Download presentation
Presentation is loading. Please wait.

1
Dosing Regimen Individualization Age

2
Subcategories Newborn1-7 d Neonate8 d – 2 mo Infant2 mo – 1 yr Child1 – 12 yr Adolescent12 – 20 yr Adult20 – 70 yr Elder> 70 yr Age of usual adult for whom the “usual adult regimen” is prescribed is 55 years.

3
Confounding variables Influence of age on pharmacokinetics is difficult to separate from the influence of body weight in the young, and from disease in adults.

4
Cross-sectional vs. Longitudinal Study Designs Cross-sectional design: group subjects by age and compare PK parameter values in the different age groups: AgeCL 10-20aaa.a 21-30bbb.b 31-40ccc.c Longitudinal design: Repeatedly measure PK value in the same subjects over a long period of time.

5
Pitfall with cross-sectional design An apparent age-associated effect may be due to differences in longevity that also influence the PK parameter. Example: Effect of age on eye color. Assume the people with blue eyes also have a relatively short life span, but this is unknown at the time of the study. A cross-sectional study would indicate that the fraction of people with blue eyes declined with increasing age. A longitudinal study would show the truth, that people with blue eyes did not live as long. Conclusion: eye color changes with increasing age.

6
V and age: protein binding f up tends to be elevated in newborns and in the elderly. V values tend to be elevated for protein-bound drugs. Grandison and Boudinot. Age-related changes in protein binding of drugs. Clin. Pharamacok. 38:271-290,2000. Review of literature for f up values measured in young and elderly subjects/patients found 106 studies for 66 drugs. 28/106 studies showed f up elevated in the elderly 7/106 studies showed f up decreased in the elderly 71/106 studies showed no change for f up in the elderly Age-related changes [in adults] are usually not clinically important – Grandison and Boudinot.

7
, male; o, female. B. Th. Veering, et al. Br. J. clin. Pharmac. 29:201-206, 1990. Plasma Proteins

8
V and age: protein binding AgeN K d [mg/L] n[P] [mg/L] f up 1 – 8 d1526.91350.30 7 – 15 m40.16 2 – 6 yr50.16 22-25 yr814.13270.058 40 – 49 yr415.42790.076 81 – 88 yr316.42170.113 Hayton and Stoeckel. Age associated changes in ceftriaxone pharmacokinetics. Clin. Pharamacok. 11:76-86,1986. Ceftriaxone
![V and age: protein binding AgeN K d [mg/L] n[P] [mg/L] f up 1 – 8 d – 15 m – 6 yr yr – 49 yr – 88 yr Hayton and Stoeckel.](http://images.slideplayer.com/24/7357254/slides/slide_8.jpg "Age associated changes in ceftriaxone pharmacokinetics. Clin. Pharamacok. 11:76-86,1986. Ceftriaxone.")
9
Adiposity: increases as adults age ~20% Body Weight in young adults Age and Gender Dependent: Children age 15 yr and below BF% = 1.51BMI – 0.70age –3.6Gen + 1.4 Adults BF% = 1.2BMI + 0.23age –10.8Gen - 5.4 BMI = body mass index = BW/H 2 (kg/m 2 )
")
10
V and age: ceftriaxone AgeN V [L/kg] V [L/m 2 ] 1 – 8 d240.5046.57 9 – 30 d100.6509.21 1 – 12 m110.5389.64 1 – 6 yr80.3398.53 18 – 49 yr500.1576.03 50 – 74 yr90.1515.79 75 – 92 yr110.1465.16
![V and age: ceftriaxone AgeN V [L/kg] V [L/m 2 ] 1 – 8 d – 30 d – 12 m – 6 yr – 49 yr – 74 yr – 92 yr](http://images.slideplayer.com/24/7357254/slides/slide_10.jpg "V and age: ceftriaxone AgeN V [L/kg] V [L/m 2 ] 1 – 8 d – 30 d – 12 m – 6 yr – 49 yr – 74 yr – 92 yr")
11
Obesity and V Values log P = log [octanol / pH 7.4 buffer] partition coefficient
![Obesity and V Values log P = log [octanol / pH 7.4 buffer] partition coefficient](http://images.slideplayer.com/24/7357254/slides/slide_11.jpg "Obesity and V Values log P = log [octanol / pH 7.4 buffer] partition coefficient")
12
log V vs. log P

13
-Blockers and Obesity: V log V = 0.23( 0.04)log D + 2.1( 0.07)log V = 0.25( 0.05)log D + 2.2( 0.07) control obese G. Cheymol. Effects of obesity on pharmacokinetics. Clinical Pharmacokinetics 39:215-231,2000.

14
Obesity and V General lack of correlation between V and log P is attributed in part to variability in the affinity of drug for lean tissue. affinity for lean tissue is unrelated to log P and highly variable among drugs. amine functional group seems to increase affinity for lean tissue. The difference between actual and ideal body weight in obesity is not all adipose tissue; 20-40% of the additional weight is lean.

15
CL and age: CL R 11,347 CL CR values from 5,146 subjects Hallynck T, Soep H, Thomis J, Boelaert J, Daneels R, Dettli L: Should Clearance be Normalised to Body Surface or to Lean Body Mass? Br. J. Pharmac. 11:523-526, 1981. CL CR = [140 – age] W / 70

16
CL CR – longitudinal study, adults Lindeman, et al. J. Amer. Geriatrics Soc. 33:278,1985. Baltimore longitudinal study of aging. 254 normal subjects; not taking diuretics or antihypertensives, and no renal or urinary tract disease. One-third had no decrease in renal function over time.

17
CL and age: CL H Rowland and Tozer. Fig. 15.9, p. 239. n = 307 oxidative metabolism - 1% / yr

18
CL R and age: children Hayton, Stoeckel, et al. Antimicrob. Agents Chemother. 35:720-725, 1991; 40:567-574, 1996. cefetamet b = 0.661

19
CL R cefetamet: age-weight model age CL R CL R,im CL R,ma

20
Age-Weight Model

21
The least-squares fit of this equation to cefetamet CL values in children is indicated by the solid circles.

22
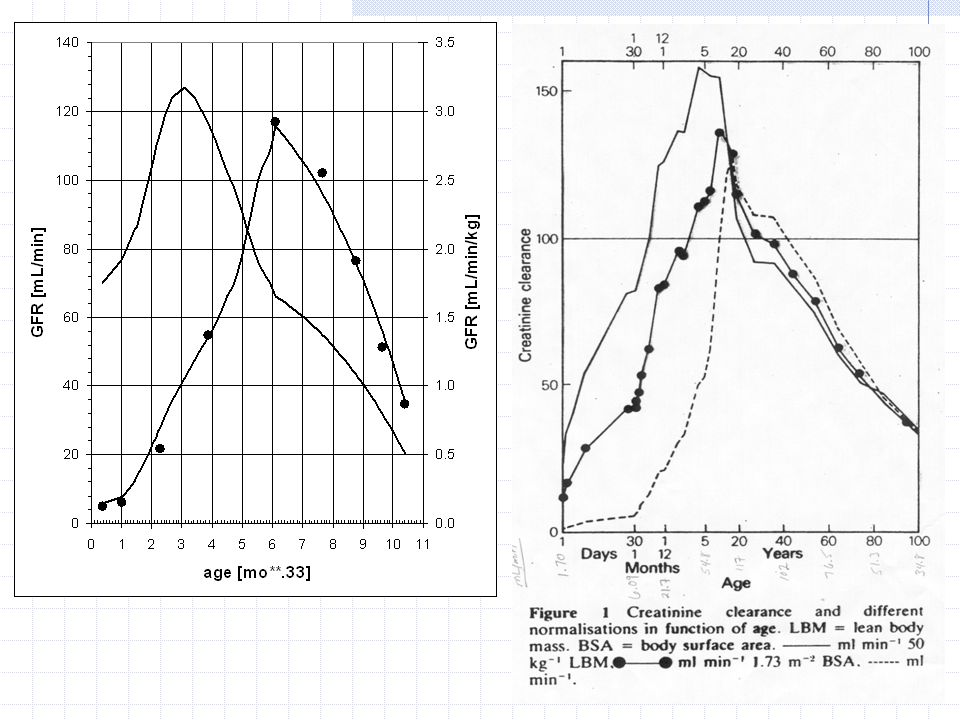
GFR: maturation and growth 63 healthy children age 2 d to 12 yr a [mL/min] 2.60 b0.662 c [mL/min] 8.14 k mat mo -1 0.0882 (t 1/2 ) mat mo 7.9
![GFR: maturation and growth 63 healthy children age 2 d to 12 yr a [mL/min] 2.60 b0.662 c [mL/min] 8.14 k mat mo (t 1/2 ) mat mo 7.9](http://images.slideplayer.com/24/7357254/slides/slide_22.jpg "GFR: maturation and growth 63 healthy children age 2 d to 12 yr a [mL/min] 2.60 b0.662 c [mL/min] 8.14 k mat mo (t 1/2 ) mat mo 7.9")
23
GFR: maturation and growth From the maturation half life, children age 2 yr and older have fully mature renal function. DR need be adjusted only for body weight. The body weight adjustment should use the b value of 0.662; i.e., a body surface area adjustment is appropriate.

24
GFR: maturation and growth For children less than 2 yr of age, adjustment of the adult dosage must include adjustment for immaturity as well as for body size. 1. Divide through by W; this results in CL R per kg W. 2. Divide through by 1.43 mL min -1 kg -1 (adult GFR of 100 mL/min per 70 kg). This results in the fraction of the adult normal GFR for a child of weight W and age in months.
. This results in the fraction of the adult normal GFR for a child of weight W and age in months..")
25
GFR: maturation and growth For a child less than 2 yr and a drug cleared primarily by the kidneys, 1) calculate FRAC GFR : 2) Calculate the dosing rate as a fraction of the adult dosing rate:
 calculate FRAC GFR : 2) Calculate the dosing rate as a fraction of the adult dosing rate:")
26
Example The usual adult dosage for this antibiotic is 250 mg t.i.d. What should the regimen be for a 4 mo. old, 12 lb infant? FRAC GFR = 5.44 -0.338 (5.69 – 3.87e -0.0882(4) ) = 1.68 D M,infant = D M,adult x FRAC GFR = (250 mg / 70 kg)(1.68) = 6.00 mg/kg D M,infant = 6.00 mg/kg x 5.44 kg = 32.6 mg t.i.d.
 ) = 1.68 D M,infant = D M,adult x FRAC GFR = (250 mg / 70 kg)(1.68) = 6.00 mg/kg D M,infant = 6.00 mg/kg x 5.44 kg = 32.6 mg t.i.d..")
27
Features of the age,weight model 1.Degree of maturation is indicated by the ratio of c / a 8.14 / 2.60 = 3.1 2. The time for maturation was characterized by the maturation half life; 3.3 t 1/2,mat was about 2 yr. 3. The body weight exponent was 0.662, which suggests that BSA is the appropriate index for adjustment of the adult DR for children 2 yr of age and older.

28
Features, cont. 4. GFR per kg body weight is influenced positively by maturation and negatively by growth, over two time frames. usual adult value

29
GFR from birth to 100 yr GFR = (140 - age) W / 70 GFR (mL/min) = 2.60W 0.662 e -0.0882age + 8.14W 0.662 (1 - e -0.0882age ) – (age/12)(W/70) 0.662 age, mo.; W, kg
 W / 70 GFR (mL/min) = 2.60W e age W (1 - e age ) – (age/12)(W/70) age, mo.; W, kg")
31
CL H and age: children S.N. de Wildt, et al., Cytochrome P450 3A ontogeny amd drug disposition. Clin. Pharmacok. 37:485-505,1999.

33
Liver Volume and Drug CL vs. Age in Children Murry, Crom, … Evans. Drug Metab. Disp. 23:1110-1116, 1995 8 boys/8 girlsmedianrange Age [yr]9.73.3-18.8 Weight [kg]40.811.9-88.5 BSA [m 2 ]1.370.57-2.0 Liver Vol. [mL]973469-1640

34
lorazepam eliminated primarily by glucuronidation p > 0.05 Murry, Crom, … Evans. Drug Metab. Disp. 23:1110-1116, 1995

35
antipyrine eliminated primarily by CYP450- mediated oxidation p > 0.05 p < 0.05 Murry, Crom, … Evans. Drug Metab. Disp. 23:1110-1116, 1995

36
Indocyanine Green clearance. CL is by the liver and E 1. CL ICG is widely used as a measure of hepatic blood flow.

Similar presentations




 if given parenterally, they should.>")










 Department of Pharmaceutics BLUE BIRDS COLLEGE OF PHARMACY (Affiliated to.>")




