical findings (e.g. white forelock) Syndromes* involving hearing loss Neurofibromatosis, osteopetrosis, Usher, Waardenburg, Alport, Pendred, Jervell & Lange- Nielson Continuation of risk factors for late onset or progressive hearing loss. * = greater risk for delayed onset HL
 Syndromes* involving hearing loss. Neurofibromatosis, osteopetrosis, Usher, Waardenburg, Alport, Pendred, Jervell & Lange- Nielson. Continuation of risk factors for late onset or progressive hearing loss. * = greater risk for delayed onset HL.")
32
Risk Indicators for permanent congenital, delayed onset or progressive hearing loss2
Neurodegenerative disorders Sensory motor neuropathies (Frieidrich ataxia, Charcot-Marie-Tooth) Culture positive postnatal infections associated with HL* Herpes, varicella, meningitis Head trauma (basal skull, temporal bone)* Chemotherapy* Continuation of risk factors for late onset or progressive hearing loss. * = greater risk for delayed onset HL
 Culture positive postnatal infections associated with HL* Herpes, varicella, meningitis. Head trauma (basal skull, temporal bone)* Chemotherapy* Continuation of risk factors for late onset or progressive hearing loss. * = greater risk for delayed onset HL.")
33
Medical Workup Complete prenatal & perinatal history
Family Hx of onset of HL < age 30 Physical exam: unusual facial appearance with attention to asymmetry, ear anomalies, neurologic, balance, skeletal, other unusual physical findings Test for CMV as soon as possible, before age 6 weeks. Refer to ENT Refer to Genetics and Ophthalmology As needed: developmental pediatrics, cardiology, neurology Additional Considerations: Dr. Betty Vohr (a leader in NHS in the US) and Professor of Pediatrics at Women and Infants Hospital in Rhode Island recommends a medical workup including the evaluations on the slide above. One third of all infants with hearing loss will have additional disabilities. For this reason, physicians should closely monitor all developmental domains, and may want to refer for multi-disciplinary assessment. A medical genetics referral may be indicated to support differential diagnosis of health conditions and/or to support the family in identifying the etiology of hearing loss. Ophthalmologic evaluation should be conducted routinely on children with hearing loss. The medical genetics evaluation can be helpful even in the presence of neonatal risk factors as children can have genetic causes of HL despite the fact that prematurity played a role. Also, it is likely that you will NOT need a genetics evaluation in the case of a child who passed the newborn screen and then got meningitis.
 and Professor of Pediatrics at Women and Infants Hospital in Rhode Island recommends a medical workup including the evaluations on the slide above. One third of all infants with hearing loss will have additional disabilities. For this reason, physicians should closely monitor all developmental domains, and may want to refer for multi-disciplinary assessment. A medical genetics referral may be indicated to support differential diagnosis of health conditions and/or to support the family in identifying the etiology of hearing loss. Ophthalmologic evaluation should be conducted routinely on children with hearing loss. The medical genetics evaluation can be helpful even in the presence of neonatal risk factors as children can have genetic causes of HL despite the fact that prematurity played a role. Also, it is likely that you will NOT need a genetics evaluation in the case of a child who passed the newborn screen and then got meningitis.")
34
Causes of Prelingual Hearing Loss > 40dB

35
Waardenburg Syndrome Abnormal pigmentation of skin and hair
Lateral displacement of medial canthi-type I Heterochromia iridis Deafness in some-not always present

36
Branchio-Oto-Renal (BOR) Syndrome
Pre-auricular pits 82% Branchial fistulae 49% Cupped or mildly altered auricle 36% Renal abnormalities 67% Hearing loss 93% •Mixed 52% •Conductive 33% •Sensorineural 29% Autosomal Dominant: EYA1 gene (8q13.3) or SIX5 gene (19q13.32)
 or SIX5 gene (19q13.32)")
38
Treacher Collins Syndrome
Malar hypoplasia Downslanting palpebral fissures Defects of lower lid Malformations of external ear

39
Usher syndrome 3-6% of Children Who Are Deaf or Hard of Hearing Develop retinitis pigmentosa-deterioration of vision Left: Usher syndrome-Optic nerve-pale, Vessels (stars) very thin, Characteristic pigment (double arrows)
 very thin, Characteristic pigment (double arrows)")
40
Usher Syndrome Usher Syndrome Type I (70%) Type II (26%) Type III (4%)
Congenital, profound SNHL Childhood onset of retinitis pigmentosa “Clumsiness” & developmental delay Absent vestibular function Type II (26%) Congenital SNHL, high frequency > low frequency, stable Later onset of retinitis pigmentosa Normal vestibular function Type III (4%) Normal hearing and vision at birth Deterioration of hearing and vision over the years
 Congenital SNHL, high frequency > low frequency, stable. Later onset of retinitis pigmentosa. Normal vestibular function. Type III (4%) Normal hearing and vision at birth. Deterioration of hearing and vision over the years.")
41
Jervell and Lange-Neilsen Syndrome
Prolongation of QT interval on EKG. May develop arrhythmias leading to sudden death • Profound sensorineural hearing loss • Autosomal recessive inheritance. Due to mutations in the KVLQT1 gene on chromosome 11p15 and KCNE1 gene on chromosome 21q22 • potassium channel genes

42
70% of Genetic Hearing Loss is Nonsyndromic
DFNB1 locus which includes the GJB2 gene encoding the gap junction protein connexin 26 and GJB6 gene encoding the gap junction protein connexin 30 is the most common cause of AR nonsyndromic HL Next-generation sequencing technologies are replacing single gene-sequencing tests for hearing loss. Advantage: ability to address genetic heterogeneity since many different genes results in phenotypes that cannot be distinguished clinically. Disadvantage: Large deletions and duplications and copy-number and structural variations not as efficiently detected so alternative genetic testing strategies may be necessary

43
Comprehensive Genetic Testing for Hereditary HL Using Massively Parallel Sequencing
The most common cause of prelingual-onset SNHL is genetic in developed countries Panels may test for all genes known to cause NSHL, Usher syndrome, and Pendred syndrome using custom-targeted sequence capture for DNA enrichment followed by massively parallel DNA sequencing. All genes sequenced at the same time. The panel we use currently tests for 109 genes known to cause NSHL and some syndromic HL. Total of genes currently tested 116 genes. Cost effective-$1500. Familial mutation testing $200.

44
Targeted Next-Generation Sequencing of Deafness Genes
When 30 individuals with nonsyndromic hearing loss were tested using targeted next-gen sequencing , 52% of the probands were diagnosed with monogenic nonsyndromic HL Determining the etiology of HL provides answers: recurrence risk, prognosis (will HL worsen over time), best treatment (cochlear implants or hearing aids), and whether vision will also be later affected.
, best treatment (cochlear implants or hearing aids), and whether vision will also be later affected.")
45
Other Tests/Recommendations
CMV recommended as an initial test if the NB hearing screen is not passed. Congenital CMV is a leading cause of hearing loss- found in 30%. CMV testing most diagnostic when done before 3-6 weeks. With increasing age there is a greater likelihood that a +CMV test is due to postnatal exposure. Consider testing for mitochondrial mutations associated with aminoglycoside ototoxicity for individuals with a history of aminoglycoside antibiotics Every infant with confirmed HL should have an evaluation by an ophthalmologist. Temporal bone imagining should be considered if indicated.

46
CMV CMV is the leading cause of nongenetic hearing loss
1/3 of NSHL in young children At birth infant may be asymptomatic or have microcephaly, IUGR, petechiae, hepatosplenomegaly Hearing loss may be fluctuating and progressive Stabilization or improvement of hearing with antiviral tx Test for CMV if initial hearing screen not passed. This testing is mandated in some states.

47
Hearing Screening Myths Misconception vs Clinical Fact
Parents can tell if their child has a hearing loss by age 2-3 months Parents/physicians can test for hearing loss by clapping hands or banging pots near the baby Hearing loss risk factor assessments will identify all children with hearing loss Hearing loss if rare, so newborn hearing screening is not necessary There is no rush to identify hearing loss Before NB hearing screening hearing loss not recognized until 2- 3 years of age; age 4 if milder Babies who are deaf/HH can still startle to loud noises but may not be able to hear all the sounds important for speech 50% of infants who are deaf/HH have no known risk factors Hearing loss affects 1-3 per births-the most common condition Identification before 6 mo. can avoid speech and language delays through evidence-based early intervention

48
Hearing Screening Myths Misconception vs Clinical Fact
Children younger than 12 months cannot be fitted with hearing aids Babies need to be sedated to complete ABR testing Fluid prevents completion of diagnostic ABR Abnormal OAEs along with a flat tympanogram (normal volume) confirms a conductive hearing loss Newborns can be fit with amplification Babies younger than 3 months can typically be tested without need for sedation Underlying sensory loss can and should be ruled out as soon as possible through use of bone conduction ABR stimuli Diagnostic ABR including bone conduction testing is needed in combinations with OAE and tympanograms for a complete diagnosis of type and degree of hearing loss in each ear.
 confirms a conductive hearing loss. Newborns can be fit with amplification. Babies younger than 3 months can typically be tested without need for sedation. Underlying sensory loss can and should be ruled out as soon as possible through use of bone conduction ABR stimuli. Diagnostic ABR including bone conduction testing is needed in combinations with OAE and tympanograms for a complete diagnosis of type and degree of hearing loss in each ear.")
49
The Role of Medical Home
Do listen to parents concerns Encourage prompt follow-up with rescreens and diagnostic evaluations Make sure diagnostic evaluations are done by an audiologist who has experience with infants Set up electronic medical record (EMR) system to include results of auditory screening Flag all patient charts for children that require follow-up for hearing screens Flag all patient charts for children that are at risk for late onset hearing loss The Role of Medical Home
 system to include results of auditory screening. Flag all patient charts for children that require follow-up for hearing screens. Flag all patient charts for children that are at risk for late onset hearing loss. The Role of Medical Home.")
50
Infants identified as deaf or hard of hearing
Address the family’s concerns Ensure the family is seeing an experienced pediatric audiologist Refer the family to appropriate specialists Otolaryngology, Genetics, Ophthalmology Help the family obtain early intervention services Monitor developmental milestones and ear infections

51
Resources: Birth to 3 Program Early Intervention Parent Physician
SDSD (South Dakota School for the Deaf) Birth to 3 Program Parent Physician hi.htm This slide lists some valuable contacts related to follow up.
 Birth to 3 Program. Parent Physician hi.htm. This slide lists some valuable contacts related to follow up.")
Similar presentations














 1, 2 All infants will access hearing screening using a physiologic.>")

 ~ Challenges and Opportunities ~>")

 October 11, 2013 Dee Robertson, MA, CRC, Community Consultant Michigan Early Hearing.>")

