Download presentation
Presentation is loading. Please wait.

1
Eyelid Trauma A-R Zandi MD Farabi eye hospital

2
Eyelid Trauma Careful history VA Globe and orbit evaluation Imaging Primary repair

3
Blunt Trauma Ecchymosis and edema Indirect funduscopy CT ( Orbital fracture )
")
4
Penetrating Trauma Laceration not involving the eyelid margin Laceration involving the eyelid margin

5
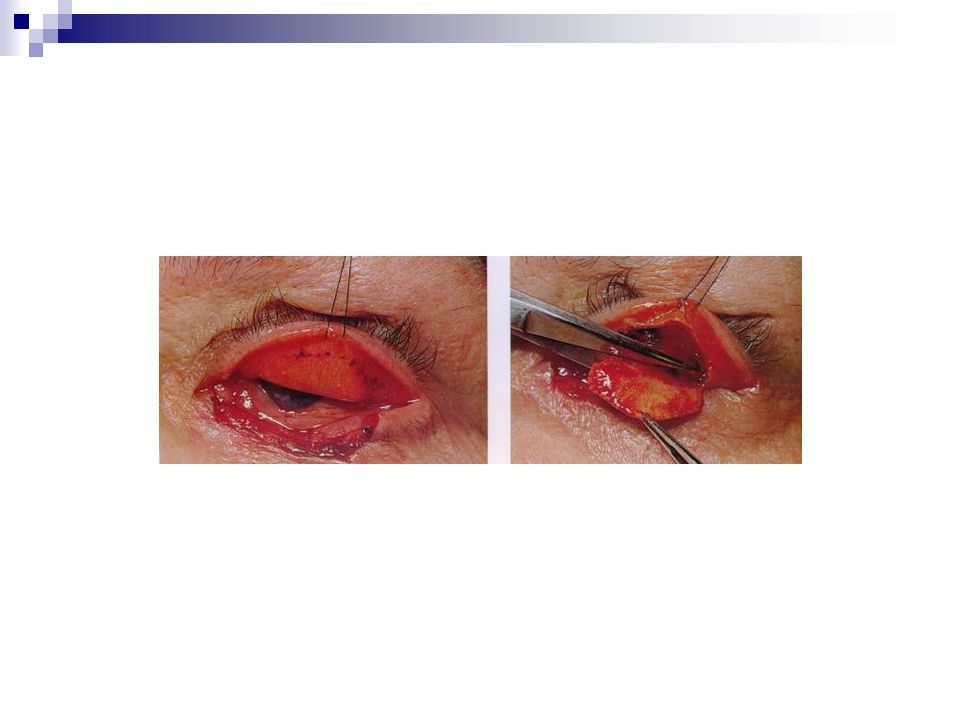
Laceration not involving the eyelid margin Skin suture

6
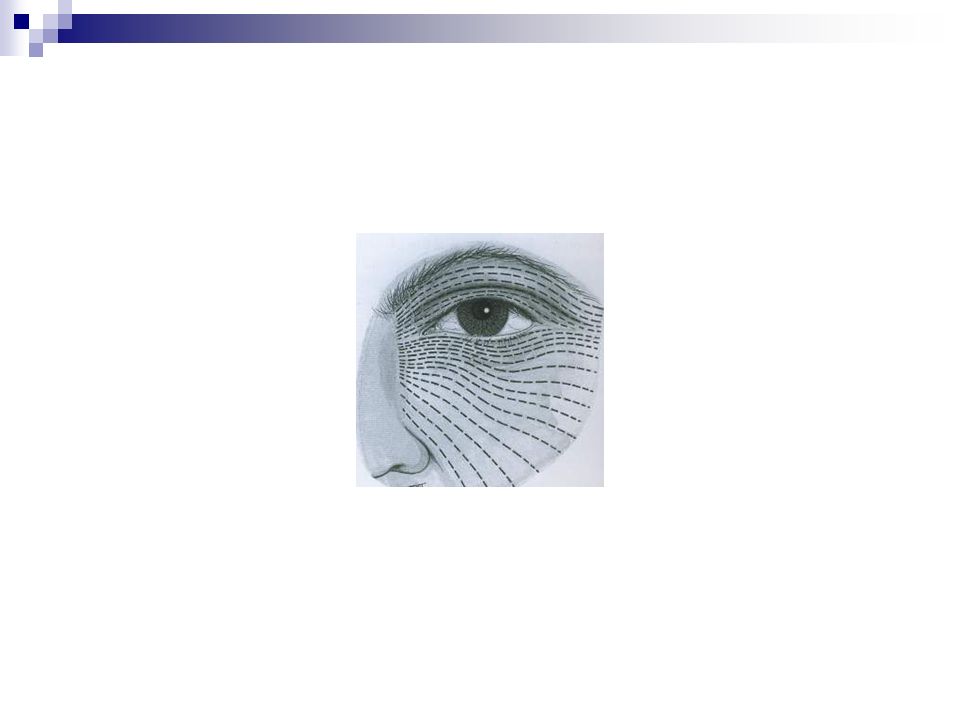
Eyelid skin suture Preparation Do wound cleaning Do not tissue debridment Regard relaxed skin tension lines Repair deep tissue first with Vicryl 6--0 Align anatomic landmarks Small caliber suture with Nylon6-0 Maximize horizontal tension and minimize vertical tension Eversion of the wound edge Early suture removal(5 days)
")
8
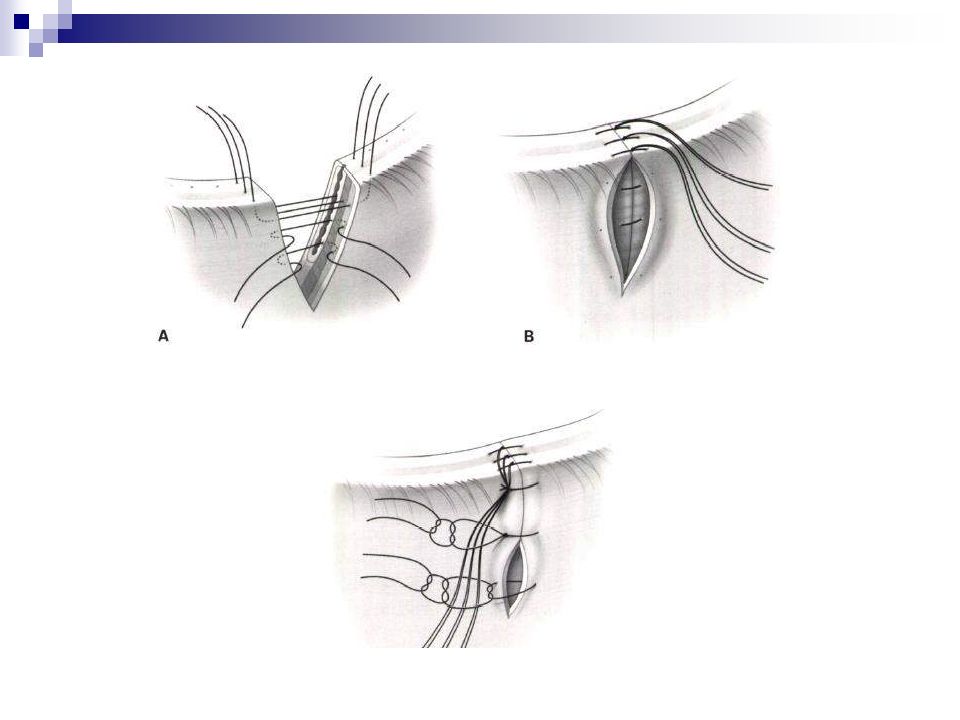
In the upper eyelid tarsus should be repaired with partial thickness bite and in the lower eyelid with full thickness bite

9
Orbital fat prolapse means that the septum has been violated - FB should be searched - Levator exploration - Globe and optic nerve - Orbital hemorrhage and infection

10
Orbital septum lacerations should not be sutured ( possible vertical Shortening )
")
11
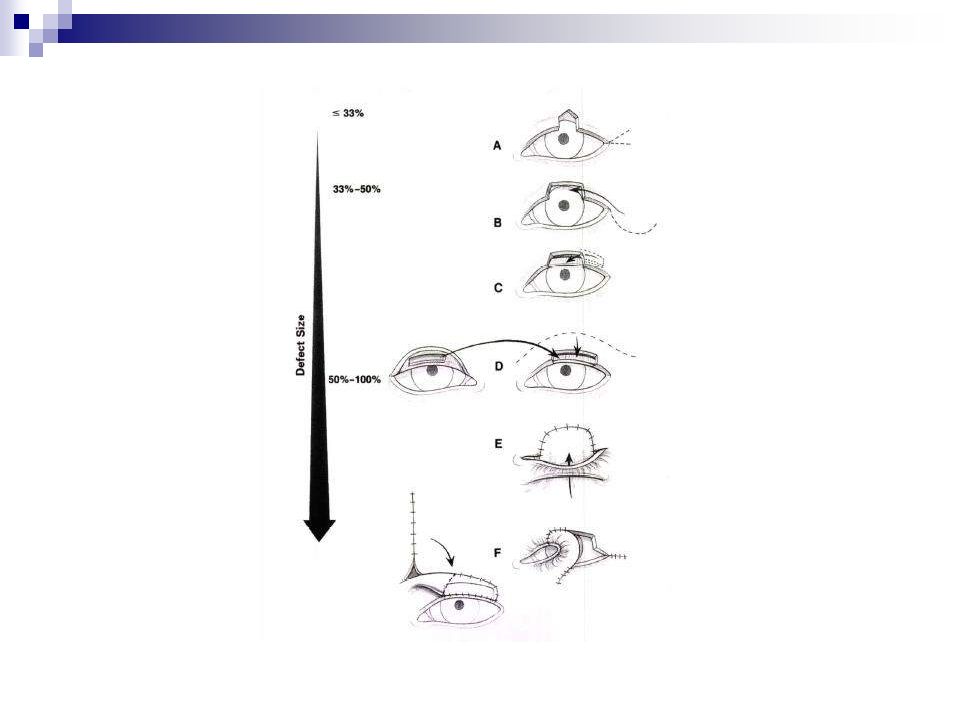
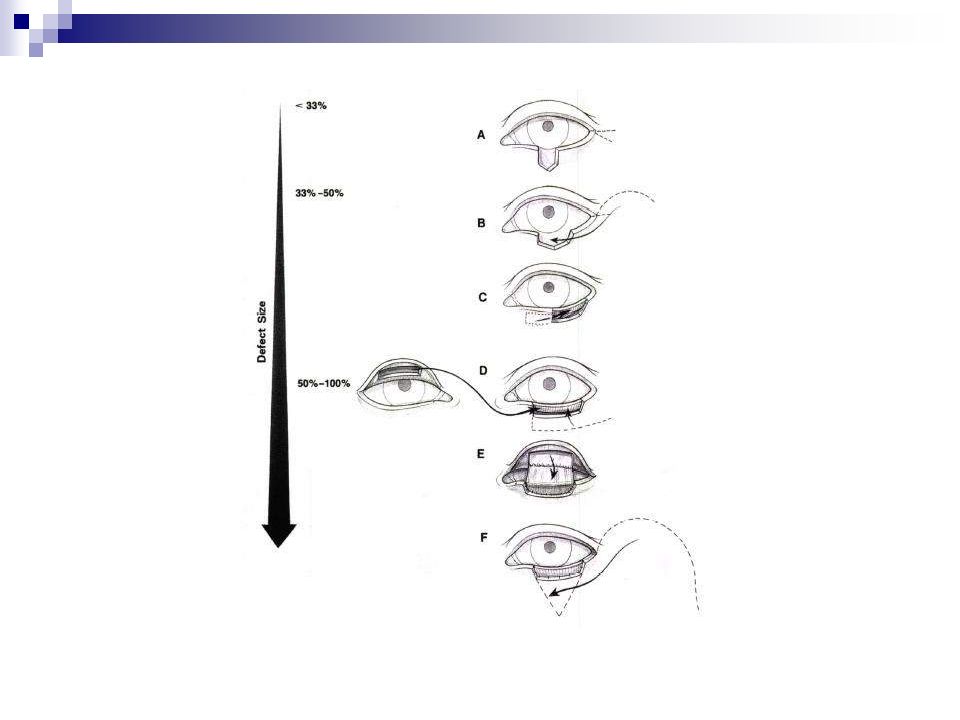
Lacerations involving the eyelid margin

13
Lacerations in the medial canthal erea demand evaluation of the lacrimal drainage apparatus

14
Diagnostic canalicular probing and irrigation may be helpful

15
Most of the canalicular laceration occurs when the lid is pulled laterally

16
Some clinicians consider the repair of single canalicular laceration optional

17
Some authors have suggested - Upper canalicular laceration do not need to be repaired - Marsupialization of a canaliculus in to the conj sac may be acceptable

18
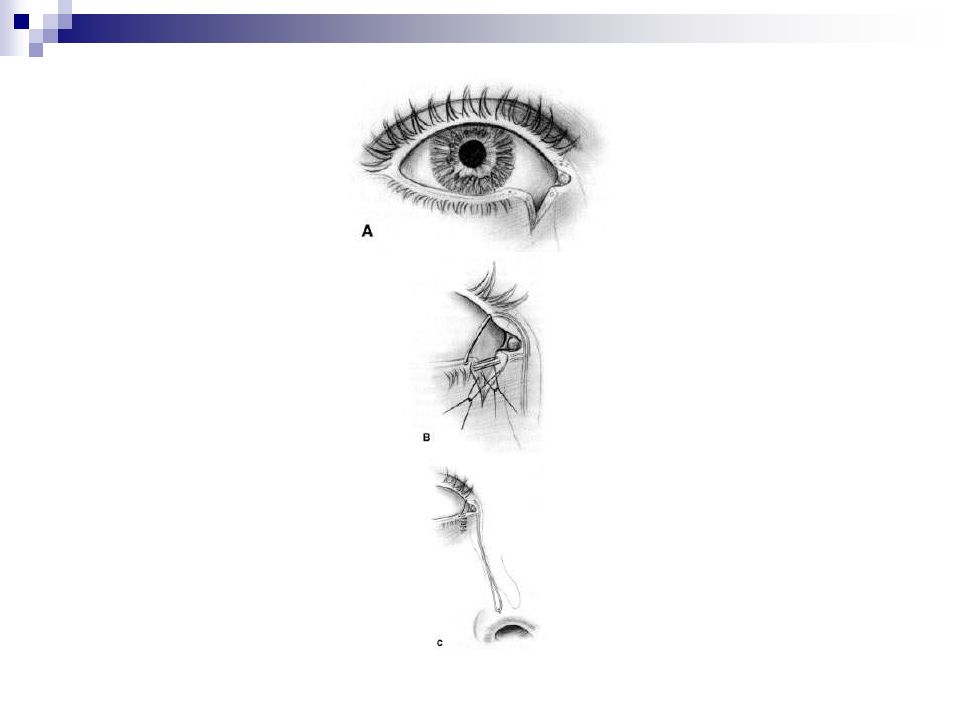
Most surgeons recommend repair of all canaliculus laceration by lacrimal intubation

19
The first step of the repair is locating the severed ends of the canaliculus system

20
It is easier to see the distal end of the lacerated canaliculus by delaying repair for 12-24 hours

21
This structure appears as an flattened oval with pearly gray shining rulled edges

22
Irrigation using air- flurscein- yellow viscoelastic through an intact canaliculus may be helpful

23
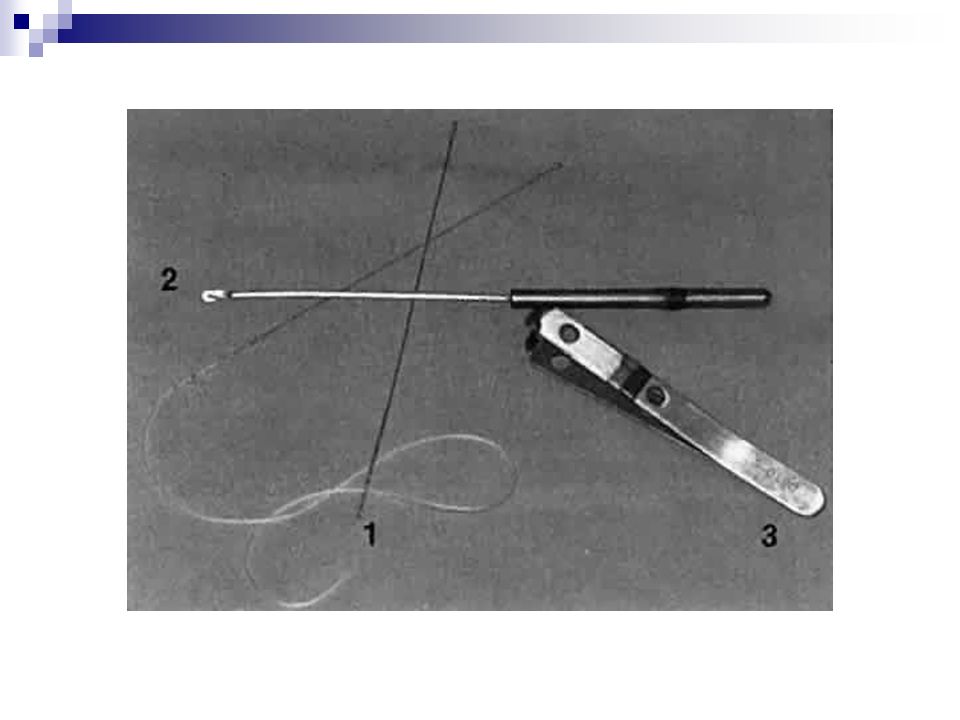
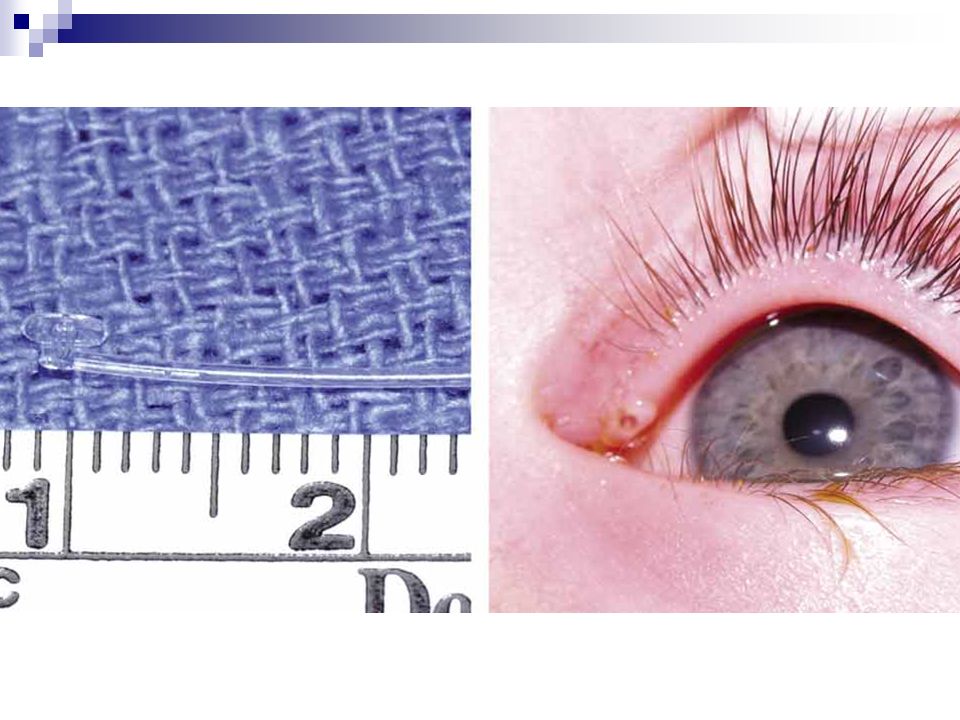
Traditionally bicanalicular stent have been used but monocanalicular stents are gaining popular

27
Direct anastomosis of the cut canaliculus over the silicon tube can be accomplished with closure of the pericanalicular tissues

28
Stents are usually left in place for 3 months or longer

29
Medial canthal tendon avulsion Rounding of the medial canthal angle Telecanthus

30
Treatment The avulsed limb sutured to the periostium The avulsed tendon should be wired transnasally

31
Failure to treat the canthal avulsion gives rise to cosmetic and functional problems

32
Observe the upper eyelid movement to ensure that the levator muscle has not been damaged

33
Before treatment for traumatic ptosis: The patient should be observed for 6 months

34
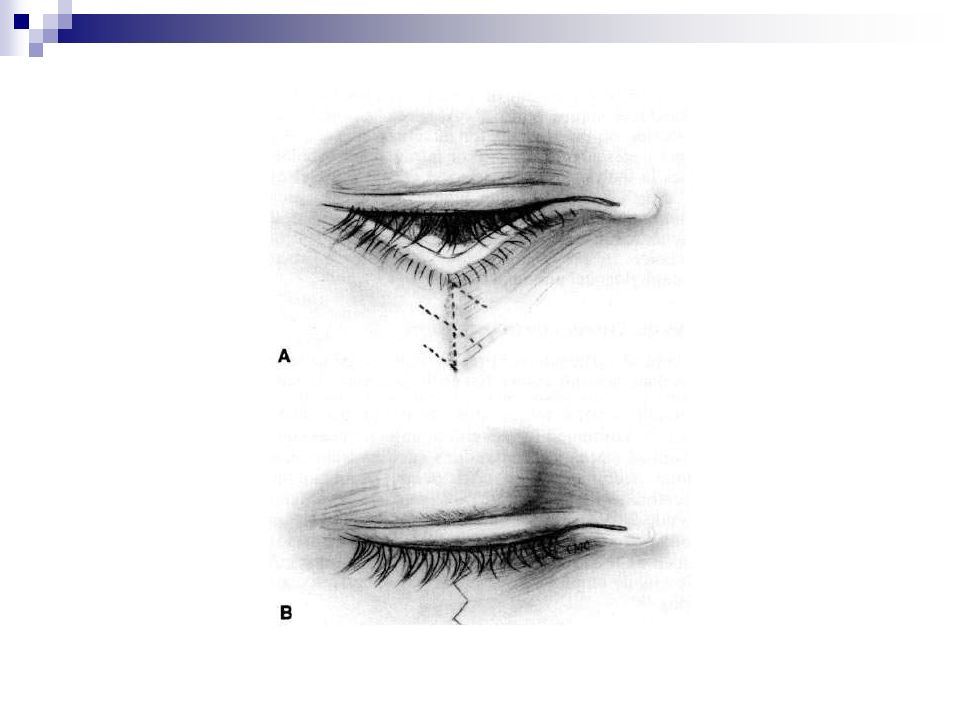
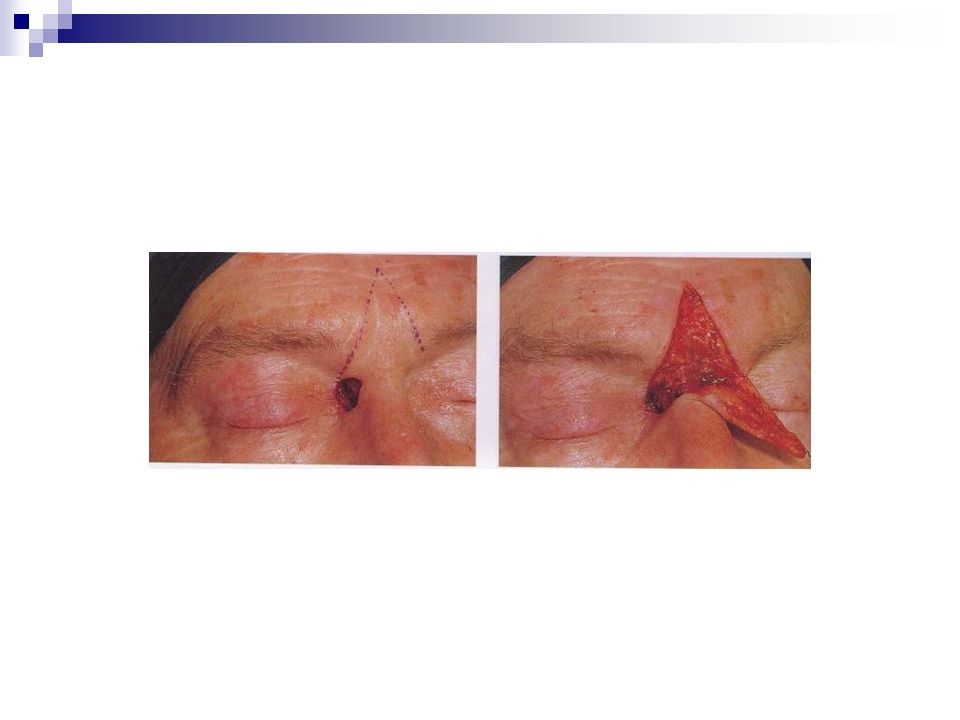
Secondary repair Treatment of cicatricial changes from… Initial Trauma Surgical repair

35
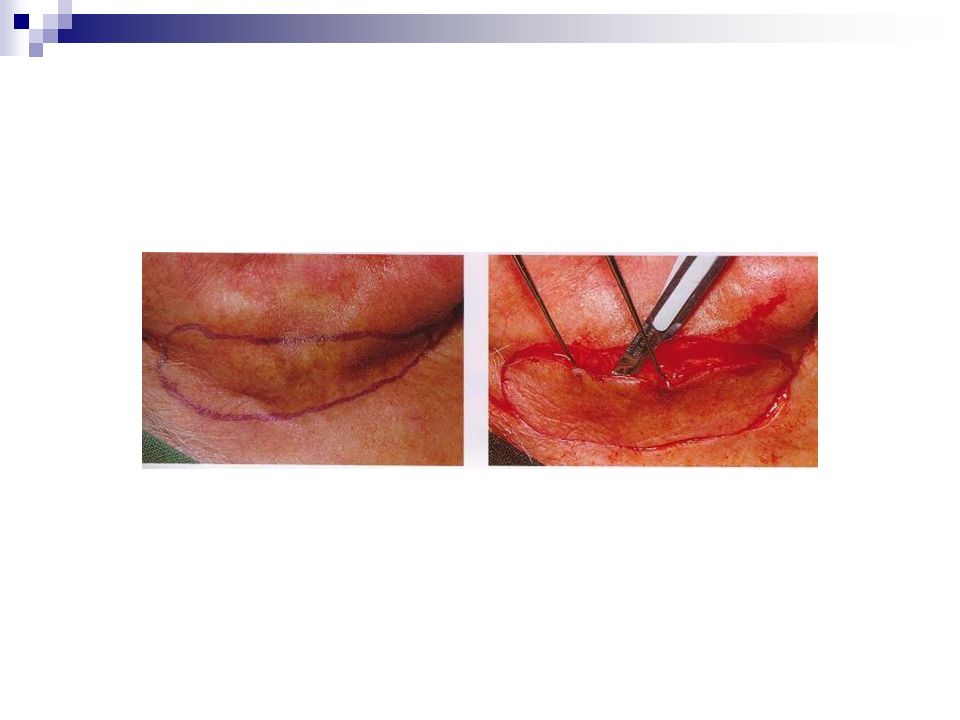
An elliptical excision Z-plasty Free skin graft Skin flap

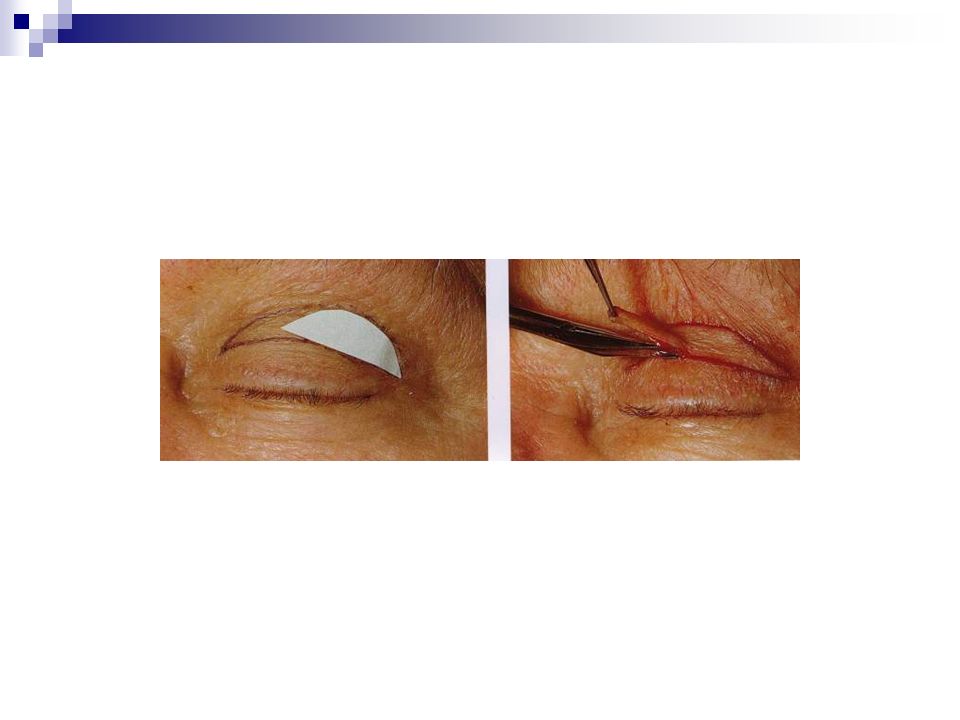
38
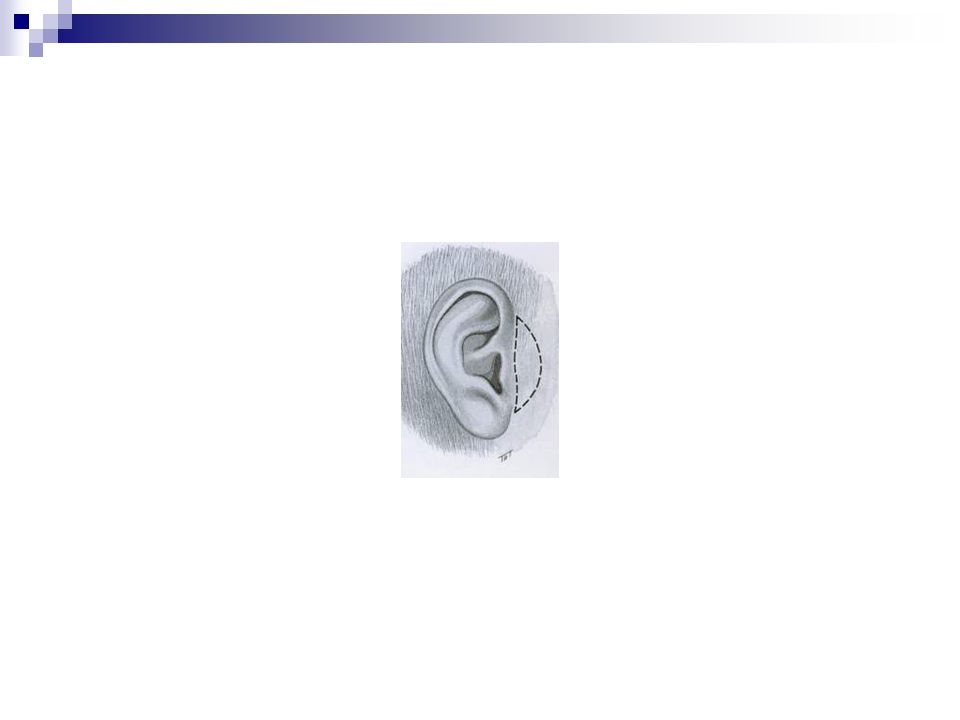
Non-hair-bearing skin Postauricular Preauricular Upper eyelid Supraclavicular Inner upper arm

42
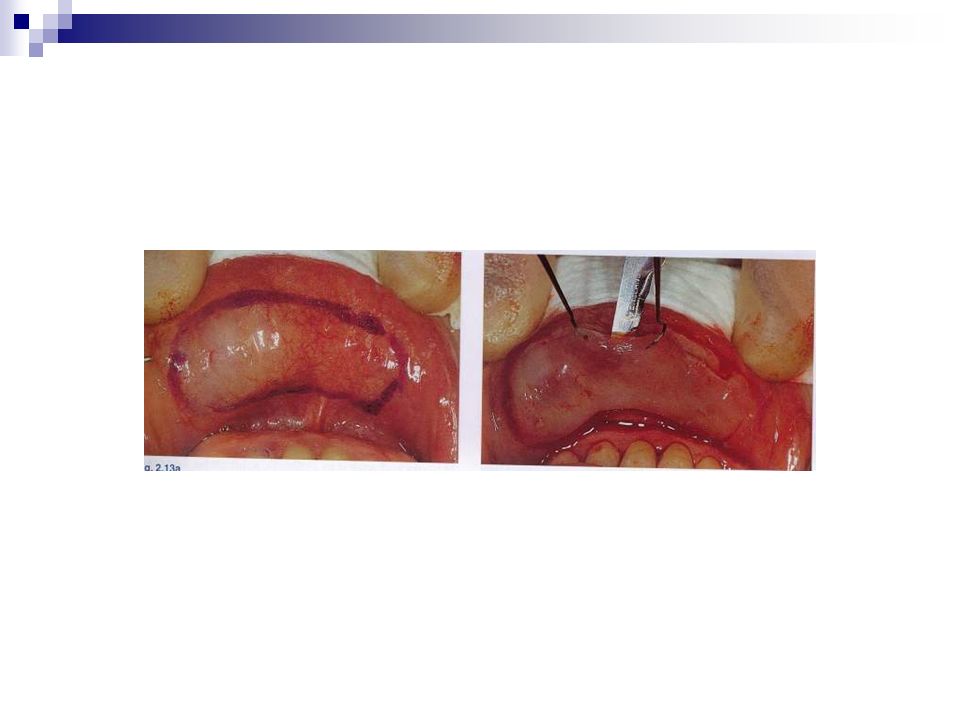
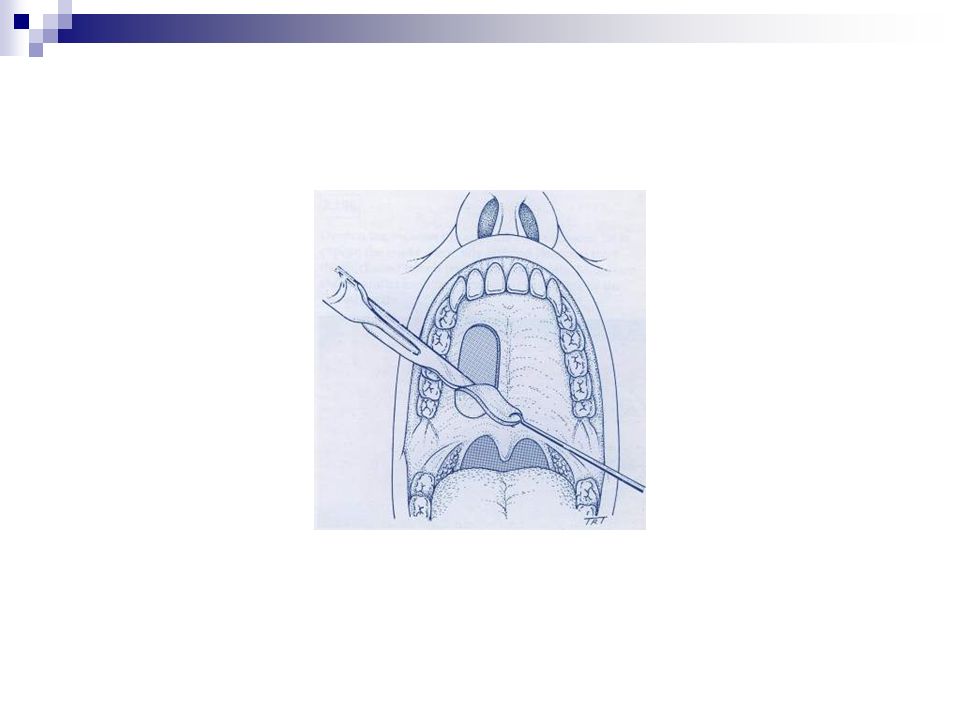
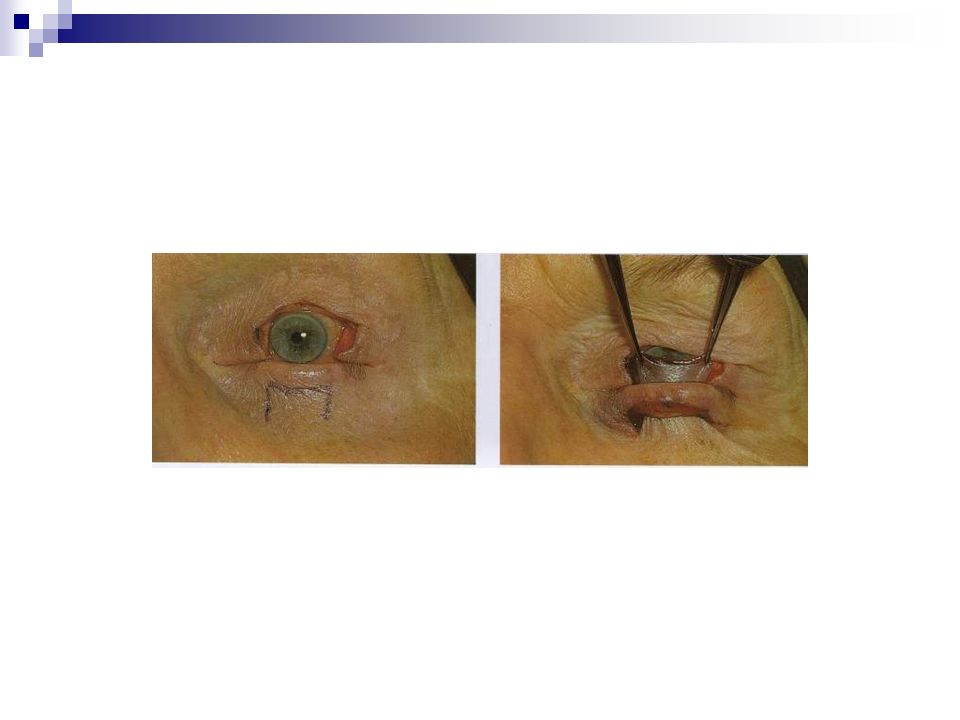
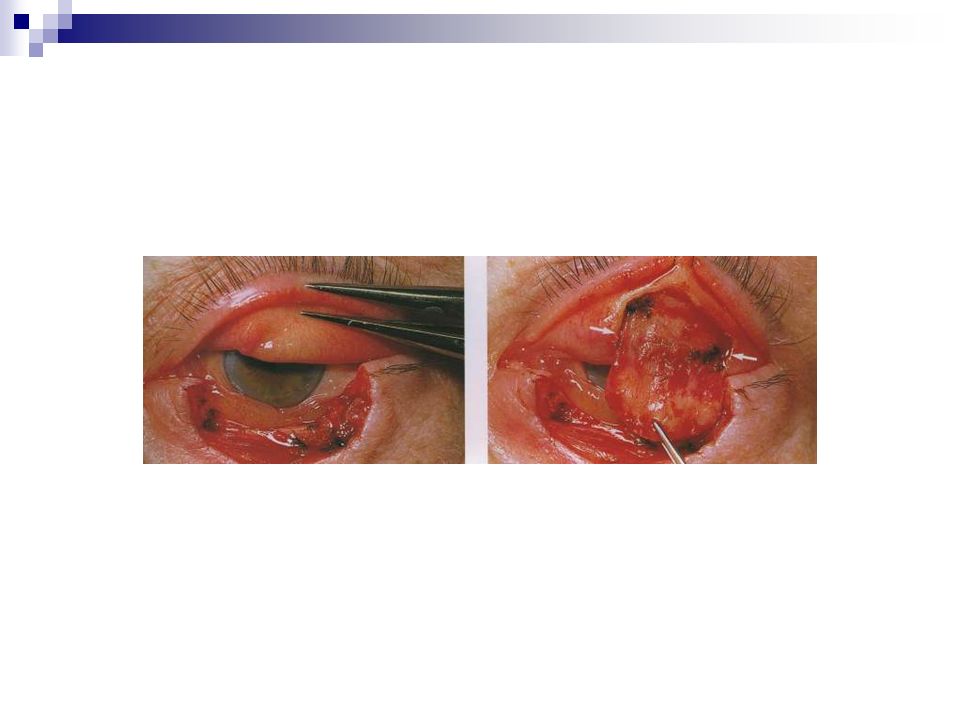
Posterior lamella Tarsoconjunctival graft Hard palate Buccal mucosa

55
One of the layers must provide the blood supply( pedicle flap )
")
Similar presentations




Extension of traumatized wound to allow identification of zone of injury 2)Detection & removal of foreign material, especially.>")


>")














