Download presentation
Presentation is loading. Please wait.

1
Presented by: Meme Phung Zhi Yuan Quek Alison Wong

2
Acute Diabetes Jill, aged 30 years, has recently experienced hypoglycaemic episodes. She has experienced weakness & dizziness periodically for the last 5 years and a seizure 2 years previously. She does not have a history of drug abuse or organ dysfunction. A fasting plasma glucose was 3.7 mmol/L, with no accompanying symptoms. An insulinoma is suspected.

3
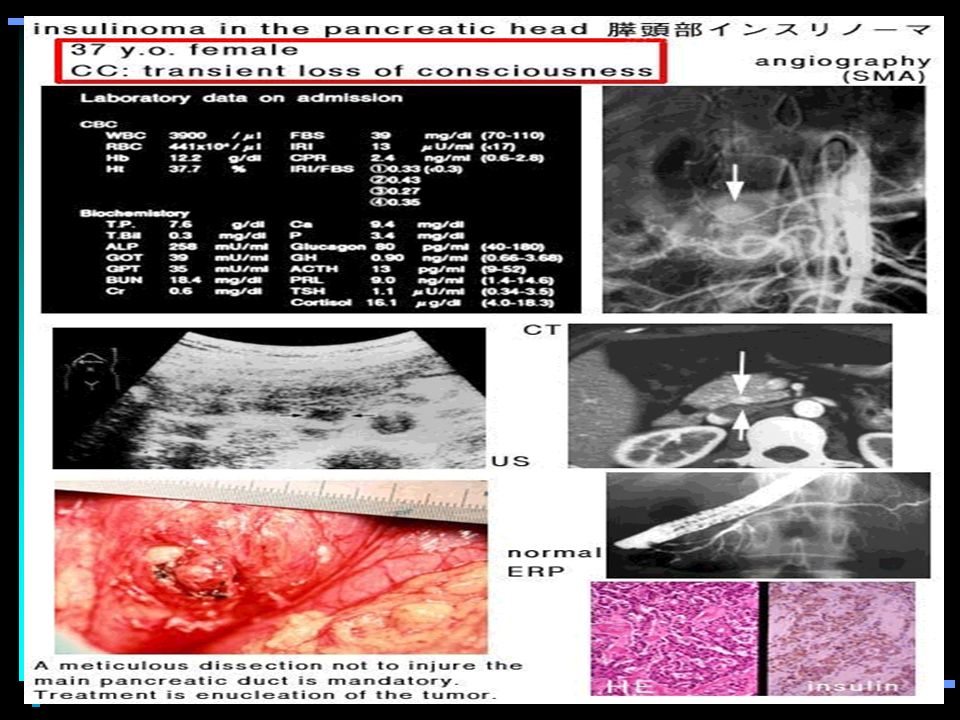
What is insulinoma? A rare form of tumour of the islets of Langerhans in the pancreas Commonly derived from beta cells Produce excessive amounts of insulin 80% are benign, small, single 10% are malignant (metastasis are present) 10% are multiple (MEN 1 hereditary disease)
 10% are multiple (MEN 1 hereditary disease).")
4
CT scan

6
Symptoms Due to excessive or inapproriate insulin and proinsulin secretion hypoglycaemia occurs such as: Diplopia, blurred vision, palpitations, confusion and abnormal behaviour. Episodic unconsciousness Grand-mal seizures

7
Symptoms May be present from 1 week - several decades prior to diagnosis Occur during fasting or after alcohol or exercise and treatment with sulphonylureas Weight gain

8
Signs and Diagnosis Signs Low blood glucose High serum insulin High c-peptide level Diagnosis is based on : Inappropriate hyperinsulinaemia High ratio of proinsulin to insulin in a fasting blood sample CT scanning and/or pancreatic arteriography to identify the site of the lesion

9
Inappropriate hyperinsulinaemia Frequently have increased proinsulin concentrations and an insulin:proinsulin ratio closer to 1:1 Normal individuals have a 6:1 ratio

10
Management Medical treatment with: Diazoxide Hydrochlorothiazide Octreotide acetate Surgery !

11
Insulin - polypeptide hormone - islets of Langerhans

12
Pro-insulin - precursor molecule - split into two molecules in equimolar amounts insulin (physiologically active) C-peptide (physiologically inactive)
 C-peptide (physiologically inactive)")
13
HOW ARE INSULIN LEVELS MEASURED? IMMUNOASSAYS 1.Radioimmunoassay (RIA) - non-specific polyclonal antisera cross-reactivity 38% to 100%
 - non-specific polyclonal antisera cross-reactivity 38% to 100%.")
14
- specific monoclonal antibodies competitive - unlabelled insulin and 125 I-labelled insulin - fixed amount of tracer and antibody - amount of tracer inversely proportional to concentration of unlabelled ligand

15
non-competitive - excess of antibodies immobilized on surface of matrix - insulin in serum captured - detected by labelled secondary antibody

17
2. Enzyme-linked Immunosorbent Assay (ELISA) - non-isotopic - competitive and non-competitive - horseradish peroxidase - spectrophotometry measurement - enzyme activity directly proportional to captured human insulin
 - non-isotopic - competitive and non-competitive - horseradish peroxidase - spectrophotometry measurement - enzyme activity directly proportional to captured human insulin.")
18
INTERFERENCES Issue of specificity - cross-reactivity of insulin precursors Anti-insulin antibodies - interfere with results of immunoassays - overestimation or underestimation

20
Why do we measure C-peptide? 1.Diagnosis of insulin-induced factitious hypoglycemia 2.Contribution of the diagnosis of insulinoma (insulin suppression test) 3.Assessment of residual beta-cell function in diabetes under insulin therapy 4.Adjunct in the differential diagnosis between type 1 (insulin dependent) and type 2 (non insulin dependent) diabetes 5.Evaluation of insulin secretion in liver disease
 3.Assessment of residual beta-cell function in diabetes under insulin therapy 4.Adjunct in the differential diagnosis between type 1 (insulin dependent) and type 2 (non insulin dependent) diabetes 5.Evaluation of insulin secretion in liver disease.")
21
1. Diagnosis of insulin-induced factitious hypoglycemia Elevation in insulin may be the result of excessive insulin administration Commercial insulin preparations do not contain C-peptide. You’ll expect the C-peptide levels to be low, if it is exogenous insulin administration (factitious hypoglycemia).
..")
22
2. Contribution of the diagnosis of insulinoma (insulin suppression test) If both C-peptide and insulin (which are released in equimolar amounts) are elevated… suspect insulinoma?
 If both C-peptide and insulin (which are released in equimolar amounts) are elevated… suspect insulinoma .")
23
3. Assessment of residual beta- cell function in diabetes under insulin therapy When endogenous insulin cannot be measured. Patients who receive exogenous insulin treatment anti-insulin antibodies interfere with the RIA for insulin C-peptide measurement will provide an estimate of the patient’s own remaining insulin-secretory capacity and may help in distinction between type 1 and type 2 diabetes.

24
4.Adjunct in the differential diagnosis between type 1 and type 2 diabetes C-peptide and insulin are secreted in equimolar amounts: C-peptide levels can serve as a valuable index to insulin secretion. Low C-peptide levels are expected where insulin secretion is diminished (insulin dependent diabetes)
.")
25
Insulin Suppression Test Used for the diagnosis for insulinoma.

26
PRINCIPLE OF TEST In the absence of fasting hypoglycaemia, insulin administration will result in a suppression of endogenous insulin production. C-peptide levels will also be suppressed as a normal response to exogenous insulin

27
METHOD 72-hour fasting test Insulin to be administered to patients/subjects to check for insulin suppressibility. Blood samples are taken 30,60,90 and 120 minutes after the insulin dose. Lab results for blood glucose, insulin and C- peptide.

28
RESULTS Normal subject: C-peptide usually suppresses to <1.5ug/L and may be undetectable 30-60min after hypoglycemia has been achieved, with insulin being <10mU/L. Insulinoma: C-peptide is not suppressed by insulin administration. Both insulin and C-peptide levels will be elevated Insulin >10mU/L, despite low blood glucose of <2.2mmol/L

29
Jill was hospitalised and an extended fast was conducted yielding the following results: The c-peptide value at 48 hours was 5 ug/L (0.8-1.9ug/L). 12h24h36h48hRange Glucose mmol/L 3.33.12.72.13.6-5.8 Insulin mU/L 81217354-10

30
Lab results conducted over a 48-hour period Glucose levels very low (hypoglycemia), outside the reference interval Insulin levels increases to very high, of 35mU/L (outside the reference interval), C-peptide value also raised. Results support diagnosis of insulinoma Further tests (e.g. detailed CT scan, MRI, octreotide scan, and an endoscopic ultrasound) need to be performed to detect for the tumour in the pancreas.
 need to be performed to detect for the tumour in the pancreas..")
Similar presentations





>")






>")
. 2 Hypoglycaemia Learning outcomes >Can state what hypoglycaemia is >Be able to assess who is at risk of hypoglycaemia.>")


 is a very important fuel source to generate universal energy molecules (ATP). Blood glucose regulation I->")



