Download presentation
Presentation is loading. Please wait.

1
Treatment Algorithms in Crohn’s Disease

2
In Most Clinical Scenarios of Crohn’s Disease
Premise and Preview In Most Clinical Scenarios of Crohn’s Disease Therapy is Sequential

3
Goals of Therapy for IBD
Inducing remission Maintaining remission Restoring and maintaining nutrition Maintaining patient’s quality of life Surgical intervention (selection of optimal time for surgery)
")
4
Long-term Evolution of Disease Behavior in CD
100 90 80 70 60 Penetrating Cumulative Probability (%) 50 40 Inflammatory 30 Stricturing 20 10 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180 192 204 216 228 240 Months Patients at risk: N = 2002 552 229 95 37 Cosnes J et al. Inflamm Bowel Dis. 2002;8:244.
 Inflammatory. 30. Stricturing Months. Patients at risk: N = Cosnes J et al. Inflamm Bowel Dis. 2002;8:244.")
5
Crohn’s Disease: Anatomic Distribution
Small bowel alone (33%) Ileocolic (45%) Colon alone (20%) Freq of involvement Most Least
 Ileocolic (45%) Colon alone (20%) Freq of involvement. Most. Least.")
6
Cumulative Probability of Surgical Intervention in CD
100 ± 2 SD 80 60 Probability (%) 40 20 Dx 2 5 8 11 14 17 20 Years Events (no.) Munkholm P et al. Gastroenterology. 1993;105:1716. Revised mwa
 Dx Years. Events (no.) Munkholm P et al. Gastroenterology. 1993;105:1716. Revised mwa.")
7
Inductive Therapies for Crohn’s Disease
Aminosalicylates Antibiotics Corticosteroids Infliximab

8
Therapeutic Pyramid for Active Crohn’s Disease
Surgery Severe Immunomodulators Infliximab (Prednisone) ? Moderate Corticosteroids The therapeutic pyramid for Crohn’s disease is based upon clinical trials. Controlled release budesonide has been advocated for mild-moderate disease in countries where it is available. Infliximab has been efficacious independent of concomitant medications. (Budesonide) Mild Aminosalicylates/Antibiotics
 Moderate. Corticosteroids. The therapeutic pyramid for Crohn’s disease is based upon clinical trials. Controlled release budesonide has been advocated for mild-moderate disease in countries where it is available. Infliximab has been efficacious independent of concomitant medications. (Budesonide) Mild. Aminosalicylates/Antibiotics.")
9
Treatment of Mild-Moderate Crohn’s Disease

10
NCCDS: Response to Therapy for Active Crohn’s Disease
60 50 40 30 20 10 70 Sulfasalazine 1 g/15 kg (5 g) Patients (%) 13% Placebo 5 10 15 Weeks after Randomization NCCDS, National Cooperative Crohn’s Disease Study. Summers RW et al. Gastroenterology 1979;77:
 Patients (%) 13% Placebo Weeks after Randomization. NCCDS, National Cooperative Crohn’s Disease Study. Summers RW et al. Gastroenterology 1979;77:")
11
Meta-Analysis of Pentasa® (4g/day) in Active Crohn’s Disease
Pentasa® 4 g minus Placebo Pentasa® 4 g Placebo -10 -10 P=0.7 P=0.5 -20 -20 -30 P=0.04 -30 Change from baseline in CDAI score -40 -50 P=0.7 -40 -60 -50 -70 P=0.04 P=0.005 P=0.005 P=0.05 -60 -80 Crohn's I Crohn's II Crohn's III Overall Crohn's I Crohn’s II Crohn's III Overall n=155 n=150 n=310 n=615 n=155 n=150 n=310 n=615 Hanauer, Stromber. Clinical Gastroenterology & Hepatology 2004

12
Antibiotics in Active CD
% Remission Metro + Cipro Metro Cipro vs. Me-Pred vs. SASP vs. Mesalamine Prantera 1996; Ursing 1982; Colombel 1999

13
Corticosteroids in Crohn’s Disease
Faubion et al (Olmsted County, ) “Only 43% of inception cohort ever required steroids”
 Only 43% of inception cohort ever required steroids")
14
Corticosteroids in CD: Induction of Remission
p not calculated 92%† 100 Corticosteroids 82%* Placebo 80 60%* 60 38% % Patients 40 30% 20 NCCDS ECCDS GETAID 17 weeks 18 weeks 7 weeks Clinical Remission *Randomized controlled trial †Multicenter prospective trial Malchow H et al. Gastroenterology. 1984;86:249. Modigliani R et al. Gastroenterology. 1990;98:811. Summers RW et al. Gastroenterology. 1979;77:847.

15
Corticosteroid Therapy for Crohn’s Disease
Immediate Outcome* (n = 74) Complete Remission 58% (n = 43) Partial Remission 26% (n = 19) No Response 16% (n = 12) Prolonged Response 32% (n = 24) Steroid Dependent 28% (n = 21) Surgery 38% (n = 28) 1-Year Outcome (n = 74) Steroid Dependence Patients who initially respond to treatment with corticosteroids frequently become dependent within months of that response. The prospective evaluation of Munkholm et al involving 196 patients with CD demonstrated that more than one third of patients who achieved complete or partial clinical remission of active CD with prednisolone therapy (1 mg/kg per day, reduced within weeks to a maintenance dose of 10–15 mg/d) developed a dependency on corticosteroids within the first year of treatment. In the Munkholm study, dependence was defined as 1. relapse within 30 days of steroid discontinuation, or 2. relapse upon dose reduction, impeding steroid discontinuation for more than 1 year. Because this definition of steroid dependency is considered excessively lenient, the dependence rate may be underestimated. A consensus has not formally been reached regarding the definition of steroid dependency, but many clinicians agree that recurrence of symptoms with dosage reduction prohibiting the cessation of steroid therapy after a period of at least 3 months constitutes dependency. *30 days after initiating corticosteroid therapy Faubion W et al. Gastroenterology 2001;121:225
 Complete. Remission. 58% (n = 43) Partial. Remission. 26% (n = 19) No. Response. 16% (n = 12) Prolonged Response. 32% (n = 24) Steroid Dependent. 28% (n = 21) Surgery. 38% (n = 28) 1-Year. Outcome. (n = 74) Steroid Dependence. Patients who initially respond to treatment with corticosteroids frequently become dependent within months of that response. The prospective evaluation of Munkholm et al involving 196 patients with CD demonstrated that more than one third of patients who achieved complete or partial clinical remission of active CD with prednisolone therapy (1 mg/kg per day, reduced within weeks to a maintenance dose of 10–15 mg/d) developed a dependency on corticosteroids within the first year of treatment. In the Munkholm study, dependence was defined as. 1. relapse within 30 days of steroid discontinuation, or. 2. relapse upon dose reduction, impeding steroid discontinuation for more than 1 year. Because this definition of steroid dependency is considered excessively lenient, the dependence rate may be underestimated. A consensus has not formally been reached regarding the definition of steroid dependency, but many clinicians agree that recurrence of symptoms with dosage reduction prohibiting the cessation of steroid therapy after a period of at least 3 months constitutes dependency. *30 days after initiating corticosteroid therapy. Faubion W et al. Gastroenterology 2001;121:225.")
16
Outcome of Corticosteroid Therapy for CD
Remission 48% Improved 32% No change 20% 12-month outcomes 1-month outcomes Remission 54% Relapse 46% Improved 57% Relapse 43% * Remission at 12 Months = 25% Munkholm. Gut 1994;35:

17
Corticosteroids: Maintenance of Remission
n=274; p=NS 80 n=59; p=NS 75% 76% Steroid Placebo 70 58% 60 55% 50 n=237; p=NS % Patients in Remission 40 30% 30 23% 20 10 Smith Summers Malchow 36 months 12 months 24 months Bergman L et al. Scand J Gastroenterol. 1976;11:651. Malchow H et al. Gastroenterology. 1984;86:249. Smith RC et al. Gut. 1978;19:606. Summers RW et al. Gastroenterology. 1979;77:847.

18
Overview of Corticosteroids in CD
Induce remission (NCCDS,* ECCDS,† GETAID‡) Provide rapid symptomatic relief (NCCDS,* ECCDS,† GETAID‡) Frequent corticosteroid dependency with prolonged use DO NOT maintain remission Dose- and duration-related adverse events with acute and chronic therapy *Summers RW et al. Gastroenterology. 1979;77:847. †Malchow H et al. Gastroenterology. 1984;86:249. ‡Modigliani R et al. Gastroenterology. 1990;98:811. Faubion WA Jr et al. Gastroenterology. 2001;121:255. Keenan GF et al. Clin Chest Med. 1997;18:507. Munkholm P et al. Gut. 1994;35:360. Singleton JW et al. Gastroenterology. 1979;77:870. Steinhart AH et al. Cochrane Database Syst Rev. 2003;CD
 Provide rapid symptomatic relief (NCCDS,* ECCDS,† GETAID‡) Frequent corticosteroid dependency with prolonged use. DO NOT maintain remission. Dose- and duration-related adverse events with acute and chronic therapy. *Summers RW et al. Gastroenterology. 1979;77:847. †Malchow H et al. Gastroenterology. 1984;86:249. ‡Modigliani R et al. Gastroenterology. 1990;98:811. Faubion WA Jr et al. Gastroenterology. 2001;121:255. Keenan GF et al. Clin Chest Med. 1997;18:507. Munkholm P et al. Gut. 1994;35:360. Singleton JW et al. Gastroenterology. 1979;77:870. Steinhart AH et al. Cochrane Database Syst Rev. 2003;CD")
19
Remission Rates in Acute Crohn’s Studies with Budesonide CIR
Remission rates at 8 weeks (%) 70 60 50 40 30 20 10 Bud CIR Bud CIR Placebo Pentasa® Prednisolone 9 mg QD 4.5 mg BID 2 g BID 40 mg Greenberg 1994; Rutgeerts 1994; Thomsen 1998
 Bud CIR Bud CIR Placebo Pentasa® Prednisolone. 9 mg QD 4.5 mg BID 2 g BID 40 mg. Greenberg 1994; Rutgeerts 1994; Thomsen")
20
Maintenance Therapy for Crohn’s Disease: Issues
Definition of remission Clinical, endoscopic, radiologic, laboratory Induction therapy 5-ASA, steroids, antibiotics, immunomodulators Surgery Disease location Disease behavior Inflammatory, fibrostenotic, fistulizing Smoking

21
NCCDS - Response to Therapy for Crohn’s Disease Remission Maintenance
Months after Randomization Summers. Gastroenterology 1979

22
Oral Budesonide as Maintenance Therapy for CD
1 Budesonide 6 mg Budesonide 3 mg Placebo Cumulative probability of remission 0.5 P = ns 100 200 300 Days Adapted from Greenberg GR et al. Gastroenterology 1996;110:45-51

23
Outcomes for Mild-Moderate Disease

24
Antibiotics Metronidazole MOA: Dosing:
It is thought that metronidazole may have anti-inflammatory effects as well as antibacterial effects. Dosing: Metronidazole is most useful in treating fistulizing CD in doses ranging from 1 g/day to 2 g/day. Treatment of 2 months or longer is necessary for fistula healing. Discontinuing metronidazole therapy often results in an exacerbation of the fistula drainage.

25
Antibiotics Ciprofloxacin:
Recently, ciprofloxacin in doses of 1–1.5 g/day has been used as an alternative to metronidazole. Ciprofloxacin has not been well studied as monotherapy. In small studies, it appears to be mainly effective in treating perianal and fistulizing CD. It may be useful in combination with metronidazole. One study suggested that this combination could be an alternative treatment to steroids in treating the acute phase of CD.

26
Budesonide Highly potent glucocorticoid.
First pass metabolism in the liver , resulting in a systemic bioavailability of 10–15%. Low corticosteroid-related adverse effects, including adrenal suppression, (due to the low systemic bioavailability). Approved in the U.S. in 2001 for pts with mild to moderate, active CD involving the ileum and/or ascending colon.
. Approved in the U.S. in 2001 for pts with mild to moderate, active CD involving the ileum and/or ascending colon.")
27
Budesonide A recently published meta-analysis (total 621 enrolled pts)
Suggests that budesonide is not as effective as standard doses of the steroids in inducing remission. * Budesonide induced remission in 50–70% of pts with active disease in the ileum or in the right ileocolonic area. * Older steroids induced remission in 60–73% of pts. This indicates that budesonide is not superior to older agents in inducing remission for active CD but may be an alternative to mesalamine in these patients.

28
“Evidence-Based” Approach of Sandborn and Feagan
Mild-Moderate Crohn’s Disease Left-sided disease restricted to colon Disease involving the ileum and/or ascending colon Sulfasalazine 16 weeks Budesonide capsules 8-16 weeks Sulfa-allergic/failed treatment Failed treatment >60% 45% acute 80% 1 year Conventional steroids Sandborn, Feagan, 2003

29
Topics Antimetabolite therapy Anti-inflammatory cytokines TNF blockade

30
AZA: Induction of Remission
NCCDS Data 80 60 % Response 40 20 P=0.17 10 Weeks Prednisone Placebo AZA

31
AZA and 6-MP: Induction of Remission in CD
Pearson DC et al. Ann Intern Med 1995;122:

32
Azathioprine and 6-Mercaptopurine in IBD: Toxicity
Common Gastrointestinal intolerance Myalgia Uncommon Bone marrow suppression Pancreatitis Allergic reactions Hepatic toxicity Opportunistic infection Neoplasm Present DH. Gastroenterol Clin North Am 1989;18:57-71

33
Methotrexate

34
MTX Results: Remission
50 P =0.025 % Response 25 19.1% 39.4% Placebo MTX Feagan. N Eng J Med. 1995;332(5):292-7
:")
35
Methotrexate: Time to Relapse
% Remission Methotrexate Placebo Weeks Since Randomization Feagan BG. N Engl J Med 2000;342(22):
:")
36
Methotrexate in IBD: Toxicity
Major Hepatic Myelosuppressive Pulmonary Fertility-related Teratogenic Enteritic/colitic Minor Gastrointestinal Alopecia-inductive Allergic Neurologic Egan LJ, Sandborn WJ. Mayo Clin Proc 1996;71:69-80

37
Cyclosporine

38
Cyclosporine in CD Feagan BG. Inflammatory Bowel Dis 1995;1:

39
Biologic Therapy

40
Infliximab: Mechanism of Action

41
Healing of Colonic Ulceration with Infliximab
Pretreatment 4 weeks post-treatment Van Dullemen HM et al. Gastroenterology 1995;109:

42
Median Time to Loss of Response Through Week 54
ACCENT I Median Time to Loss of Response Through Week 54 Week 2 Responders Hanauer S, Feagan B. Lancet. 2002;359:1541-9

43
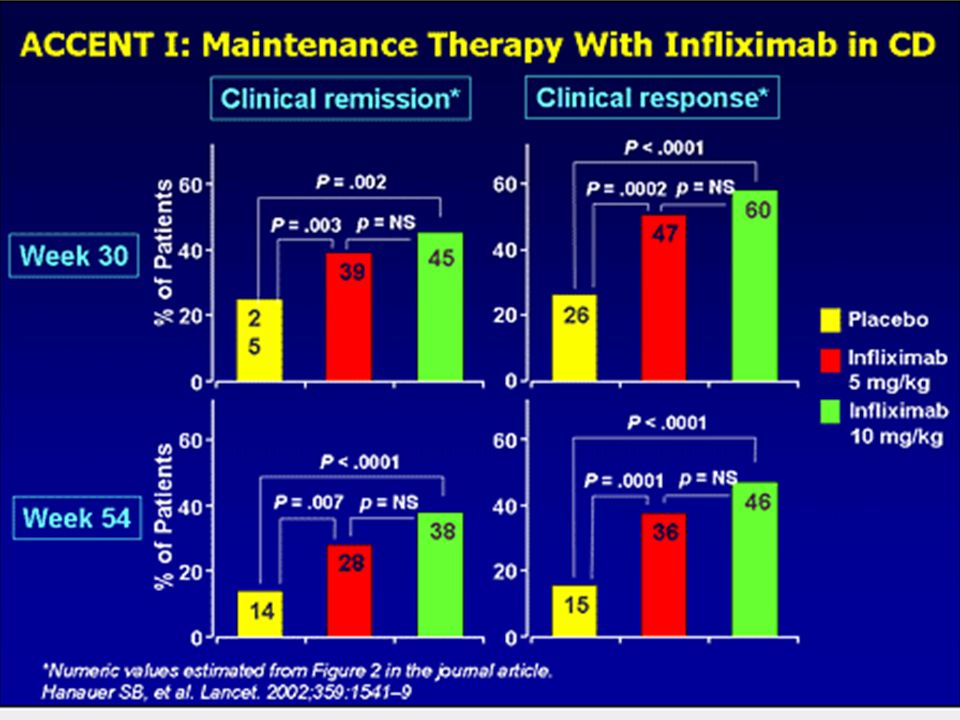
Clinical Remission at Week 54*
ACCENT I Clinical Remission at Week 54* 50 P<0.001 38% 40 P=NS P=0.007 28% 30 Proportion of Patients (%) 20 14% 10 Single Dose (n=110) 5 mg/kg q 8 wk (n=113) 10 mg/kg q 8 wk (n=112) *Week-2 responders Hanauer SB, et al. Lancet 2002
 % 10. Single Dose. (n=110) 5 mg/kg. q 8 wk. (n=113) 10 mg/kg. q 8 wk. (n=112) *Week-2 responders. Hanauer SB, et al. Lancet")
44
REMICADE® (infliximab) in Patients with Fistulizing Crohn’s Disease
Present, et al. REMICADE® (infliximab) in Patients with Fistulizing Crohn’s Disease Complete Response: All Fistulas Closed P=0.04 P=0.001 * *Placebo=Conventional Therapy Present D, et al. N Engl J Med. 1999;340:
 in Patients with Fistulizing Crohn’s Disease. Complete Response: All Fistulas Closed. P=0.04. P= * *Placebo=Conventional Therapy. Present D, et al. N Engl J Med. 1999;340:")
45
Fistula Response at Week 54
ACCENT II Fistula Response at Week 54 Among Patients Responding at Weeks 10 and 14 P=0.002 P=0.014 Patients in Response (%) The ACCENT II trial was a Phase III study evaluating the safety and efficacy of long-term REMICADE® (infliximab) treatment in patients with fistulizing Crohn’s disease. A total of 296 patients with at least one draining enterocutaneous fistula were included. At baseline approximately 80% of patients were receiving stable doses of ≥1 concomitant Crohn’s-related therapy. All patients received an initial 3-dose induction of REMICADE 5 mg/kg at Weeks 0, 2, and 6. Patients were then randomized based on clinical response at Week 14 to receive REMICADE 5 mg/kg q 8 weeks or placebo through Week 46. The primary endpoint of the study was time to loss of fistula response through Week 54 among patients responding at Week 14. Among patients responding at Weeks 10 and 14, 27% of patients in the placebo-maintenance group still had a response at Week 54 as compared with 49% of patients in the REMICADE 5 mg/kg maintenance group (P=0.002). 23% of placebo maintenance patients had a complete response versus 40% of patients in the REMICADE maintenance group (P=0.014). Analysis excluded patients who had no fistula evaluation at Week 54. 24/89 41/83 24/89 41/83 Sands BE, et al NEJM 2004
 The ACCENT II trial was a Phase III study evaluating the safety and efficacy of long-term REMICADE® (infliximab) treatment in patients with fistulizing Crohn’s disease. A total of 296 patients with at least one draining enterocutaneous fistula were included. At baseline approximately 80% of patients were receiving stable doses of ≥1 concomitant Crohn’s-related therapy. All patients received an initial 3-dose induction of REMICADE 5 mg/kg at Weeks 0, 2, and 6. Patients were then randomized based on clinical response at Week 14 to receive REMICADE 5 mg/kg q 8 weeks or placebo through Week 46. The primary endpoint of the study was time to loss of fistula response through Week 54 among patients responding at Week 14. Among patients responding at Weeks 10 and 14, 27% of patients in the placebo-maintenance group still had a response at Week 54 as compared with 49% of patients in the REMICADE 5 mg/kg maintenance group (P=0.002). 23% of placebo maintenance patients had a complete response versus 40% of patients in the REMICADE maintenance group (P=0.014). Analysis excluded patients who had no fistula evaluation at Week /89. 41/83. 24/89. 41/83. Sands BE, et al NEJM")
46
Fistula Response at Week 54
ACCENT II Fistula Response at Week 54 Among Patients Responding at Weeks 10 and 14 P=0.002 P=0.014 Patients in Response (%) The ACCENT II trial was a Phase III study evaluating the safety and efficacy of long-term REMICADE® (infliximab) treatment in patients with fistulizing Crohn’s disease. A total of 296 patients with at least one draining enterocutaneous fistula were included. At baseline approximately 80% of patients were receiving stable doses of ≥1 concomitant Crohn’s-related therapy. All patients received an initial 3-dose induction of REMICADE 5 mg/kg at Weeks 0, 2, and 6. Patients were then randomized based on clinical response at Week 14 to receive REMICADE 5 mg/kg q 8 weeks or placebo through Week 46. The primary endpoint of the study was time to loss of fistula response through Week 54 among patients responding at Week 14. Among patients responding at Weeks 10 and 14, 27% of patients in the placebo-maintenance group still had a response at Week 54 as compared with 49% of patients in the REMICADE 5 mg/kg maintenance group (P=0.002). 23% of placebo maintenance patients had a complete response versus 40% of patients in the REMICADE maintenance group (P=0.014). Analysis excluded patients who had no fistula evaluation at Week 54. 24/89 41/83 24/89 41/83 Sands, B et al. NEJM 2004
 The ACCENT II trial was a Phase III study evaluating the safety and efficacy of long-term REMICADE® (infliximab) treatment in patients with fistulizing Crohn’s disease. A total of 296 patients with at least one draining enterocutaneous fistula were included. At baseline approximately 80% of patients were receiving stable doses of ≥1 concomitant Crohn’s-related therapy. All patients received an initial 3-dose induction of REMICADE 5 mg/kg at Weeks 0, 2, and 6. Patients were then randomized based on clinical response at Week 14 to receive REMICADE 5 mg/kg q 8 weeks or placebo through Week 46. The primary endpoint of the study was time to loss of fistula response through Week 54 among patients responding at Week 14. Among patients responding at Weeks 10 and 14, 27% of patients in the placebo-maintenance group still had a response at Week 54 as compared with 49% of patients in the REMICADE 5 mg/kg maintenance group (P=0.002). 23% of placebo maintenance patients had a complete response versus 40% of patients in the REMICADE maintenance group (P=0.014). Analysis excluded patients who had no fistula evaluation at Week /89. 41/83. 24/89. 41/83. Sands, B et al. NEJM")
47
Incidence of Antibodies-to-Infliximab (ATI) Maintenance Studies*
Antibody-to-Infliximab (ATI) Status The most frequent AEs (by preferred term) in infliximab-treated patients in all studies were upper respiratory tract infections (27.9%), headache (25.7%), nausea (20.6%), abdominal pain (20.5%), pain (13.9%), pharyngitis (13.5%), arthralgia (13.0%), rash (12.9%), fatigue (11.9%), sinusitis (11.7%), vomiting (11.6%) fever (11.5%), diarrhea and dizziness (each 10.8%), and coughing (10.0%). % of Pts with ATI % of Patients Inconclusive† % of Pts without ATI ACCENT I CD n = 514 Week 72 ACCENT II CD n = 258 Week 54 ATTRACT RA n = 295 Week 102 ASPIRE RA n = 629 Week 54 p. 94 and 95 of ASPIRE ISS Maintenance Studies * pts with evaluable samples † pts with long-lasting serum concentrations of infliximab and never ATI (+) ASPIRE: Integrated Safety Summary, Sep. 18, 2003
 Status. The most frequent AEs (by preferred term) in infliximab-treated patients in all studies. were upper respiratory tract infections (27.9%), headache (25.7%), nausea (20.6%), abdominal pain (20.5%), pain (13.9%), pharyngitis (13.5%), arthralgia (13.0%), rash. (12.9%), fatigue (11.9%), sinusitis (11.7%), vomiting (11.6%) fever (11.5%), diarrhea. and dizziness (each 10.8%), and coughing (10.0%). % of Pts with ATI. % of Patients Inconclusive† % of Pts without ATI. ACCENT I CD. n = 514. Week 72. ACCENT II. CD. n = 258. Week 54. ATTRACT. RA. n = 295. Week 102. ASPIRE. RA. n = 629. Week 54. p. 94 and 95 of ASPIRE ISS. Maintenance Studies. * pts with evaluable samples. † pts with long-lasting serum concentrations of infliximab and never ATI (+) ASPIRE: Integrated Safety Summary, Sep. 18,")
48
Infliximab and Antibody Formation
Cohort study (n = 125): mean of 3.9 infusions / 10 months 61% of patients developed ATI Antibody formation inversely associated with serum infliximab concentration ATI formation > 8 ug predicted shorter duration of response (35 vs. 71 days) – present in 37% Approximately 2.5 times as likely to form ATI if concomitant antimetabolite therapy was not used Baert et al. N Engl J Med 2003;348:7
: mean of 3.9 infusions / 10 months. 61% of patients developed ATI. Antibody formation inversely associated with serum infliximab concentration. ATI formation > 8 ug predicted shorter duration of response (35 vs. 71 days) – present in 37% Approximately 2.5 times as likely to form ATI if concomitant antimetabolite therapy was not used. Baert et al. N Engl J Med 2003;348:7.")
54
Prevention of ATIs Avoid intermittent therapy
Use effective preventative strategies: MTX/AZA for chronic use * Farrell R. Gastroenterology 2003;124(4):917-24
:")
55
CD: Mild to Moderate Active symptoms/ flare
Consider 5-ASA Consider Abx Exclude enteric pathogen Ileal/ R colon Not confined to ileal/ R colon No response Budesonide Prednisone Response Response No flare No flare Observe Taper Taper Observe Patients with a new mild to moderately severe flare of Crohn’s disease should be evaluated for an intercurrent enteric infection. Patients with ileal and/or right colonic disease respond more rapidly and completely to controlled ileal release budesonide, whereas patients with other anatomic localizations of disease may better respond to oral prednisone by a tapering regimen. Patients with colonic Crohn’s in particular may be considered for treatment with 5-aminosalicylate, particularly sulfasalazine, or antibiotics, such as metronidazole and/or ciprofloxacin. Patients unable to taper off budesonide or prednisone are considered steroid dependent and should be considered for treatment with an immune modulator. Alternatively, for patients with ileal/right colonic disease, a dose of budesonide 9 mg/d or less may be given to minimize symptoms. Flare Flare Consider budesonide titrated to symptoms or 6-MP/AZA or MTX 6-MP/AZA or MTX

56
CD: Moderate to Severe Moderate CD Severe CD Observe Taper PO Steroids
Adequate response Adequate response Success Observe Taper PO Steroids IV Steroids Inadequate response Inadequate response Failure 6-MP/AZA Consider infliximab + 6-MP/AZA or MTX Consider surgery Adequate response Inadequate response/intolerant Maintain 6-MP/AZA or MTX Adequate response Consider change to MTX Inadequate response/intolerant Patients with more active symptoms may require a course of oral or intravenous steroids. Patients who are unable to successfully taper steroids, or who do not respond fully should be considered for 6-mercaptopurine, azathioprine, or methotrexate. Patients who do not fully respond to optimized dosing with these agents may be considered for infliximab, surgery, or investigational therapy. Maintain infliximab + 6-MP/AZA or MTX Adequate response Add infliximab Inadequate response/intolerant Surgery or investigational therapy

57
Infliximab Infliximab indicated Exclude enteric pathogen
Exclude abscess, stricture Exclude latent/active TB (Start 6-MP/AZA or MTX) Response Observe up to 8 wks Infliximab 5 mg/kg wks 0, 2, 6 Consider steroid pre-treatment Consider acetaminophen, diphenhydramine pre-treatment Recurrent sx ≤ 4 wks Recurrent sx > 4 - < 8 wks Recurrent sx ≥ 8 wks Once a decision to treat with infliximab has been made, infectious complications need to be first guarded against by diagnosing and treating enteric pathogens, abscess, tuberculosis, or other infectious issues. Concurrent treatment with an immune modulator is desirable to minimize risk of antibodies to infliximab and subsequent loss of response. Similarly, once a course of treatment has been begun, maintenance dosing at regular intervals of 8 weeks or less should ensue, again to minimize the formation of antibodies to infliximab. Patients who do not respond to 5 mg/kg may respond to dose escalation, while patients who require treatment intervals of less than 8 weeks may be maintained at shorter intervals. Inadequate response Maintain infliximab 5 mg/kg q 4-8 wks Infliximab 10 mg/kg Inadequate response Inadequate response Surgery or investigational Rx Escalate dose or shorten interval Maintain infliximab 5 mg/kg q 8 wks Loss of response
 Response. Observe up to 8 wks. Infliximab 5 mg/kg wks 0, 2, 6. Consider steroid pre-treatment. Consider acetaminophen, diphenhydramine pre-treatment. Recurrent sx ≤ 4 wks. Recurrent sx > 4 - < 8 wks. Recurrent sx ≥ 8 wks. Once a decision to treat with infliximab has been made, infectious complications need to be first guarded against by diagnosing and treating enteric pathogens, abscess, tuberculosis, or other infectious issues. Concurrent treatment with an immune modulator is desirable to minimize risk of antibodies to infliximab and subsequent loss of response. Similarly, once a course of treatment has been begun, maintenance dosing at regular intervals of 8 weeks or less should ensue, again to minimize the formation of antibodies to infliximab. Patients who do not respond to 5 mg/kg may respond to dose escalation, while patients who require treatment intervals of less than 8 weeks may be maintained at shorter intervals. Inadequate response. Maintain infliximab 5 mg/kg q 4-8 wks. Infliximab 10 mg/kg. Inadequate response. Inadequate response. Surgery or investigational Rx. Escalate dose or shorten interval. Maintain infliximab 5 mg/kg q 8 wks. Loss of response.")
58
Diagnostic evaluation
Fistula Fistula Diagnostic evaluation Fistula type Not superficial Superficial Antibiotics Consider fistulotomy Seton Antibiotics 6-MP/AZA ± infliximab Failure Tacrolimus Failure Evaluation of fistulas begins with definition of anatomic course and exclusion of complicating factors such as abscess. Superficial fistulas may respond to a course of antibiotics, or to fistulotomy. Patients with more complicated fistula anatomy will likely require a combined medical and surgical approach with placement of seton. Patients who do not respond to antibiotics or 6MP/azathioprine may be tried on infliximab, with maintenance using the agent that led to fistula response. Tacrolimus may be effective in closing fistulas, but also has a high rate of adverse effects in association with its use. Ultimately, some patients will fail to respond to all best efforts and may require surgery, including possible proctectomy and permanent stoma. Failure Observe Definitive surgery Failure Maintain 6-MP/AZA and/or infliximab

Similar presentations