Download presentation
Presentation is loading. Please wait.

1
Bias Correction in Pharmaceutical Risk-Benefit Assessment Bob Obenchain, PhD, FASA Risk-Benefit Statistics LLC Yin = Dark = Evil = Risk Yang = Light = Good = Benefit

2
Outline: Covariate Adjustment (Simplistic, Global Modeling) is Inadequate Local Control methods take BIG Steps in Right Directions. Emerging Credibility Crisis in Pharmaceutical Safety

3
Shah BR, Laupacis A, Hux JE, Austin PC. Propensity score methods gave similar results to traditional regression modeling in observational studies: a systematic review. J Clin Epidemiol 2005; 58: 550–559. Stürmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Schneeweiss S. A review of the application of propensity score methods yielded increasing use, advantages in specific settings, but not substantially different estimates compared with conventional multivariable methods. [REVIEW ARTICLE] J Clin Epidemiol 2006; 59: 437– 447. With titles like these, do you really need to read the paper?

4
Heckman JJ. Sample selection bias as a specification error. Econometrica 1979; 47: 153–161. Crown WE, Obenchain RL, Engelhart L, Lair TJ, Buesching DP, Croghan TW. The application of sample selection models in evaluating treatment effects: the case for examining the effects of antidepressant medication. Stat Med 1998; 17, 1943–1958. Obenchain RL, Melfi CA. Propensity score and Heckman adjustments for treatment selection bias in database studies. 1997 Proceedings of the Biopharmaceutical Section. Alexandria, VA: American Statistical Association. 1998; 297–306. Early CA Modeling Efforts

5
DAgostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. [TEACHERS CORNER] Stat Med 1998; 17: 2265–2281. Highly Influential ??? Claimed that 3 rd form of PS Adjustment (after matching and sub-grouping) was to simply use some function of PS estimates as an additional X in Covariate Adjustment.
 was to simply use some function of PS estimates as an additional X in Covariate Adjustment..")
6
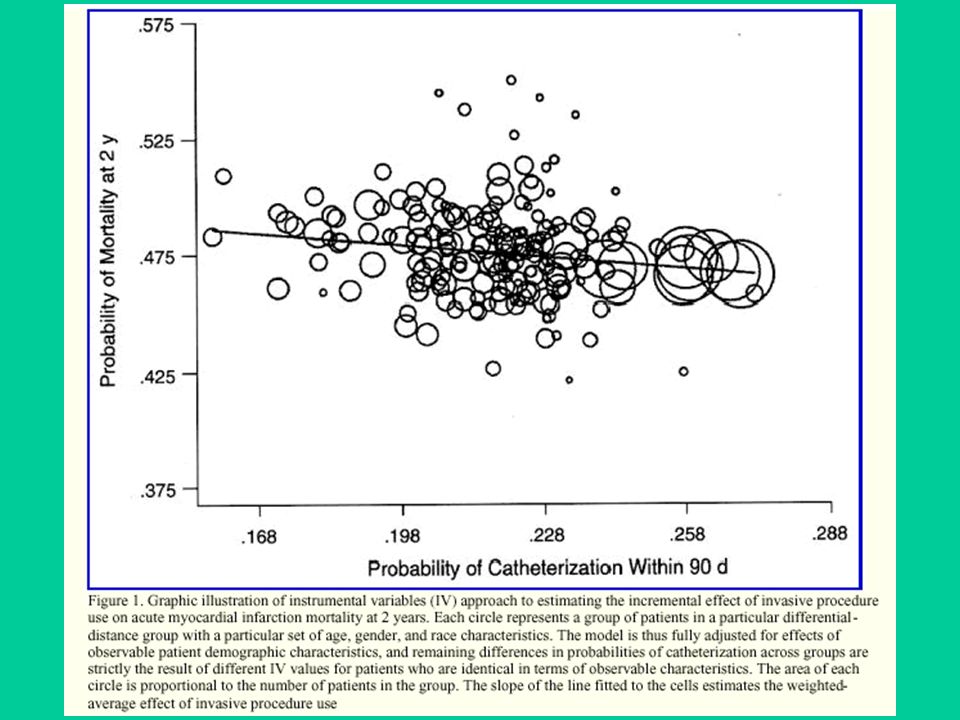
Epidemiology (case-control & cohort) studies Post-stratification and re-weighting in surveys Stratified, dynamic randomization to improve balance on predictors of outcome Matching and Sub-grouping using Propensity Scores Econometric Instrumental Variables (LATEs) Marginal Structural Models (IPW 1/PS) Unsupervised Propensity Scoring: Nested Treatment- within-Cluster ANOVA model …with LATE, LTD and Error sources of variation History of Local Control Methods for Human Studies
 studies Post-stratification and re-weighting in surveys Stratified, dynamic randomization to improve balance on predictors of outcome Matching and Sub-grouping using Propensity Scores Econometric Instrumental Variables (LATEs) Marginal Structural Models (IPW 1/PS) Unsupervised Propensity Scoring: Nested Treatment- within-Cluster ANOVA model …with LATE, LTD and Error sources of variation History of Local Control Methods for Human Studies")
7
Local Terminology: Subgroups of Patients Subclasses… Strata… Clusters… (natural or forced)
")
8
Notation for Variables y = observed outcome variable(s) x = observed baseline covariate(s) t = observed treatment assignment (usually non-random) z = unobserved explanatory variable(s)
 x = observed baseline covariate(s) t = observed treatment assignment (usually non-random) z = unobserved explanatory variable(s)")
9
Fundamental PS Theorem Joint distribution of x and t given p: Pr( x, t | p ) Pr( x | p ) Pr( t | x, p ) = Pr( x | p ) Pr( t | x ) = Pr( x | p ) times p or (1 p ) = Pr( x | p ) Pr( t | p )...i.e x and t are conditionally independent given the propensity for new, p = Pr( t = 1 | x ).
 Pr( x | p ) Pr( t | x, p ) = Pr( x | p ) Pr( t | x ) = Pr( x | p ) times p or (1 p ) = Pr( x | p ) Pr( t | p )...i.e x and t are conditionally independent given the propensity for new, p = Pr( t = 1 | x ).")
10
Conditioning (patient matching) on Propensity Scores implies both… Balance: local X-covariate distributions must be the same for both treatments and Imbalance: Unequal local treatment fractions unless Pr( t | p ) = p = 1 p = 0.5
 on Propensity Scores implies both… Balance: local X-covariate distributions must be the same for both treatments and Imbalance: Unequal local treatment fractions unless Pr( t | p ) = p = 1 p = 0.5")
11
Constant PS Estimate Calipers from Discrete Choice (Logit or Probit) Model x2x2 x3x3 x1x1 x Linear Functional constant constant Infinite 3-D Slab
 Model x2x2 x3x3 x1x1 x Linear Functional constant constant Infinite 3-D Slab")
12
Pr( x, t | p ) = Pr( x | p ) Pr( t | p ) The unknown true propensity score is the most coarse possible balancing score. The known x -vector itself is the most detailed balancing score… Pr( x, t ) = Pr( x ) Pr( t | x )
 = Pr( x ) Pr( t | x ).")
13
Conditioning upon Cluster Membership is intuitively somewhere between the two PS extremes in the limit as individual clusters become numerous, small and compact… But LESS detailed than Pr( x, t ) = Pr( x ) Pr( t | x ) ? Pr( x, t | C ) = Pr( x | C ) Pr( t | x, C ) = Pr( x | C ) Pr( t | x ) for x C constant Pr( t | C ) What is LESS coarse than Pr( x, t | p ) = Pr( x | p ) Pr( t | p ) ?
 = Pr( x | C ) Pr( t | x, C ) = Pr( x | C ) Pr( t | x ) for x C constant Pr( t | C ) What is LESS coarse than Pr( x, t | p ) = Pr( x | p ) Pr( t | p ) .")
14
Unsupervised No PS Estimates Needed x2x2 x3x3 x1x1 3-D Clusters (Informative or Uninformative)
")
15
Source Degrees-of- Freedom Interpretation Clusters (Subgroups) C = Number of Clusters Local Average Treatment Effects (LATEs) are Cluster Means Treatment within Cluster Number of Informative Clusters C Local Treatment Differences (LTDs) Error Number of Patients 2C Uncertainty Although a NESTED model can be (technically) WRONG, it is sufficiently versatile to almost always be USEFUL as the number of clusters increases. Nested ANOVA

17
Source Degrees-of- Freedom Interpretation Clusters (Subgroups) C = Number of Clusters Local Average Treatment Effects (LATEs) are Cluster Means Treatment within Cluster Number of Informative Clusters C Local Treatment Differences (LTDs) Error Number of Patients 2C Uncertainty Although a NESTED model can be (technically) WRONG, it is sufficiently versatile to almost always be USEFUL as the number of clusters increases. Nested ANOVA

18
Multiplicative Shrinkage Model

19
Nested ANOVA Treatment Difference within i th Cluster: Local Treatment Imbalance!

20
i.e. not Generalized Linear Models and their Nonlinear extensions. The statistical methodology engine ideal for making fair treatment comparisons is: Cluster Analysis (Unsupervised Learning) plus Nested ANOVA
 plus Nested ANOVA.")
21
Inverse Probability Weighting (IPW) for CA models:
 for CA models:")
22
The Local Control Philosophy: y = Outcome comparisons among patients with the have most similar X characteristics are most relevant Robust, Nested Treatment-within-Cluster ANOVA Systematically form, compare, subdivide & recombine subgroups (clusters) …built-in sensitivity Non-parametric Distribution of Observed Local Treatment Differences (LTDs) …no prior distribution! Main Effect of Treatment is Mean of CDF formed by combining LTD estimates weighted Cluster Size Only when Combined CDF suggests Differential Response: Which patient characteristics predict What?

23
Credibility… Conflicts of Interest between Pharmaceutical Industry, Regulators and Data Custodians / Analysts Why should industry pay BIG $$$ for observational studies when poor / naïve analyses of biased data can create perceived needs for even more expensive RCTs?

24
FDA MC Research CRO & Academic Research Managed Care CMS & VA Pharma Industry PUBLIC The pieces dont fit together very well in the USA!

25
Aprotinin Case Study… Attack in early 2006 by a US MD who got some very sloppy analyses of international patient registry data published in NEJM Bayer (Germany) commissioned gigantic admin claims analysis by the research arm of their major US payer in mid 2006 MC researcher emailed a flawed, highly unfavorable analysis to Germany 8 days before 2006 US advisory board meeting
 commissioned gigantic admin claims analysis by the research arm of their major US payer in mid 2006 MC researcher ed a flawed, highly unfavorable analysis to Germany 8 days before 2006 US advisory board meeting")
26
Drug warnings fall flat Bayer hides bad news; a researcher doesn't, and takes heat. KRIS HUNDLEY, St. Petersburg Times, August 5, 2007 Dr. Thomas Kelly, a heart surgeon for 30 years, …routinely uses Trasylol on repeat open-heart patients or people on blood thinners. "Bleeding is a tremendous problem" Kelly said. In certain populations, there is much less need for transfusions with Trasylol. The alternatives are not nearly as effective. "This drug is used on high-risk people; that's why there's a higher incidence of death," the surgeon said. "I think a terrible disservice has been done to a very helpful drug." Though he thinks the recent studies "unfairly impugned" Trasylol, Kelly said he is using the drug more selectively and reading all the research available on the topic.

27
FDA MC Data CRO & Academic Research Managed Care CMS & VA Pharma Industry PUBLIC Why should Pharma TRUST the other Players? Unbiased Arbitration

28
What constitutes a BENEFIT ??? When a treatment is approved only for patients with high disease severity or clear vulnerability / frailty, there appear to be two possible standards. Treated patients have better outcomes than untreated patients with same risk or Treated patients have better outcomes than untreated patients with high risk

29
Bang H, Robins JM. Doubly Robust Estimation in Missing Data and Causal Inference Models. Biometrics 2005; 61: 962-972. Fraley C, Raftery AE. Model based clustering, discriminant analysis and density estimation. JASA 2002; 97: 611-631. Imbens GW, Angrist JD. Identification and Estimation of Local Average Treatment Effects. Econometrica 1994; 62: 467-475. McClellan M, McNeil BJ, Newhouse JP. Does More Intensive Treatment of Myocardial Infarction in the Elderly Reduce Mortality?: Analysis Using Instrumental Variables. JAMA 1994; 272: 859-866. McEntegart D. The Pursuit of Balance Using Stratified and Dynamic Randomization Techniques: An Overview. Drug Information Journal 2003; 37: 293-308. References

30
Obenchain RL. USPS package: Unsupervised and Supervised Propensity Scoring in R. Version 1.1-0. www.r-project.org August 2007. Obenchain RL. Unsupervised Propensity Scoring: NN and IV Plots. 2004 Proceedings of the JSM. Robins JM, Hernan MA, Brumback B. Marginal Structural Models and Causal Inference in Epidemiology. Epidemiology 2000; 11: 550-560. Rosenbaum PR, Rubin RB. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983; 70: 41-55. Rosenbaum PR. Observational Studies, Second Edition. 2002. New York: Springer-Verlag. References …concluded

Similar presentations


 Randomization:>")




>")




 Analyzing Observational Data: Focus on Propensity Scores.>")



 David Madigan Rosenbaum, P.R. (2002). Observational Studies (2 nd edition). Springer.>")


