Download presentation
Presentation is loading. Please wait.

1
Woking and Weybridge NHS Walk-in Centres: Local Evaluation 2000-2002 Dr Susan Turnbull On behalf of the University of Surrey

2
Acknowledgements (1) Ross Lawrenson John Roberts Surrey Social and Market Research, University of Surrey: Rosemarie Simmons and Elaine Bowyer
 Ross Lawrenson John Roberts Surrey Social and Market Research, University of Surrey: Rosemarie Simmons and Elaine Bowyer")
3
WICLE Steering Group Graham Browning Chris Dunstan Lou Major Sara McMullen Iain McNeil Vincent ONeill Stephen Price Pauline Rogers Cathy Winfield

4
Background: Local 39 Walk-in centres were set up as a pilot project in 2000 £31 million funding, key role in governments NHS Modernisation Programme Woking WIC opened April 2000 Weybridge WIC opened June 2000

5
Remit of WICs (1) Offer fast and convenient access to local NHS advice, information and treatment Complement, rather than compete with or replace local GP or hospital services Open 7am-10pm weekdays; 9am –10pm weekends
 Offer fast and convenient access to local NHS advice, information and treatment Complement, rather than compete with or replace local GP or hospital services Open 7am-10pm weekdays; 9am –10pm weekends")
6
Remit of WICs (2) No appointments Treatment provided by experienced NHS nurses Able to deal with minor injuries and illness, and encourage self-help Allow GPs more time to deal with patients in need of medical expertise Potential to relieve pressure on primary care/ decrease waiting times for GP appointments
 No appointments Treatment provided by experienced NHS nurses Able to deal with minor injuries and illness, and encourage self-help Allow GPs more time to deal with patients in need of medical expertise Potential to relieve pressure on primary care/ decrease waiting times for GP appointments")
7
Policy context – access to primary care NHS Plan 2000: The publics top concern about the NHS is waiting for treatment, including waiting to see a GP Target: by 2004 patients will be able to see a primary care professional within 24 hours and a GP within 48 hours

8
Policy context – access to primary care (2) Practices would be required to guarantee this level of access for their patients, either by providing the service themselves, entering into a relationship with another practice, or by the introduction of further NHS walk-in centres
 Practices would be required to guarantee this level of access for their patients, either by providing the service themselves, entering into a relationship with another practice, or by the introduction of further NHS walk-in centres")
9
NHS Priorities and Planning Framework 2002/3 2 must-dos relevant to WIC aims: Improving emergency services in terms of their availability, quality, comprehensiveness and speed Reducing waiting throughout the system and in particular for consultations in primary care and hospital and admissions to hospital PPF also emphasises need to address inequalities in access to services

10
Primary care access: pressures (Audit Commission 2002: General Practice in England) 1/3 of GPs and practice nurses >50 Increasing consumer expectations Ageing population Exacting national standards / quality/ monitoring Greater scrutiny Shifting of workload from secondary to primary care More GPs part-time Increasingly complex care GPSIs – less time for general practice Other commitments outside the practice eg PCT
 1/3 of GPs and practice nurses >50 Increasing consumer expectations Ageing population Exacting national standards / quality/ monitoring Greater scrutiny Shifting of workload from secondary to primary care More GPs part-time Increasingly complex care GPSIs – less time for general practice Other commitments outside the practice eg PCT")
11
National Evaluation Commissioned as part of the WICs pilot University of Bristol on behalf of the Department of Health Published 2002 Each WIC submitted quarterly monitoring returns including activity and costings data

12
Local evaluations DH funding to each WIC for local evaluation Bournewood Community and Mental Health NHST managed both WICs: commissioned University of Surrey to evaluate both

13
Location

14
Study objective To evaluate the impact of Woking and Weybridge NHS walk-in centres on improving access to health care Combined quantitative and qualitative approach

15
Framework: Maxwells 6 dimensions of healthcare quality Access Equity Effectiveness Appropriateness Acceptability Efficiency

16
Quantitative analysis (1) Database anonymised – year of birth and ward of residence only Study period 9 October 2000 – 19 August 2001 – longest period when both WICs fully computerised + using same system (Interhealth)
 Database anonymised – year of birth and ward of residence only Study period 9 October 2000 – 19 August 2001 – longest period when both WICs fully computerised + using same system (Interhealth)")
17
Quantitative analysis (2) Initial visits rather than all visits – to avoid consideration of recurrent or review attendances for same condition Initial visits : 24117 Woking 9020 Weybridge
 Initial visits rather than all visits – to avoid consideration of recurrent or review attendances for same condition Initial visits : Woking 9020 Weybridge")
18
Sex: Woking Females 53.2%

19
Sex: Weybridge Females: 55.8%

20
Visits by age and sex

22
Time: trends in visit numbers

23
Proportion of visits by day attended

24
Time of day: weekday vs. weekend

25
Time attended, location and sex

28
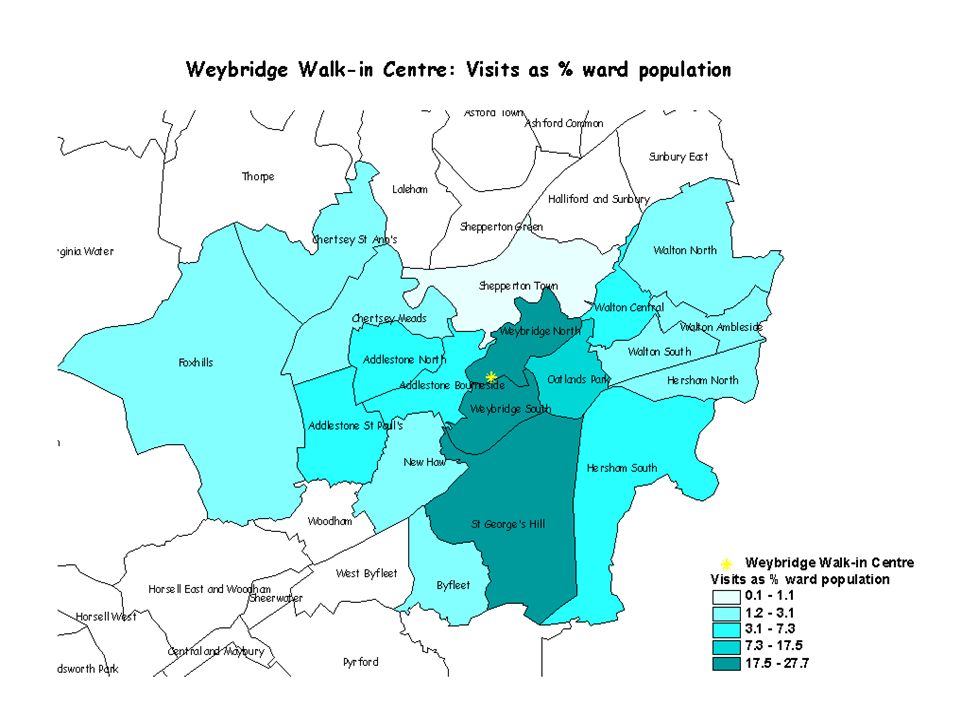
Ward of residence Most visits from residents of closest wards Woking: Visits equivalent over a ¼ of these wards: Kingfield & Westfield (33.7%) Mount Hermon West (31.7%) Mount Hermon East (28.8%) Old Woking (28.3%) Weybridge: Weybridge North (27.7%) St Georges Hill (27.1%)
 Mount Hermon West (31.7%) Mount Hermon East (28.8%) Old Woking (28.3%) Weybridge: Weybridge North (27.7%) St Georges Hill (27.1%)")
35
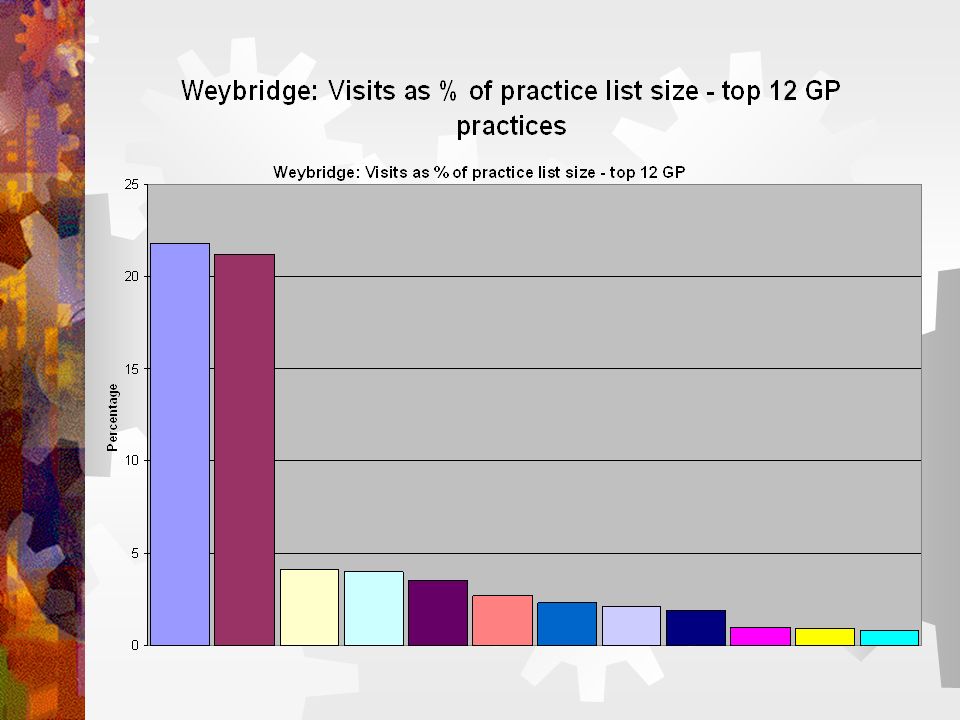
Access and equity Gender pattern of attendance similar to general practice F>M. Opposite re A&E M>F 25-44 year olds most frequent attenders – but also largest age group Older people attending in numbers appropriate to population proportion (Woking – even higher) Most WIC visits not out of hours Visits gradually increased Highest proportion of visitors live nearby and/or are registered with GP practice close to WIC
 Most WIC visits not out of hours Visits gradually increased Highest proportion of visitors live nearby and/or are registered with GP practice close to WIC.")
36
Proportion of visits by diagnosis (1)
")
37
Proportion of visits by treatment (1)
")
38
Proportion of visits by discharge recommendation

39
Appropriateness Disappointing proportion of missing data Commonest diagnoses: Soft tissue injury Woking; ENT Weybridge Commonest treatment: advice and reassurance Woking: 83.5% with A&R as treatment (1) had no treatment (2) recorded. Weybridge: 90.1%

40
Effectiveness Estimates of impact based on visitors reported alternative in the absence of a WIC Caution about desirable responses – ? bias against self-care as alternative to justify decision to seek professional advice

41
Proportion of visits by alternative if no WIC available

42
Alternative Disappointing proportion of missing data Very small proportion where alternative = self care, especially Woking Woking males – almost equal re GP and A&E Weybridge females: >3x as many GP as A&E alternative GP alternative most frequent both WICs

43
Alternative = GP by discharge

44
Alternative=A&E by discharge

45
Alternative= self care by discharge

46
Acceptability Quantitative analysis did not address acceptability Growing attendance suggests acceptability User survey at Woking WIC July 2000: (Rogers,P. Case study of one walk-in centre pilot site. University of Surrey. Dissertation for MSc in Health Care Management)
.")
47
Efficiency Qualitative study did not address efficiency Cost per visit calculated using same criteria as national evaluation: all running costs (no set up costs); all visits
; all visits")
48
Efficiency (2) Woking: Running costs quarter ended 31/03/01: £ 159k Estimated all visits: 8353 Estimated cost per visit £19 Weybridge: Running costs quarter ended 31/03/01: £156k Estimated all visits: 2644 Estimated cost per visit £59
 Woking: Running costs quarter ended 31/03/01: £ 159k Estimated all visits: 8353 Estimated cost per visit £19 Weybridge: Running costs quarter ended 31/03/01: £156k Estimated all visits: 2644 Estimated cost per visit £59")
49
Efficiency (3) Higher cost per visit Weybridge: similar running costs, visit rate much lower in study period Recent enquiry: Weybridge activity increased by > 3-fold. Cost per visit for Oct 2001 – Aug 2002: £15.36 Reinforces moving picture National evaluation – comparable cost per visit £31.11 Average cost of visit to a GP £15; practice nurse £9

50
Qualitative study (1) Surrey Social and Market Research (SSMR), Department of Sociology, UniS Aim – assess impact on other local health services providers: GPs, receptionists, practice nurses) GPs re OOH perspective Staff of nearest A&E Surrey Ambulance Service personnel WIC personnel Total 30 interviews January 2002
 Surrey Social and Market Research (SSMR), Department of Sociology, UniS Aim – assess impact on other local health services providers: GPs, receptionists, practice nurses) GPs re OOH perspective Staff of nearest A&E Surrey Ambulance Service personnel WIC personnel Total 30 interviews January 2002")
51
Qualitative study: access & equity Access probably be limited by distance Use may be limited by lack of awareness Need for publicity: services provided, and exclusions WICs probably unpopular with older people Noticeable use of Woking WIC by Woking Asian community (largest in Surrey)
")
52
Qualitative study: appropriateness Most agreed WICs dealt with appropriate minor conditions GPs felt WIC staff erred on side of caution Some A&E, WIC and ambulance staff considered WIC eligibility criteria too rigid WIC staff keen to have feedback on how they are doing WIC staff – the presence of the WIC may be encouraging some unnecessary visits A GP: it may muddy the distinction between what is an emergency and what can wait

53
Qualitative study: effectiveness GPs had noticed little if any impact on workload Most GPs felt referrals to them from the WICs were appropriate Main impact on A&E department staff was loss of experienced colleagues Most considered WICs had not generated new work for others

54
Qualitative study: acceptability GPs: expectations mixed but experiences generally favourable Most felt patients confident about advice from WIC Very positive feedback from some patients WIC staff: conflict generated by walk-in name implying no/minimum waiting Ambulance staff: noted patients preferred faster WIC turnaround times cf. A&E. Better if WICs open 24 hours – patient refused after 9pm re 10 pm closure

55
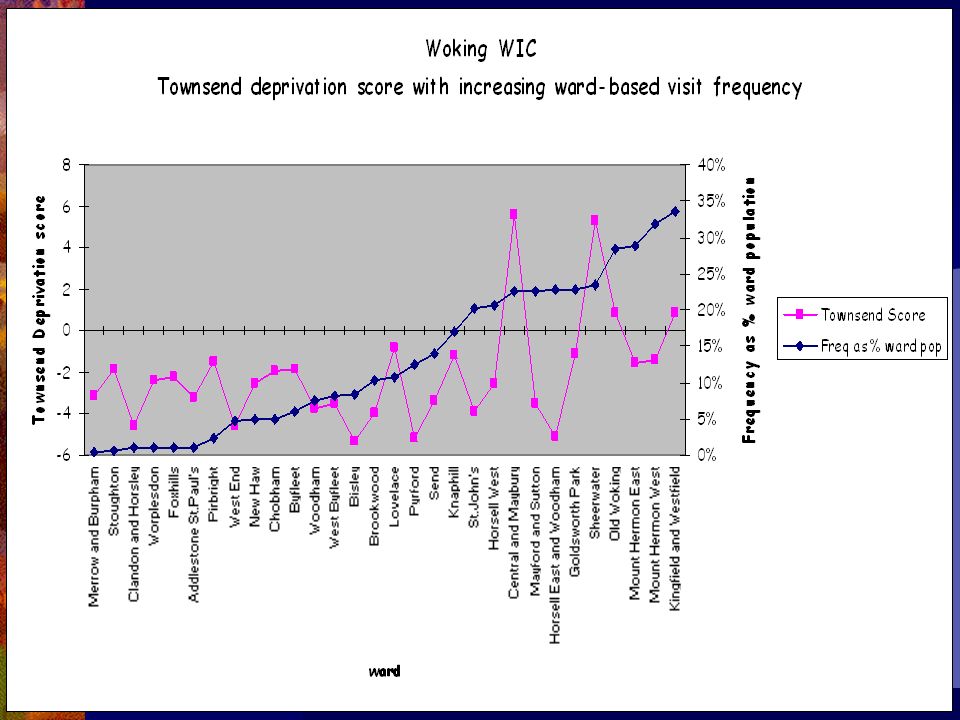
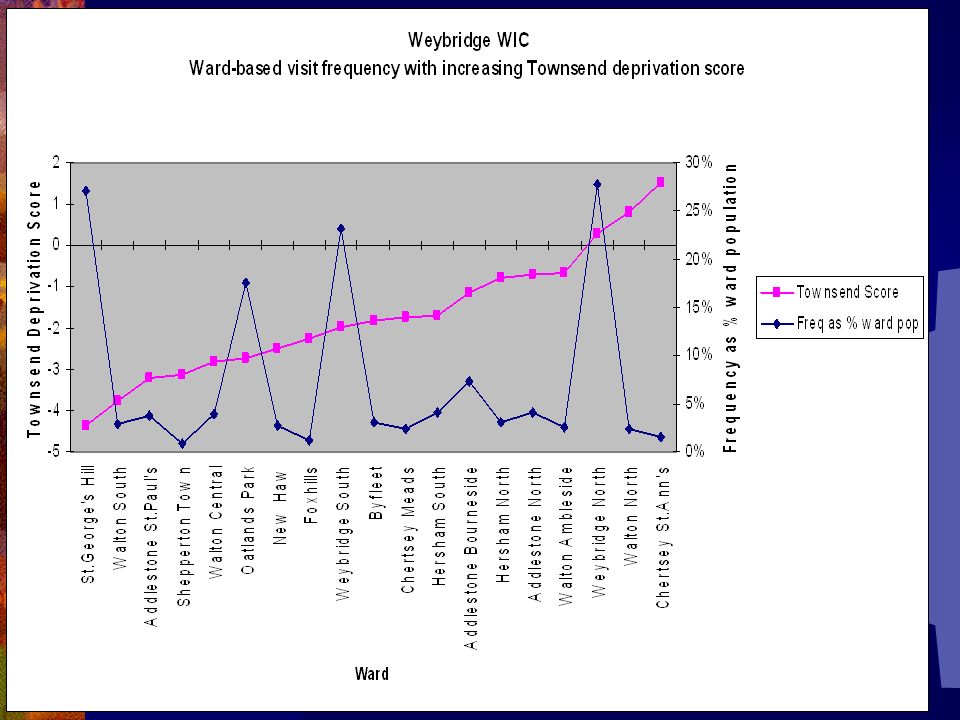
Summary: key points – quantitative (1) Main determinant of WIC use is proximity to home, or GP practice where registered Apparent correlation between increasing visits to Woking WIC, and Townsend deprivation category Most visitors: Were managed in the WIC and discharged home Received only advice and reassurance GP was the most frequently reported alternative
 Main determinant of WIC use is proximity to home, or GP practice where registered Apparent correlation between increasing visits to Woking WIC, and Townsend deprivation category Most visitors: Were managed in the WIC and discharged home Received only advice and reassurance GP was the most frequently reported alternative")
56
Summary: key points – quantitative (2) WICs appear to have diverted substantial numbers away from original intention – estimated 874/ month from GPs GPs whose practices are closest appear to have benefited most. No evidence of WIC-generated extra demand for GP or A&E attention Woking WIC inclined to review more in WIC; Weybridge referred higher proportion to own GP

57
National Evaluation of NHS WICs (Salisbury,C. et. al, University of Bristol, July 2002) Access improved for young and middle aged men who are relatively low GP users WIC users more likely to be young adult, white owner-occupiers educated beyond age 18 This may increase health inequalities Users highly satisfied Low rate of referrals elsewhere suggests most WIC consultations were appropriate
 Access improved for young and middle aged men who are relatively low GP users WIC users more likely to be young adult, white owner-occupiers educated beyond age 18 This may increase health inequalities Users highly satisfied Low rate of referrals elsewhere suggests most WIC consultations were appropriate.")
58
National evaluation (2) Impact of a WIC a drop in the ocean re number of consultations compared with GPs/A&E nearby Possible total NHS workload may have increased as result of the WIC initiative Little evidence of duplication of care Cost per visit higher (£31 average) than GP consultation (£15) Safe, quality care but at extra cost Benefits and costs must be weighed against competing claims for NHS resources
 Impact of a WIC a drop in the ocean re number of consultations compared with GPs/A&E nearby Possible total NHS workload may have increased as result of the WIC initiative Little evidence of duplication of care Cost per visit higher (£31 average) than GP consultation (£15) Safe, quality care but at extra cost Benefits and costs must be weighed against competing claims for NHS resources")
59
Comparison and Conclusions Aggregated national analysis is not informative about local variations National evaluation did not use deprivation indices Local evaluation shows key determinant of WIC is proximity of home, or GP practice where registered Potential to address health inequalities - targeted, strategic siting of WICs near populations whose needs are greatest

60
Conclusions Woking cost per visit at time of evaluation compared well with national average, and GP cost Weybridge didnt – but does now Stresses moving picture and importance of avoiding a rush to judgement But when visitor numbers treble – increased waiting, less accessibility/ acceptability, possibly reduced effectiveness working under pressure Trade-off between Maxwells dimensions

61
Unanswered questions Could WICs be generating new, previously unexpressed demand? How much duplication is there? How much are WICs promoting self-care, or inadvertently encouraging the worried well to seek professional advice? How can the impact of WICs on demand for other services be disentangled from those of NHS Direct

62
Future developments Keeping the NHS local: A new direction of travel (DH January 2003) Ambulatory care plus - models of care that build on existing primary and community services, such as walk-in centres, advanced access surgeries and community hospitals. Similar to US Kaiser Permanente approach to primary care: large team including specialist/ generalist doctors; physician assistants and nurse practitioners with own lists Facilities open evenings and weekends. On site labs, x-ray, pharmacy………………………..

Similar presentations