Download presentation
Presentation is loading. Please wait.

1
MAKATI MEDICAL CENTER DEPARTMENT OF MEDICINE MEDICAL GRANDROUNDS
Ma. Melmar S. Anicoche, M.D. April 29, 2010

2
Objectives To discuss the effect of Chronic Kidney Disease (CKD) on calcium-phosphorus metabolism. To discuss biochemical complications after parathyroidectomy.

3
Patient Profile L.G. , 61/F, from Binan, Laguna DOA: February 12, 2010
Chief complaint: Persistently elevated PTH

4
History of Present Illness
Patient is a diagnosed case of End stage Renal Disease since 2000, on hemodialysis since 2001, three times a week. 2 years PTA 1 year PTA Bone pains, weakness, intermittent abdominal pain iPTH: (15-65pg/ml) Normal calcium, elevated phosphorus Impression: tertiary hyperparathyroidism iPTH: 1,528 pg/ml Admission
 Normal calcium, elevated phosphorus. Impression: tertiary hyperparathyroidism. iPTH: 1,528 pg/ml. Admission.")
5
Personal & Social History:
Review of Systems: (-) weight loss, headache, fever, vomiting, chest pain, bowel movement irregularities Past Medical History: s/p Bilateral Ureterolithotomy – 1995 s/p Nephrectomy,left – 1998 s/p ESWL, right – 2000 s/p CVA – 2000 & 2007 Family History: (+) Urolithiasis – parents & siblings Personal & Social History: Nonsmoker Nonalcoholic beverage drinker
 weight loss, headache, fever, vomiting, chest pain, bowel movement irregularities. Past Medical History: s/p Bilateral Ureterolithotomy – s/p Nephrectomy,left – s/p ESWL, right – s/p CVA – 2000 & Family History: (+) Urolithiasis – parents & siblings. Personal & Social History: Nonsmoker. Nonalcoholic beverage drinker.")
6
BP: 140/70 CR 74 bpm, regular RR 20 cpm T 36.5°C
Warm moist skin, no active dermatoses Pink palpebral conjunctivae, anicteric sclerae Supple neck, no palpable lymph nodes, thyroid not enlarged, no masses Symmetric chest expansion, no retractions, clear breath sounds ,AB at 5th LICS MCL, S1 louder than S2 at the apex, S2 louder than S1 at the base, no murmurs Flabby abdomen (+) 9cm incisional scar on left lower quadrant, (+) 6 cm incisional scar on right lower quadrant, NABS, soft, nontender, no organomegaly Full and equal pulses, No cyanosis & edema of extremities MMT: 5/5 on left lower extremity & both upper & lower extremities, 3/5 left upper extremity; slight limitation of motion on all extremities 6
 9cm incisional scar on left lower quadrant, (+) 6 cm incisional scar on right lower quadrant, NABS, soft, nontender, no organomegaly. Full and equal pulses, No cyanosis & edema of extremities. MMT: 5/5 on left lower extremity & both upper & lower extremities, 3/5 left upper extremity; slight limitation of motion on all extremities. 6.")
7
Salient Features 61/F Known case of End Stage Renal Disease for 10 years, on hemodialysis Bone pains, weakness and abdominal pain Elevated iPTH & phosphorus, normal calcium

8
Impression: Tertiary Hyperparathyroidism

9
Feedback Mechanisms Restoring Calcium Levels to Normal
Serum PTH levels are tightly regulated by a negative feedback loop, and closely regulated by the concentration of serum ionized calcium. A decrease in extracellular calcium triggers an increase in PTH secretion (1) via activation of the calcium sensor receptor on parathyroid cells. PTH, in turn, results in tubular reabsorption of calcium by the kidney, (2) and resorption of calcium from bone (2) and also stimulates renal 1,25 (OH)2D production (3) 1.25 (OH)2D, in turn, acts principally on the intestine to increase calcium absorption (4) Collectively, these homeostatic mechanisms serve to restore serum calcium levels to normal.
 via activation of the calcium sensor receptor on parathyroid cells. PTH, in turn, results in tubular reabsorption of calcium by the kidney, (2) and resorption of calcium from bone (2) and also stimulates renal 1,25 (OH)2D production (3) 1.25 (OH)2D, in turn, acts principally on the intestine to increase calcium absorption (4) Collectively, these homeostatic mechanisms serve to restore serum calcium levels to normal.")
10
Disturbances in mineral & bone metabolism are common in patients with chronic kidney disease. Phosphate retention, which may develop with loss of kidney function, interferes with the ability of patients with CKD to augment the production of 1,25 (OH)2D3 by the kidneys to meet the increased need for this metabolite. Thus, a state of absolute or relative vitamin D deficiency develops, leading to defective intestinal absorption of calcium and impaired calcemic response to PTH. These 2 abnormalities produce hypocalcemia which in turn causes secondary hyperparathyroidism. Hypocalcemia and phosphate retention or hyperphosphatemia are the most important factors responsible for the hyperplasia of the parathyroid glands. Because hypocalcemia may develop early in the course of CKD, hyperactivity of the parathyroid glands is also encountered in the early stages of kidney disease. Indeed, elevated blood levels of PTH may be noted when the GFR falls below 60 mL/min/1.73 m2. K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease

11
Frequency of Measurement of iPTH, Ca & Phos
CKD Stage GFR Range iPTH Ca & Phos 3 30 – 59 Every 12 months 4 15 – 29 Every 3 months 5 <15 or dialysis Every month K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease

12
Target Range of iPTH, Ca & Phos
CKD Stage iPTH (pg/ml) Ca (mg/dl) Phos (mg/dl) 3 35 – 70 8.6 – 10.2 2.7 – 4.6 4 70 – 110 5 8.4 – 9.5 3.5 – 5.5 K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease
 Ca (mg/dl) Phos (mg/dl) – – – – – – 5.5. K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease.")
13
Outpatient Labs

14
Pre-operatively, ultrasound of the parathyroid gland was done and it revealed multiple parathyroid gland disease, however, there were only 3 parathyroid glands visualized (right inferior, left superior & left inferior). The aim of the OR was to localize all parathyroid glands and to correct the hyperparathyroidism. Aside from parathyroidectomy, thymectomy was also contemplated, since the thymus is a common site of ectopic parathyroid gland.

15
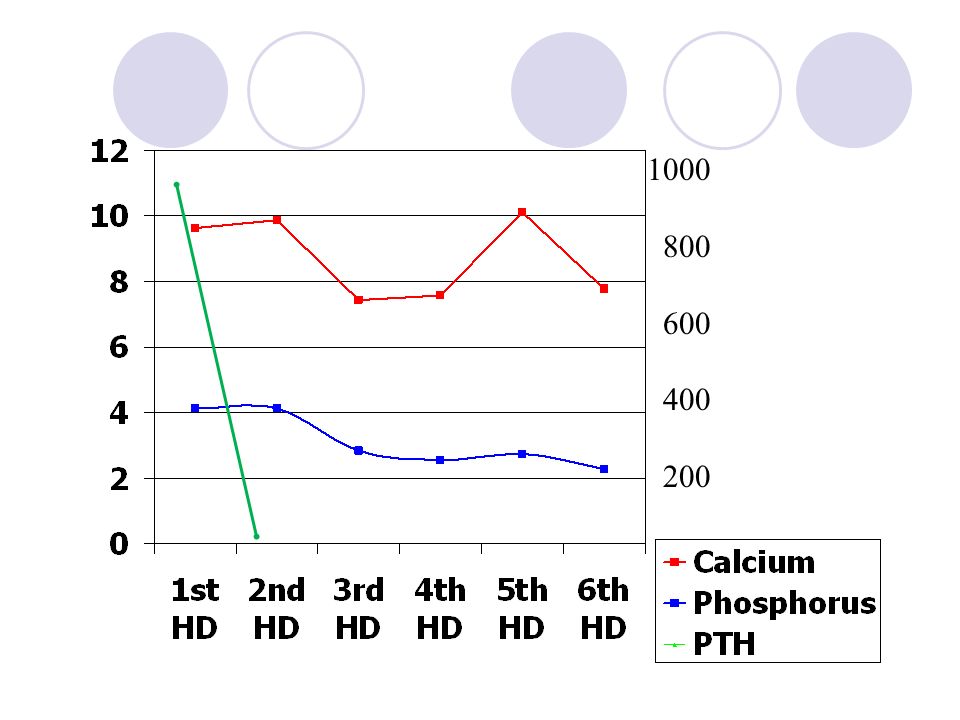
1000 800 600 400 200
16
Day of Surgery

17
Vitamin D Patients on HD or PD with iPTH >300pg/ml
Elevated corrected serum calcium and/or phosphorus levels Patients treated with hemodialysis or peritoneal dialysis with serum levels of intact PTH levels >300 pg/mL (33.0 pmol/L) should receive an active vitamin D sterol (such as calcitriol, alfacalcidol, paricalcitol, or doxercalciferol to reduce the serum levels of PTH to a target range of 150 to 300 pg/ml. The intermittent, intravenous administration of calcitriol is more effective than daily oral calcitriol in lowering serum PTH levels. In patients with corrected serum calcium and/or phosphorus levels above the target range, a trial of alternative vitamin D analogs, such as paricalcitol or doxercalciferol may be warranted. When therapy with vitamin D sterols is initiated or the dose is increased, serum levels of calcium and phosphorus should be monitored at least every 2 weeks for 1 month and then monthly thereafter. The plasma PTH should be measured monthly for at least 3 months and then every 3 months once target levels of PTH are achieved. Patients with CKD who undergo dialysis have reduced plasma levels of 1,25(OH)2D3. This leads to reduced intestinal absorption of calcium (thereby contributing to hypocalcemia) and impaired suppression of the parathyroid gene that initiates the synthesis of PTH. The result is secondary hyperparathyroidism that often progresses. Treatment with calcitriol or another active vitamin D sterol both reduces PTH secretion with resultant improvement of hyperparathyroid bone disease, and improves musculoskeletal symptoms, when these are present.
 should receive an active vitamin D sterol (such as calcitriol, alfacalcidol, paricalcitol, or doxercalciferol to reduce the serum levels of PTH to a target range of 150 to 300 pg/ml. The intermittent, intravenous administration of calcitriol is more effective than daily oral calcitriol in lowering serum PTH levels. In patients with corrected serum calcium and/or phosphorus levels above the target range, a trial of alternative vitamin D analogs, such as paricalcitol or doxercalciferol may be warranted. When therapy with vitamin D sterols is initiated or the dose is increased, serum levels of calcium and phosphorus should be monitored at least every 2 weeks for 1 month and then monthly thereafter. The plasma PTH should be measured monthly for at least 3 months and then every 3 months once target levels of PTH are achieved. Patients with CKD who undergo dialysis have reduced plasma levels of 1,25(OH)2D3. This leads to reduced intestinal absorption of calcium (thereby contributing to hypocalcemia) and impaired suppression of the parathyroid gene that initiates the synthesis of PTH. The result is secondary hyperparathyroidism that often progresses. Treatment with calcitriol or another active vitamin D sterol both reduces PTH secretion with resultant improvement of hyperparathyroid bone disease, and improves musculoskeletal symptoms, when these are present.")
18
Hyperparathyroidism Characterized by excessive secretion of PTH
Primary Secondary Tertiary Symptoms are due to the hypercalcemia itself The parathyroid glands are primarily responsible for maintaining extracellular calcium concentrations. Hyperparathyroidism is a disease characterized by excessive secretion of parathyroid hormone, an 84–amino acid polypeptide hormone. The secretion of parathyroid hormone is regulated directly by the plasma concentration of ionized calcium. Primary hyperparathyroidism is the unregulated overproduction of parathyroid hormone (PTH) resulting in abnormal calcium homeostasis. A single abnormal gland is the cause in 80% of patients. They may arise in hereditary syndromes, such as MEN syndromes. Secondary hyperparathyroidism occurs when partial resistance to the metabolic actions of PTH leads to excessive production of the hormone. Parathyroid gland hyperplasia occurs because resistance to the normal level of PTH leads to hypocalcemia, which, in turn, is a stimulus to parathyroid gland enlargement. PTH hypersecretion, no longer responsive to medical therapy, a state of severe hyperparathyroidism in patients with renal failure, has been referred to as tertiary hyperparathyroidism. This usually requires surgery.
 resulting in abnormal calcium homeostasis. A single abnormal gland is the cause in 80% of patients. They may arise in hereditary syndromes, such as MEN syndromes. Secondary hyperparathyroidism occurs when partial resistance to the metabolic actions of PTH leads to excessive production of the hormone. Parathyroid gland hyperplasia occurs because resistance to the normal level of PTH leads to hypocalcemia, which, in turn, is a stimulus to parathyroid gland enlargement. PTH hypersecretion, no longer responsive to medical therapy, a state of severe hyperparathyroidism in patients with renal failure, has been referred to as tertiary hyperparathyroidism. This usually requires surgery.")
19
Treatment Options Medical Surgical

20
Phosphate Binders phosphorus or iPTH levels not controlled despite phosphorus restriction Calcium-based Noncalcium, nonaluminum, nonmagnesium containing Prolonged hyperphosphatemia causes soft-tissue and vascular calcification due at least in part to an increase in calcium-phosphate product and is associated with increased morbidity and mortality. In the case of vascular calcification, hyperphosphatemia exerts a direct calcifying effect on vascular smooth muscle cells. In another study, serum phosphorus levels >6.2 mg/dL (2.00 mmol/L) were associated with increased blood pressure, hyperkinetic circulation, increased cardiac work, and high arterial tensile stress Calcium-based phosphate binders are effective in lowering serum phosphorus levels and may be used as the initial binder therapy. In CKD Patients With Kidney Failure (Stage 5): Both calcium-based phosphate binders and other noncalcium-, nonaluminum-, nonmagnesium-containing phosphate-binding agents (such as sevelamer HCl) are effective in lowering serum phosphorus levels and either may be used as the primary therapy. In dialysis patients who remain hyperphosphatemic (serum phosphorus >5.5 mg/dL [1.78 mmol/L]) despite the use of either of calcium-based phosphate binders or other noncalcium-, nonaluminum-, nonmagnesium-containing phosphate-binding agents, a combination of both should be used. 5.5 The total dose of elemental calcium provided by the calcium-based phosphate binders should not exceed 1,500 mg/day and the total intake of elemental calcium (including dietary calcium) should not exceed 2,000 mg/day. In patients with serum phosphorus levels >7.0 mg/dL (2.26 mmol/L), aluminum-based phosphate binders may be used as a short-term therapy (4 weeks), and for one course only, to be replaced thereafter by other phosphate binders. In such patients, more frequent dialysis should also be considered.
 were associated with increased blood pressure, hyperkinetic circulation, increased cardiac work, and high arterial tensile stress. Calcium-based phosphate binders are effective in lowering serum phosphorus levels and may be used as the initial binder therapy. In CKD Patients With Kidney Failure (Stage 5): Both calcium-based phosphate binders and other noncalcium-, nonaluminum-, nonmagnesium-containing phosphate-binding agents (such as sevelamer HCl) are effective in lowering serum phosphorus levels and either may be used as the primary therapy. In dialysis patients who remain hyperphosphatemic (serum phosphorus >5.5 mg/dL [1.78 mmol/L]) despite the use of either of calcium-based phosphate binders or other noncalcium-, nonaluminum-, nonmagnesium-containing phosphate-binding agents, a combination of both should be used. 5.5 The total dose of elemental calcium provided by the calcium-based phosphate binders should not exceed 1,500 mg/day and the total intake of elemental calcium (including dietary calcium) should not exceed 2,000 mg/day. In patients with serum phosphorus levels >7.0 mg/dL (2.26 mmol/L), aluminum-based phosphate binders may be used as a short-term therapy (4 weeks), and for one course only, to be replaced thereafter by other phosphate binders. In such patients, more frequent dialysis should also be considered.")
21
Vitamin D Patients on HD or PD with iPTH >300pg/ml
Elevated corrected serum calcium and/or phosphorus levels Patients treated with hemodialysis or peritoneal dialysis with serum levels of intact PTH levels >300 pg/mL (33.0 pmol/L) should receive an active vitamin D sterol (such as calcitriol, alfacalcidol, paricalcitol, or doxercalciferol to reduce the serum levels of PTH to a target range of 150 to 300 pg/ml. The intermittent, intravenous administration of calcitriol is more effective than daily oral calcitriol in lowering serum PTH levels. In patients with corrected serum calcium and/or phosphorus levels above the target range, a trial of alternative vitamin D analogs, such as paricalcitol or doxercalciferol may be warranted. When therapy with vitamin D sterols is initiated or the dose is increased, serum levels of calcium and phosphorus should be monitored at least every 2 weeks for 1 month and then monthly thereafter. The plasma PTH should be measured monthly for at least 3 months and then every 3 months once target levels of PTH are achieved. Patients with CKD who undergo dialysis have reduced plasma levels of 1,25(OH)2D3. This leads to reduced intestinal absorption of calcium (thereby contributing to hypocalcemia) and impaired suppression of the parathyroid gene that initiates the synthesis of PTH. The result is secondary hyperparathyroidism that often progresses. Treatment with calcitriol or another active vitamin D sterol both reduces PTH secretion with resultant improvement of hyperparathyroid bone disease, and improves musculoskeletal symptoms, when these are present.
 should receive an active vitamin D sterol (such as calcitriol, alfacalcidol, paricalcitol, or doxercalciferol to reduce the serum levels of PTH to a target range of 150 to 300 pg/ml. The intermittent, intravenous administration of calcitriol is more effective than daily oral calcitriol in lowering serum PTH levels. In patients with corrected serum calcium and/or phosphorus levels above the target range, a trial of alternative vitamin D analogs, such as paricalcitol or doxercalciferol may be warranted. When therapy with vitamin D sterols is initiated or the dose is increased, serum levels of calcium and phosphorus should be monitored at least every 2 weeks for 1 month and then monthly thereafter. The plasma PTH should be measured monthly for at least 3 months and then every 3 months once target levels of PTH are achieved. Patients with CKD who undergo dialysis have reduced plasma levels of 1,25(OH)2D3. This leads to reduced intestinal absorption of calcium (thereby contributing to hypocalcemia) and impaired suppression of the parathyroid gene that initiates the synthesis of PTH. The result is secondary hyperparathyroidism that often progresses. Treatment with calcitriol or another active vitamin D sterol both reduces PTH secretion with resultant improvement of hyperparathyroid bone disease, and improves musculoskeletal symptoms, when these are present.")
22
Calcimimetic Drugs Activate the calcium-sensing receptor and inhibit parathyroid cell function Results in reduction without normalization of PTH levels Reduction & normalization of calcium Cinacalcet

23
Treatment Options (Surgical)
Subtotal or total parathyroidectomy, with or without parathyroid tissue autotransplantation Ablation of parathyroid tissue by direct injection of alcohol Kidney transplantation Effective surgical therapy of severe hyperparathyroidism can be accomplished by subtotal or total parathyroidectomy with parathyroid tissue autotransplantation. All of these methods can result in satisfactory outcomes, and no one technique appears to provide superior outcomes. Accordingly, the choice of procedure may be at the discretion of the surgeons involved. It is important to emphasize that if reimplantation of parathyroid tissue is considered, that a portion of the smallest parathyroid gland, one less likely to have severe nodular hyperplasia, should be reimplanted. Total parathyroidectomy probably is not the procedure of choice in patients who may subsequently receive a kidney transplant, since the subsequent control of serum calcium levels may be problematic in such patients. An alternative to surgical removal of parathyroid glands has recently been introduced in which parathyroid tissue is ablated by direct injection of alcohol into the parathyroid gland under ultrasound guidance. Additional long-term studies with this technique are needed to evaluate its role in long-term therapy. Kidney transplantation can have beneficial effects upon hyperparathyroidism by reversal of hyperphosphatemia and production of 1,25-dihydroxyvitamin D3 by the renal allograft.PTH levels tend to decline over time as the hyperplastic parathyroid glands undergo involution. Within approximately 3 to 6 months after successful transplant, it can be anticipated that 50% of patients with serum creatinine <2.0 mg/dL (177 mmol/L) will have normal levels of intact PTH. Most reports indicate that intact PTH levels usually return to near normal by 1 year after transplant. However, PTH levels can remain above normal, presumably due to persistent parathyroid hyperplasia, as evidenced by other reports.
 will have normal levels of intact PTH. Most reports indicate that intact PTH levels usually return to near normal by 1 year after transplant. However, PTH levels can remain above normal, presumably due to persistent parathyroid hyperplasia, as evidenced by other reports.")
24
Parathyroidectomy in Patients with CKD
persistent iPTH >800 pg/mL associated with hypercalcemia and/or hyperphosphatemia that are refractory to medical therapy iCa measured every 4 to 6 hours for the first 48 to 72 hours after surgery, and then twice daily until stable. Criteria for adequate excision 50% drop in PTH from the baseline level to the 10-minute postexcision level or 50% drop in PTH from the preexcision level at 10 minutes and a postexcision level below the baseline level. If ionized or corrected total calcium fall below normal (<3.6 mg/dL, calcium gluconate infusion should be initiated at a rate of 1 to 2 mg elemental calcium per kilogram body weight per hour and adjusted to maintain an ionized calcium in the normal range (4.6 to 5.4 mg/dL) A 10-mL ampule of 10% calcium gluconate contains 90 mg of elemental calcium. The calcium infusion should be gradually reduced when the level of ionized calcium attains the normal range and remains stable
 A 10-mL ampule of 10% calcium gluconate contains 90 mg of elemental calcium. The calcium infusion should be gradually reduced when the level of ionized calcium attains the normal range and remains stable.")
25
Surgical Complications after Parathyroidectomy
Nerve damage Bleeding Infection

26
Biochemical Aberrations in a Dialysis Patient Following Parathyroidectomy
Severe hypocalcemia hypophosphatemia hyperkalemia. The abrupt withdrawal of PTH often results in a marked reduction in osteoclast activity. In this setting, osteoblast-mediated bone formation proceeds unopposed, resulting in a dramatic increase in the uptake of calcium and phosphate by bone. Taken together, the combination of decreased bone resorption and improved bone mineralization results in a decrease in serum calcium concentration. The reduced mobilization of phosphate from bone and an increased movement of this divalent anion into bone causes abrupt hypophosphatemia. Cruz, Dinna, et. Al.;American Journal of Kidney Disease, vol 29, No 5 (May) 1997; pp
 1997; pp")
27
Hungry Bone Syndrome Severe post-operative hypocalcemia despite normal or elevated PTH Occurs in patients who have developed bone disease preoperatively due to a chronic increase in bone resorption induced by high PTH Hypocalcemia is a common problem after parathyroidectomy. This is primarily due to functional or relative hypoparathyroidism, leading to reductions in bone reabsorption and intestinal calcium absorption. The hypocalcemia is generally transient because the degree of bone disease is typically mild and normal parathyroid tissue recovers function quickly (usually within one week), even after long-term suppression. The postoperative hypocalcemia probably results from acute reversal of the PTH-induced contribution of bone to maintenance of the serum calcium concentration. In the high turnover state associated with hyperparathyroidism, PTH increases bone formation and resorption with a net efflux of calcium from bone. Sudden withdrawal of PTH in such patients causes an imbalance between osteoblast-mediated bone formation and osteoclast-mediated bone resorption and perhaps other changes affecting calcium fluxes, leading to a marked net increase in bone uptake of calcium, phosphate, and magnesium. Thus, the hungry bone syndrome requires an abrupt decrease in PTH release that upsets the equilibrium between calcium efflux from bone and influx into the skeleton during bone remodeling.
, even after long-term suppression. The postoperative hypocalcemia probably results from acute reversal of the PTH-induced contribution of bone to maintenance of the serum calcium concentration. In the high turnover state associated with hyperparathyroidism, PTH increases bone formation and resorption with a net efflux of calcium from bone. Sudden withdrawal of PTH in such patients causes an imbalance between osteoblast-mediated bone formation and osteoclast-mediated bone resorption and perhaps other changes affecting calcium fluxes, leading to a marked net increase in bone uptake of calcium, phosphate, and magnesium. Thus, the hungry bone syndrome requires an abrupt decrease in PTH release that upsets the equilibrium between calcium efflux from bone and influx into the skeleton during bone remodeling.")
28
Diagnosis of Hungry Bone Syndrome
Persistently low serum calcium following parathyroidectomy Low or low normal serum phosphate Rising/raised serum alkaline phosphatase Low urine calcium These are the markers of increased bone formation after the sudden withdrawal of PTH. Serum raised alkaline phosphatase is secondary to increased osteoblastic activity. Urinary calcium and phosphate concentrations are reduced, indicating total body deficiency.

29
Treatment Elemental Calcium Vitamin D Calcium gluconate
Calcium carbonate Vitamin D Elemental calcium 100–300 mg (10–30 ml of 10% calcium gluconate) diluted in 150 ml of five percent dextrose solution should be administered over ten minutes. If calcium gluconate is not available, calcium carbonate can be used. Calcium can also be diluted in isotonic saline or water but should not be used undiluted, as concentrated solutions can cause thrombophlebitis. The intravenous calcium solution must not also contain bicarbonate or phosphate, which can form insoluble calcium salts. Such regimens do not increase serum calcium for more than two hours, and should therefore be followed by a continuous infusion of elemental calcium 0·5–1·5 mg/Kg/hour (1 mmol ten per cent calcium gluconate is equivalent to 10 mg of elemental calcium). The intravenous calcium infusion should be continued until the patient is asymptomatic and tolerating oral calcium and vitamin 1,25 (OH)2D (calcitriol). Calcitriol is the preferred vitamin D preparation as the conversion of 25 to 1,25 (OH)2D requires 1α hydroxylation in the kidney, which is mediated by parathyroid hormone. In hungry bone syndrome, with the sudden withdrawal of parathyroid hormone, the activity of this enzyme is minimal. Since bone mineral density has been noted to increase for one year after successful parathyroidectomy, it is prudent to continue calcium supplementation for one year. Frequent measurements of urinary calcium are important to avoid progression of hypocalcaemia, to detect hypercalciuria and to guide adjustment of calcium and vitamin D therapy. When significant hypomagnesaemia is associated with hypocalcaemia, it is best treated using the parenteral route. Up to 50 mmol/day can be administered safely in a patient with normal renal function. A large fraction of parenterally administered magnesium may be excreted in the urine, even in the presence of profound total body deficiency. In hungry bone syndrome, hypomagnesaemia is usually corrected with the correction of hypocalcaemia. In cases of hypophosphataemia, intravenous phosphate is avoided since phosphate can combine with calcium to produce a further drop in serum calcium concentration. An exception to this rule is the presence of severe hypophosphataemia (less than 0·31mmol/L) where phosphate supplementation is necessary. The phosphate should be replaced by oral, intravenous or intraperitoneal routes in patients on dialysis.
 diluted in 150 ml of five percent dextrose solution should be administered over ten minutes. If calcium gluconate is not available, calcium carbonate can be used. Calcium can also be diluted in isotonic saline or water but should not be used undiluted, as. concentrated solutions can cause thrombophlebitis. The intravenous calcium solution must not also contain bicarbonate or phosphate, which can form insoluble calcium salts. Such regimens do not increase serum calcium for more than two hours, and should therefore be followed by a continuous infusion of elemental calcium 0·5–1·5 mg/Kg/hour (1 mmol ten per cent calcium gluconate is equivalent to 10 mg of elemental calcium). The intravenous calcium infusion should be continued until the patient is asymptomatic and tolerating oral calcium and vitamin 1,25 (OH)2D (calcitriol). Calcitriol is the preferred vitamin D preparation as the conversion of 25 to 1,25 (OH)2D requires 1α hydroxylation in the kidney, which is mediated by parathyroid hormone. In. hungry bone syndrome, with the sudden withdrawal of parathyroid hormone, the activity of this enzyme is minimal. Since bone mineral density has been noted to increase for one year after successful parathyroidectomy, it is prudent to continue calcium supplementation for one year. Frequent measurements of urinary calcium are important to avoid progression of hypocalcaemia, to detect hypercalciuria and to guide adjustment of calcium and vitamin D therapy. When significant hypomagnesaemia is associated with hypocalcaemia, it is best treated using the parenteral route. Up to 50 mmol/day can be administered safely in a patient with normal renal function. A large fraction of parenterally administered magnesium may be excreted in the urine, even in the presence of profound total body deficiency. In hungry bone syndrome, hypomagnesaemia is usually corrected with the correction. of hypocalcaemia. In cases of hypophosphataemia, intravenous phosphate is avoided since phosphate can combine with calcium to produce a further drop in serum calcium concentration. An exception to this rule is the presence of severe hypophosphataemia (less than 0·31mmol/L) where phosphate supplementation is necessary. The phosphate should be replaced by oral, intravenous or intraperitoneal routes in patients on dialysis.")
30
Can Pamidronate Prevent Hungry Bone Syndrome After parathyroidectomy?
Bisphosphonates may be beneficial in preventing hungry bone syndrome by reducing bone formation First report involved a 62-year-old woman with severe hyperparathyroidism who received 60 mg of pamidronate prior to parathyroidectomy. Another study retrospectively reviewed medical records to determine the effect of pre-operatively administered bisphosphonates on serum calcium levels following parathyroidectomy. Out of 14 patients who did not have hungry bone syndrome 6 had received bisphosphonates prior to surgery. Yuriy Gurevich, DO, and Leonid Poretsky, MD:Can Pamidronate Prevent Hungry Bone Syndrome after Parathyroidectomy, a case report

32
Current Status of the Patient:
On Dialysis thrice a week On maintenance medications Still no match for kidney transplant

33
Thank You!

Similar presentations




 Male Filipino Roman Catholic Sampaloc, Manila Informant: Mother Reliability: Good.>")


>")












