Download presentation
Presentation is loading. Please wait.

1
Population Screening for Colorectal Cancer - update of evidences
Dr Jennifer Lee PYNEH

3
Screening – the principles
World Health Organization Criteria Important common health problem Natural history of disease adequately understood and there is asymptomatic early disease stage Treatment available Diagnostic tool available Cost-effective and competent follow-up programs available

4
Important common health problem ?
3rd commonest cancer in US 3rd leading cause of cancer death in both men and women in the US Incidence: Male: 57.2/100, 000 population Female: 42.5/100,000 population American Cancer Society

5
Colorectal Cancer in Hong Kong
Incidence: Male: 47.1/100, 000 population Female: 31.0/100,000 population (Hong Kong Cancer Registry )
")
6
Prognosis 5 year survival:
90% if disease diagnosed while still localized 68% for regional disease 10% if distant metastasis present

7
Natural history of disease : Pathogenesis
Journal of InternalMedicine 270; 87–98

8
Screening modalities

9
Screening Modalities Stool based Faecal Occult Blood Test
Faecal Immunochemical Test Stool DNA Structural Exam Flexible sigmoidoscopy Colonoscopy Double contrast Barium Enema CT colonography Colon capsule endoscopy

10
Sensitivity Evidence Recommendation Faecal Occult Blood 37.1% – 79.4% RCT proven Mortality ↓15-33% Incidence ↓20% Annually screening Faecal Immunochemical test 81% - 94% Stool DNA 52%-91% ? Barium Enema Cancer: 85-97% Adenoma>1cm: ~48% 5 years* Barium enema: not recommended by Asia Pacific Working Group

11
Flexible sigmoidoscopy
Evaluates rectum, sigmoid colon, descending colon Does not require sedation /full bowel preparation Shorter procedural time Can be done by trained nurse/physician assistants Cost: ~ USD 244

12
Colonoscopy Gold standard for diagnosis
Requires bowel preparation and sedation Potential risk of perforation and post-polypectomy bleeding Cost: ~USD 450 Efficacy: No prospective, RCT of screening colonoscopy for incidence/ mortality reduction Indirect evidence of incidence reduction in RCT of other screening test

13
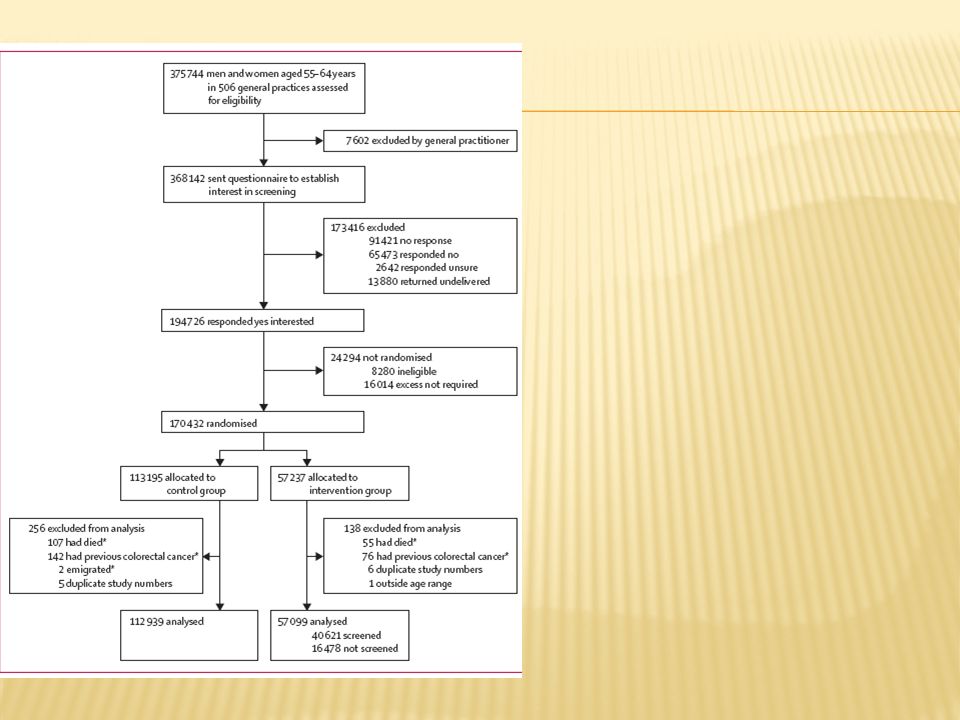
170,432 individuals aged 55-64 randomized
No family history / colonic workup within 3 years / no bowel symptoms Intervention group ( 57,237 ) vs controlled group (NO screening) (113,195) 71% (40,674) had flexible sigmoidoscopy done 5% referred for full colonoscopy due to high risk neoplasms Participants flagged in national health registry for causes of death and colorectal cancer diagnoses Follow up period: 11 years Lancet 2010; 375: >1cm 3 or more adenomas Severe dysplasia / villous type >20 hyperplastic polyps at distal colon
 vs controlled group (NO screening) (113,195) 71% (40,674) had flexible sigmoidoscopy done. 5% referred for full colonoscopy due to high risk neoplasms. Participants flagged in national health registry for causes of death and colorectal cancer diagnoses. Follow up period: 11 years. Lancet 2010; 375: >1cm. 3 or more adenomas. Severe dysplasia / villous type. >20 hyperplastic polyps at distal colon.")
14
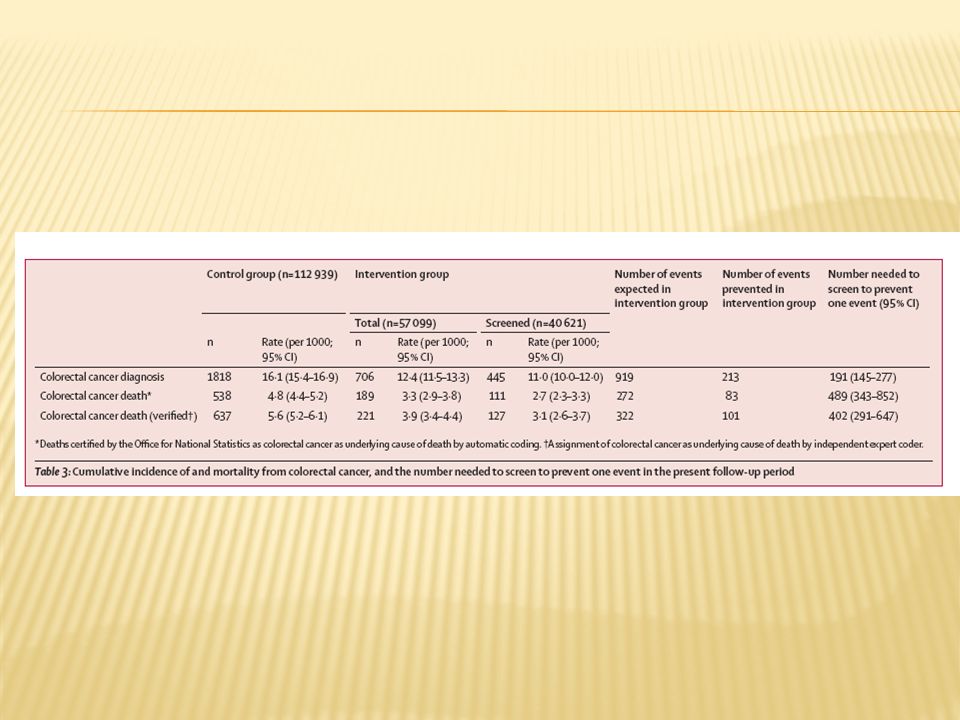
Colorectal cancer detection rate: 3.5 / 1000 screened
All distal neoplasia (adenoma/cancer) 12% of screening group In intention-to-treat analyses, colorectal cancer incidence in the intervention group was reduced by 23% and mortality by 31% 23% of patients who had colonoscopy has proximal polyps 5% advanced proximal adenomas 0.4% proximal cancers No significant effect on incidence of proximal colon cancers
 12% of screening group. In intention-to-treat analyses, colorectal cancer incidence in the intervention group was reduced by 23% and mortality by 31% 23% of patients who had colonoscopy has proximal polyps. 5% advanced proximal adenomas. 0.4% proximal cancers. No significant effect on incidence of proximal colon cancers.")
15
Is this UK study applicable to Hong Kong?

16
Difference between east & west?
Figures comparing 3 Caucasian populations studies VS 5 studies from Asian populations and Australia Asia West Polyps Proximal 30% 49% Distal 57% Synchrounous 13% 2% Advanced Neoplasia 29% 35% 52% 59% Synchronous 19% 6% Sung et al, Gut 2008;57:1166–1176

17
5464 colonoscopy performed; Mean age: 55.0 +/-15.5 year
Advanced neoplasm found in 512 patients (9.4%) Carcinoma found in 322 patients (5.9%) majority of colonic neoplasms are in distal colon advanced neoplasm (65.1%) ; Cancer (71.1%) Similar to western figures Volume 64, No. 5 : 2006 GASTROINTESTINAL ENDOSCOPY
 Carcinoma found in 322 patients (5.9%) majority of colonic neoplasms are in distal colon. advanced neoplasm (65.1%) ; Cancer (71.1%) Similar to western figures. Volume 64, No. 5 : 2006 GASTROINTESTINAL ENDOSCOPY.")
18
What are we missing? 2.2% of patients with advanced proximal neoplasm (including 1% cancer) will be missed by flexible sigmoidoscopy alone 61% of patients with advanced proximal lesions had no colonic neoplasm in the distal colon

19
Taiwan asymptomatic Chinese 1708 total colonoscopy performed
263 (15.4%) had colorectal neoplasia; 51 (3.0%) had advanced lesions 125 (37.8%) were proximal in location Two thirds (66.7%) of patients with proximal advanced lesions had no distal lesion 1.8% of subjects without distal neoplasm had proximal advanced neoplasm proportion of patients with proximal or proximal plus distal lesions increased with age (Volume 61, No. 4 : 2005 GASTROINTESTINAL ENDOSCOPY)
 had colorectal neoplasia; 51 (3.0%) had advanced lesions. 125 (37.8%) were proximal in location. Two thirds (66.7%) of patients with proximal advanced lesions had no distal lesion. 1.8% of subjects without distal neoplasm had proximal advanced neoplasm. proportion of patients with proximal or proximal plus distal lesions increased with age. (Volume 61, No. 4 : 2005 GASTROINTESTINAL ENDOSCOPY)")
20
Bleeding post- sigmoidoscopy: Bleeding post colonoscopy:
Perforations: 1/ flexible sigmoidoscopy 4/2377 colonoscopy All after snare polypectomy 3 required surgery Bleeding post- sigmoidoscopy: 12 (8 after polypectomy); 1 required surgical treatment Bleeding post colonoscopy: 9 (all after polypectomy)
; 1 required surgical treatment. Bleeding post colonoscopy: 9 (all after polypectomy)")
21
Post-polypectomy bleeding local data
Single center 5593 colonoscopy case reviewed Polypecotomy done in 1657 cases Risk of post-polypectomy bleeding ~ 2.2% Hui AJ et. Al Gastrointest Endo 2004, 59(1):44-48
:")
22
What to choose? Colonoscopy Flexible Sigmoidoscopy
Evaluates whole colon Longer procedural time Full bowel preparation Cost Potential complication related to sedation , polypectomy Flexible Sigmoidoscopy Shorter procedural time No full bowel preparation No sedation Lower cost Lower complication rate More acceptable May miss proximal lesions

23
Current recommendation in Hong Kong
2010 Recommendation on CRC screening by Cancer Expert Working Group Screening to be considered in individuals aged 50 to 75 with average risk Annual/ biennial FOBT FS every 5 years Colonoscopy every 10 years

25
CT colonography (Virtual colonoscopy)
2D&3D images obtained by CT Rapid advancement due to newer multi-detector CT Non-invasive Cost : ~ USD 800 Efficacy: No RCT to demonstrate incidence / mortality reduction Sensitivity for large polyps >1cm: ~ 85-93% Small polyps (6-9mm): ~70-86% Sensitivity for invasive cancer: 96% Eur Radiol (2012) 22:1495–1503 Margriet C. de Haan et al.
: ~70-86% Sensitivity for invasive cancer: 96% Eur Radiol (2012) 22:1495–1503 Margriet C. de Haan et al.")
26
CT colonography higher diagnostic yield per 100 invitees than primary gFOBT and FIT screening similar yield as sigmoidoscopy and colonoscopy screening Not therapeutic per-patient false-positive rates: polyps >6mm : 3.6% polyps >10-mm : 2.1% Cost-effectiveness unknown ?Impact of detecting extracolonic disease Colonoscopy to be offered if largest polyp detected >6mm Recommended for individuals who decline colonoscopy/not good candidate for colonoscopy Patients with false-positive findings were those who were sent for OC and had findings of a nonadenomatous (hyperplastic or mucosal) polyp or had a polyp that was not seen. Margriet C. de Haan et al. Eur Radiol (2012) 22:1495–1503 David H. Kim , et al. Radiology(2012),254,
 polyp or had a polyp that was not seen. Margriet C. de Haan et al. Eur Radiol (2012) 22:1495–1503. David H. Kim , et al. Radiology(2012),254,")
27
Colon capsule endoscopy
No need for sedation / air insufflation / radiation exposure NOT therapeutic Cost: ~USD 950 Results affected by Bowel preparation Colonic transit time Battery life

28
Colon capsule endoscopy
Sensitivity Specificity Gossum, et al Polyps >6mm 64% 84% Advanced adenoma 73% 79% Rokkas, et al Meta-analysis 626 CCE Significant polyps (size >6mm / no.>3) 69% 86% All polyps 89% Sensitivity for cancer : 74% Polyp and cancer pick up rate: inferior than colonoscopy False positive rate: 33% Future improvement ? Rokkas: A total of 626 individuals were included in this meta-analysis. Gossum, et al, N Engl J Med 2009;361:264-70 Rokkas, et al, Gastrointest Endosc 2010;71:792-8
 69% 86% All polyps. 89% Sensitivity for cancer : 74% Polyp and cancer pick up rate: inferior than colonoscopy. False positive rate: 33% Future improvement Rokkas: A total of 626 individuals were included in this meta-analysis. Gossum, et al, N Engl J Med 2009;361: Rokkas, et al, Gastrointest Endosc 2010;71:")
29
Summary Colorectal cancer screening is important
Recent large scale population randomised study in UK suggest flexible sigmoidoscopy is effective for screening However ~2% proximal lesions may be missed Newer modalities such as CT colonography and colon capsule endoscopy is a viable alternative, but needs further evaluation for effectiveness as screening tool

30
Thank you

31
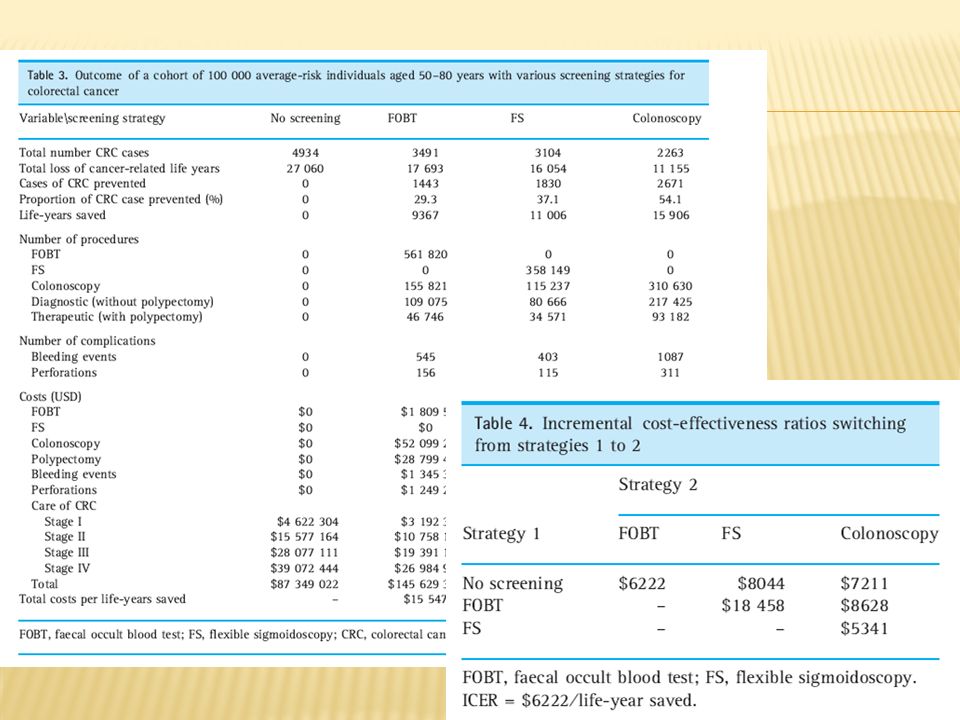
Cost-effectiveness of screening
Hypothetical population of 100, 000 population for screening annual FOB / 5 yearly FS / 10 yearly Colonoscopy Screening at age 50 until 80 Cost of treatment including chemotherapy calculated incremental cost-effectiveness ratio (Cost per life year saved) Aliment Pharmacol Ther 28, 353–363
 Aliment Pharmacol Ther 28, 353–363.")
33
Flexible sigmoidoscopy
UK trial: longeset period FU, 11 years Norwegian Colorectal Cancer Prevention (NORCCAP) trial , inter-rim report 6 years Reduce mortality only, no observaed reduced incidence so far (since early peak of screening detected cancer) Populations study Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening trial in the USA Italian Screening COlon REtto (SCORE): follow UK protocol
 trial , inter-rim report 6 years. Reduce mortality only, no observaed reduced incidence so far (since early peak of screening detected cancer) Populations study. Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening trial in the USA. Italian Screening COlon REtto (SCORE): follow UK protocol.")
34
Colonoscopy Primary screening colonoscopy: Poland, Germany
Randomized trials for screening colonoscopy: Spanish trial, 55 000 individuals between 50 and 69 years of age are being randomly assigned to either iFOBT or colonoscopy final results are expected in 2021 after 10 years of follow-up Nordic–European Initiative on Colorectal Cancer (NordICC) is a multicentre, multinational randomisied trial 66 000 individuals are randomly assigned to either colonoscopy or no screening Planned 15-year follow-up an interim analysis after 10 years due around 2022
 is a multicentre, multinational randomisied trial individuals are randomly assigned to either colonoscopy or no screening. Planned 15-year follow-up. an interim analysis after 10 years due around")
35
Referal for colonoscopy
High-risk criteria: 1 cm or larger three or more adenoma tubulovillous or villous histology severe dysplasia or malignant disease 20 or more hyperplastic polyps above the distal rectum

Similar presentations