Download presentation
Presentation is loading. Please wait.

2
Preventing Stroke in Primary Care Clinical recommendations from the Alberta Provincial Stroke Strategy

3
Learning Objectives Upon completion of this program, participants will be able to: Upon completion of this program, participants will be able to: Discuss the incidence of stroke and the risk of recurrent stroke Discuss the incidence of stroke and the risk of recurrent stroke Describe four components of secondary stroke prevention Describe four components of secondary stroke prevention Identify high risk TIA/stroke patients along with the appropriate care and investigations Identify high risk TIA/stroke patients along with the appropriate care and investigations Explain strategies to reduce the risk of recurrent stroke Explain strategies to reduce the risk of recurrent stroke

4
Stroke: The Canadian Perspective 50,000 new stroke patients/year in Canada † 1 stroke every 10 minutes 5000 new strokes / year in Alberta 200,000–300,000 stroke survivors in Canada † 35-40,000 stroke survivors in Alberta Cost to Alberta Health over $300 million / year

5
Stroke: The Canadian Perspective 4th leading cause of death in Canada The leading cause of adult disability 28% of stroke patients are under age 65*

6
Stroke Subtypes Ischemic 80% Hemorrhagic 20%

7
Athero-thrombosis: a progressive process Normal Fatty streak Fibrous plaque Athero- sclerotic plaque Plaque rupture/ fissure & thrombosis Myocardial infarction Ischaemic stroke Critical leg ischaemia Clinically silent Cardiovascular death Increasing age Angina Transient ischaemic attack Claudication/PAD

8
Recurrence of Ischemic Stroke From Petty GW et al. Stroke 2000;31:1062-68 †Not significant; all other categories statistically different across subtype of stroke. Outcomes for Patients With a First Ischemic Stroke (by subtype)
.")
9
Second Strokes Stroke or TIA survivors have an increased risk of a subsequent stroke Stroke or TIA survivors have an increased risk of a subsequent stroke Recurrent strokes are more likely than initial strokes to result in disability and death Recurrent strokes are more likely than initial strokes to result in disability and death ~ 20%-40% of strokes are preceded by a TIA or non disabling stroke ~ 20%-40% of strokes are preceded by a TIA or non disabling stroke (Rothwell et al. Lancet Neurol 2006; 5: 323-331) Golden Opportunity for Stroke Prevention!
 Golden Opportunity for Stroke Prevention!.")
10
TIA Stroke Risk Risk of stroke following TIA is high: 10-20% within 90 days 10-20% within 90 days 50% of these within the first 2 days (48 hours) 50% of these within the first 2 days (48 hours) Johnston et al. JAMA 2000; 284: 2901-06 EARLY PREVENTION STRATEGIES can make a difference! ACT FAST!

12
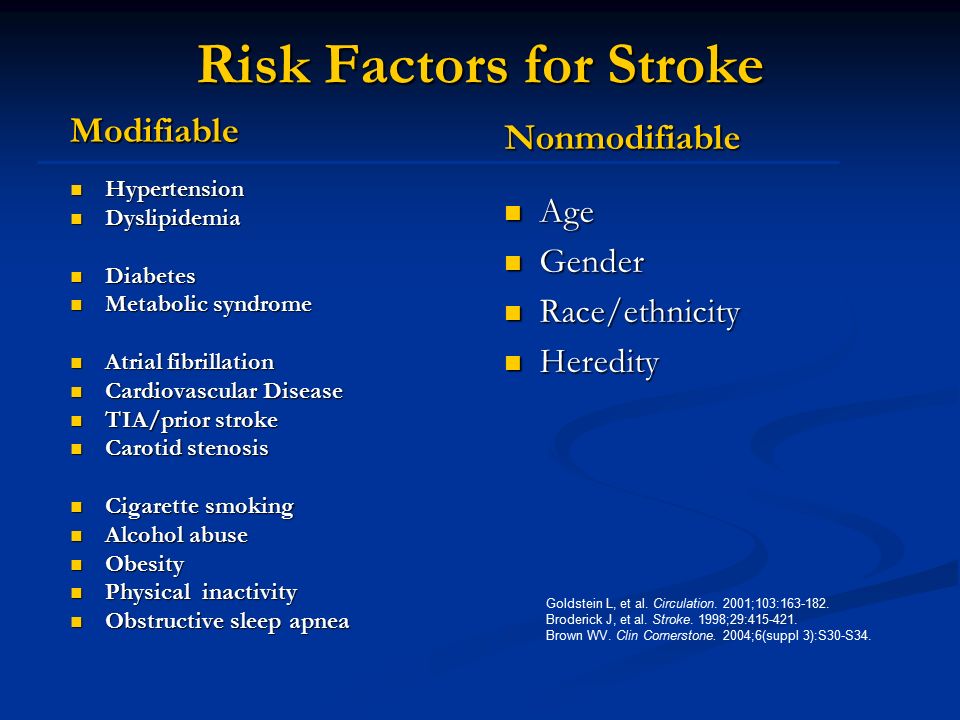
Modifiable Hypertension Hypertension Dyslipidemia Dyslipidemia Diabetes Diabetes Metabolic syndrome Metabolic syndrome Atrial fibrillation Atrial fibrillation Cardiovascular Disease Cardiovascular Disease TIA/prior stroke TIA/prior stroke Carotid stenosis Carotid stenosis Cigarette smoking Cigarette smoking Alcohol abuse Alcohol abuse Obesity Obesity Physical inactivity Physical inactivity Obstructive sleep apnea Obstructive sleep apnea Nonmodifiable Age Gender Race/ethnicity Heredity Goldstein L, et al. Circulation. 2001;103:163-182. Broderick J, et al. Stroke. 1998;29:415-421. Brown WV. Clin Cornerstone. 2004;6(suppl 3):S30-S34. Risk Factors for Stroke
:S30-S34. Risk Factors for Stroke.")
13
Approach to Secondary Stroke Prevention Components: Evaluate the Event Evaluate the Event Implement Interventions Implement Interventions Initiate Medications Initiate Medications Modify Stroke Risk Factor: Continuous Monitoring Modify Stroke Risk Factor: Continuous Monitoring

14
Evaluate the Event

15
ABCD 2 Score Rothwell et al. Lancet; 2007; 369: 283-292 Yes No Age 60 yrs 1 0 Bp 140/90 1 0 Clinical Features Unilateral weakness 2 0 (with or without speech disturbance) Speech deficit without weakness 1 0 Duration > 10 min < 59 min 1 0 60 min 2 0 Diabetes 1 0 Score 4 = High Risk
 Speech deficit without weakness 1 0 Duration > 10 min < 59 min 1 0 60 min 2 0 Diabetes 1 0 Score 4 = High Risk.")
16
Evaluate the Event: TIA / Minor Stroke Risk Assessment TIA Stroke Risk Assessment High Risk 1. Symptom onset within the last 48 hours with any one of the following : Motor deficit lasting more than 5 minutes Speech deficit lasting more than 5 minutes ABCD 2 score ≥ 4 2. Atrial fibrillation with TIA

17
Evaluate the Event: TIA / Minor Stroke Risk Assessment TIA Stroke Risk Assessment Medium Risk Symptom onset between 48 hours and 7 days with any one of the following : Motor deficit lasting more than 5 minutes Speech deficit lasting more than 5 minutes ABCD 2 score ≥ 4 Low Risk 1. Symptom onset > 7 days 2. Symptom onset ≤ 7 days without the presence of high risk symptoms Speech deficit, motor deficit, ABCD 2 score ≥ 4, atrial fibrillation with TIA Speech deficit, motor deficit, ABCD 2 score ≥ 4, atrial fibrillation with TIA ** Isolated syncope or dizziness is rarely a TIA and may not require Stroke Prevention Clinic Referral

19
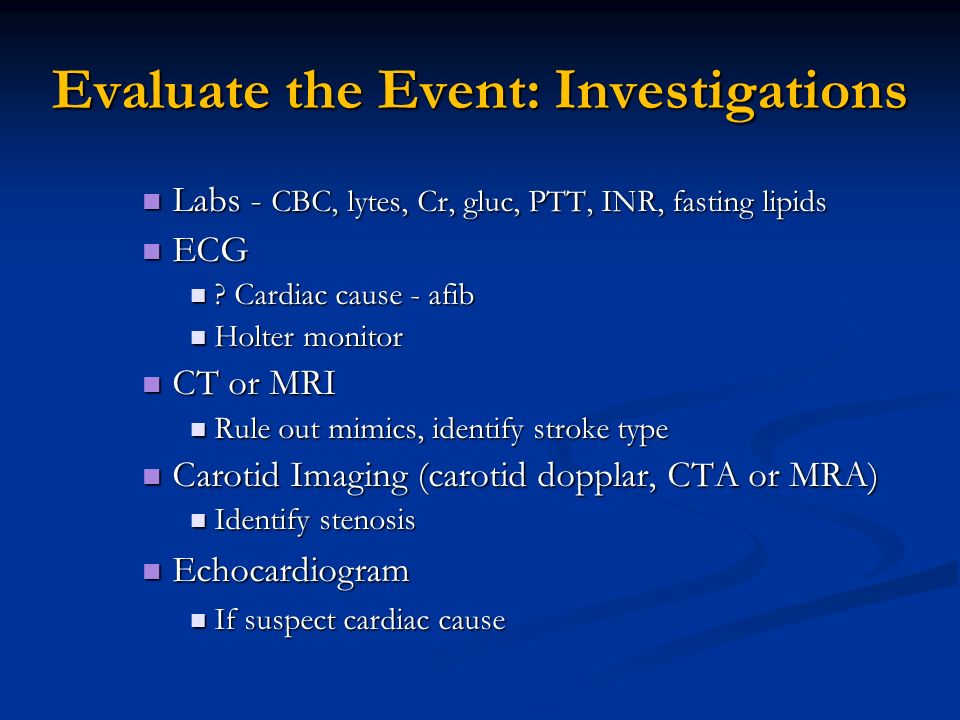
Evaluate the Event: Investigations Labs - CBC, lytes, Cr, gluc, PTT, INR, fasting lipids Labs - CBC, lytes, Cr, gluc, PTT, INR, fasting lipids ECG ECG ? Cardiac cause - afib ? Cardiac cause - afib Holter monitor Holter monitor CT or MRI CT or MRI Rule out mimics, identify stroke type Rule out mimics, identify stroke type Carotid Imaging (carotid dopplar, CTA or MRA) Carotid Imaging (carotid dopplar, CTA or MRA) Identify stenosis Identify stenosis Echocardiogram Echocardiogram If suspect cardiac cause If suspect cardiac cause
 Carotid Imaging (carotid dopplar, CTA or MRA) Identify stenosis Identify stenosis Echocardiogram Echocardiogram If suspect cardiac cause If suspect cardiac cause.")
20
IMPLEMENT INTERVENTIONS ACT FAST WITH HIGH RISK PATIENTS!

22
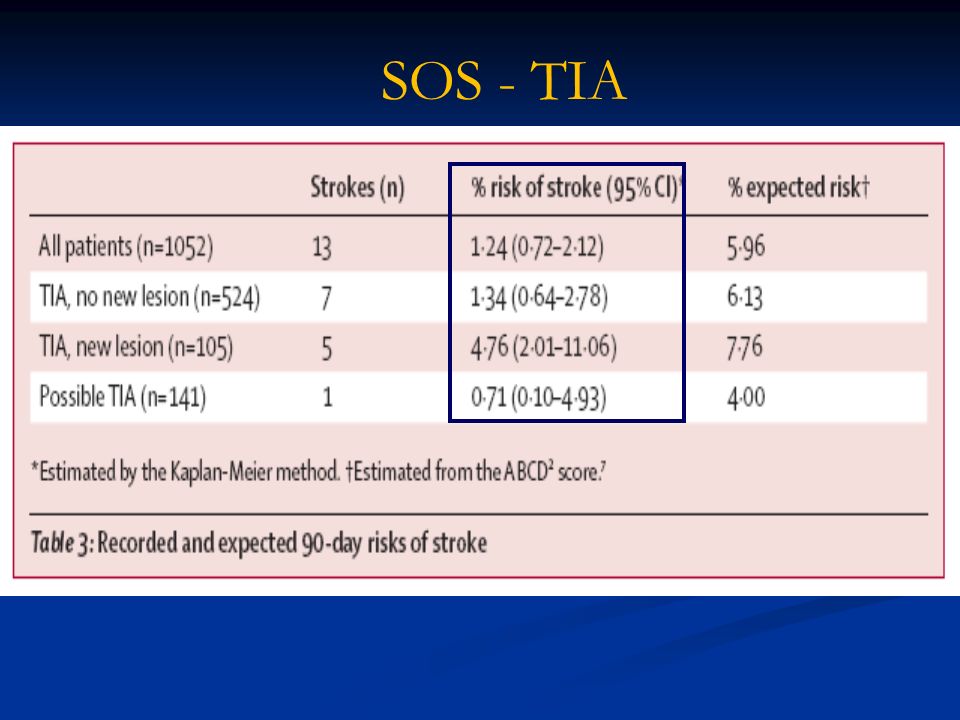
SOS - TIA

23
EXPRESS study ( UK) PHASE 1 : daily appointment clinic, advice faxed to the FP PHASE 1 : daily appointment clinic, advice faxed to the FP PHASE 2 : Emergency clinic, TIA patients seen on the same day and treatment given in clinic PHASE 2 : Emergency clinic, TIA patients seen on the same day and treatment given in clinic ASA in all cases, ASA + clopidogrel in high risk patients, simvastatin 40mg, perindopril 4mg and indapamide 1.25 mg ASA in all cases, ASA + clopidogrel in high risk patients, simvastatin 40mg, perindopril 4mg and indapamide 1.25 mg Reduction in risk of early recurrent stroke by over 80% Reduction in risk of early recurrent stroke by over 80% Rothwell et al. Lancet; 2007:370:1432-1442 Rothwell et al. Lancet; 2007:370:1432-1442

24
Express Study

25
Implement Interventions: Carotid Endarterectomy If TIA due to ≥ 50% stenosis in extracranial carotid artery consider CEA Greatest benefit if surgery within 2 weeks Rothwell et al. Lancet; 2004; 363: 915-25

26
Early Carotid Surgery Much Better >70% w/o near-occlusion Rothwell PM et al. Stroke 2004;35:2855-2861. NNT 3

28
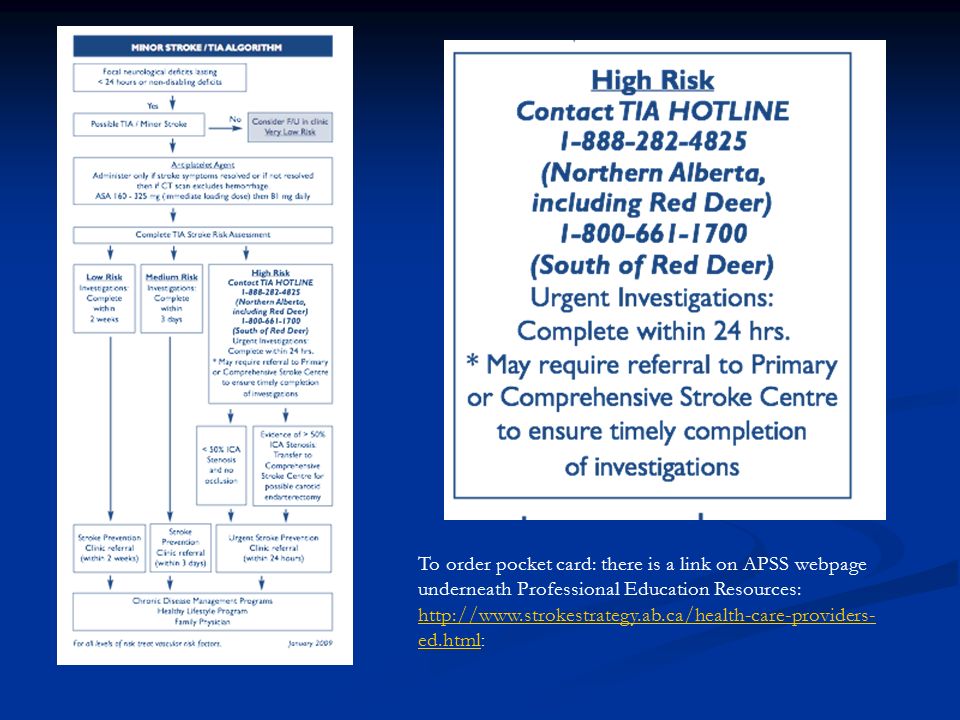
To order pocket card: there is a link on APSS webpage underneath Professional Education Resources: http://www.strokestrategy.ab.ca/health-care-providers- ed.html http://www.strokestrategy.ab.ca/health-care-providers- ed.html :

29
Initiate Medications: Antithrombotic Therapy Aspirin (50-325 mg/day) is first line treatment If aspirin naïve- load with 160mg then 81 mg OD If aspirin naïve- load with 160mg then 81 mg OD Options: Aspirin/extended release dipyridamole 25mg/200mg BID 25mg/200mg BIDClopidogrel 75 mg OD, consider loading with 300 mg 75 mg OD, consider loading with 300 mg
 is first line treatment If aspirin naïve- load with 160mg then 81 mg OD If aspirin naïve- load with 160mg then 81 mg OD Options: Aspirin/extended release dipyridamole 25mg/200mg BID 25mg/200mg BIDClopidogrel 75 mg OD, consider loading with 300 mg 75 mg OD, consider loading with 300 mg")
30
ESPS-2: The Second European Stroke Prevention Study Tested efficacy of ASA/ER DP for secondary stroke prevention Addressed clinical questions Does ER DP prevent stroke? Does ER DP prevent stroke? Does low-dose ASA prevent stroke? Does low-dose ASA prevent stroke? Is ASA/ER DP superior to ASA alone? To ER DP alone? Is ASA/ER DP superior to ASA alone? To ER DP alone? Is ASA/ER DP well tolerated? Is ASA/ER DP well tolerated? Diener HC, et al. J Neurol Sci 1997;151:S1-S77 Diener HC, et al. J Neurol Sci 1996;143:1-13

31
ESPS-2 Results: Stroke-Free Survival Kaplan-Meier stroke-free survival curves ER DP ASA/ER DP ASA Placebo Patients without stroke (%) Time (months) 80 85 90 95 100 6121824
 Time (months)")
32
Diener HC, et al. J Neurol Sci 1997;151:S1-S77 Diener HC, et al. J Neurol Sci 1996;143:1-13 ESPS-2: Conclusions Combined treatment with ER DP + ASA reduces the risk of stroke by 37% vs. placebo (p<0.001) Combined treatment with ER DP + ASA is significantly superior to ASA alone (RRR 23.1%, p<0.006) ER DP and ASA have an additive effect in secondary prevention of stroke
 Combined treatment with ER DP + ASA is significantly superior to ASA alone (RRR 23.1%, p<0.006) ER DP and ASA have an additive effect in secondary prevention of stroke.")
33
RRR: 6.4% (p=0.244) ASA+Clopidogrel Clopidogrel IS, MI, VD, rehospitalisation for acute ischaemic event Cumulative event rate 0.00 0.04 0.08 0.12 0.16 0.20 Months of follow-up 0 3 6 9121518 MATCH: ASA+Clopidogrel showed a non significant trend for the reduction in major vascular events in specific high risk cerebrovascular patients* Primary Endpoint (ITT) * All patients received clopidogrel
 ASA+Clopidogrel Clopidogrel IS, MI, VD, rehospitalisation for acute ischaemic event Cumulative event rate Months of follow-up MATCH: ASA+Clopidogrel showed a non significant trend for the reduction in major vascular events in specific high risk cerebrovascular patients* Primary Endpoint (ITT) * All patients received clopidogrel")
34
Initiate Medications: Antithrombotic Therapy If cardioembolic source: Long-term anticoagulation (Warfarin) Long-term anticoagulation (Warfarin) Target INR 2.0 – 3.0 Target INR 2.0 – 3.0
 Long-term anticoagulation (Warfarin) Target INR 2.0 – 3.0 Target INR 2.0 – 3.0")
35
Atrial Fibrillation Persistent and PAF predictors of first and recurrent strokes Persistent and PAF predictors of first and recurrent strokes Overall RR with coumadin is 68% Overall RR with coumadin is 68% Optimal INR 2-3 Optimal INR 2-3 Estimated RR with ASA compared to placebo is 21% Estimated RR with ASA compared to placebo is 21% About one-third with AF & IS will have another potential cause eg carotid stenosis About one-third with AF & IS will have another potential cause eg carotid stenosis

36
Stroke Prediction Model: CHADS Scoring Tool Risk Classification Scheme: Components of CHADS2 CHADS2 itemPoints Congestive heart failure 1 Hypertension (systolic >160 mmHg) 1 Age greater than 75 years 1 Diabetes 1 Prior cerebral ischemia 2
 1 Age greater than 75 years 1 Diabetes 1 Prior cerebral ischemia 2")
37
Antithrombotic Therapy for Patients With Atrial Fibrillation Weaker Risk Factors Moderate-Risk FactorsHigh-Risk Factors Female genderAge ≥ 75 yearsPrevious stroke /TIA or embolism Age 65 to 74 HypertensionMitral stenosis Coronary Artery DiseaseHeart FailureProsthetic heart valve Thyrotoxicosis LV ejection fraction ≤ 35% Diabetes ACC/AHA/ESC guide lines for management of AF; Circulation 2 Aug 06

38
Antithrombotic Therapy for Patients With Atrial Fibrillation Risk CategoryRecommended Therapy No risk factors ( ASR 1%) Aspirin, 81 to 325 mg daily One moderate-risk factor (ASR 4%) Aspirin, or warfarin Any high-risk factor or more than 1 warfarin moderate-risk factor (ASR 8-12%) ACC/AHA/ESC guide lines for management of AF; Circulation 2 Aug 06
 Aspirin, 81 to 325 mg daily One moderate-risk factor (ASR 4%) Aspirin, or warfarin Any high-risk factor or more than 1 warfarin moderate-risk factor (ASR 8-12%) ACC/AHA/ESC guide lines for management of AF; Circulation 2 Aug 06")
39
Modifiable Stroke Risk Factors Medical conditions Hypertension Hypercholesterolemia Obesity Diabetes mellitus Insulin resistance? Cardiac diseases Atrial fibrillation Atrial fibrillation Coronary artery disease Coronary artery disease CHF CHF Behaviours Cigarette smoking Heavy alcohol use Physical inactivity

40
1.Healthy diet; High in fresh fruits, vegetables and low fat dairy products, low in saturated fat and salt in accordance with the DASH diet 2. Regular physical activity: optimum 20-60 minutes of moderate cardiorespiratory activity 3-5/week or more 3. Reduction in alcohol consumption in those who drink excessively (<2 drinks/ day) 4. Weight loss (> 5 Kg) in those who are over weight (BMI>25) 5. Smoke free environment Lifestyle Recommendations
 4. Weight loss (> 5 Kg) in those who are over weight (BMI>25) 5. Smoke free environment Lifestyle Recommendations.")
41
Lifestyle: Weight Loss Healthy BMI: 18.5-24.9 kg/m 2 Waist circumference: <102 cm for men, <88 cm for women ? Insulin Resistance (metabolic syndrome)
.")
42
CAN ALL BARRIERS BE OVERCOME?

43
Treating Hypertension to Prevent Stroke HTN is the single most important modifiable risk factor for stroke HTN is the single most important modifiable risk factor for stroke HTN contributes to 70% of all strokes HTN contributes to 70% of all strokes Atheroma in carotids, aortic arch Atheroma in carotids, aortic arch Friability of small cerebral end arteries Friability of small cerebral end arteries LV dysfunction and atrial fibrillation LV dysfunction and atrial fibrillation

44
Benefits of Treating Hypertension Younger than 60 yrs Younger than 60 yrs Reduces the risk of stroke by 42% Reduces the risk of stroke by 42% Reduces the risk of coronary event by 14% Reduces the risk of coronary event by 14% Older than 60yrs Older than 60yrs Reduces overall mortality by 20% Reduces overall mortality by 20% Reduces cardiovascular mortality by 33% Reduces cardiovascular mortality by 33% Reduces incidence of stroke by 40% Reduces incidence of stroke by 40% Reduces coronary artery disease by 15% Reduces coronary artery disease by 15%

45
Treat Hypertension Aggressively Target most patients still < 140/90 Target most patients still < 140/90 Home Measurement < 135/85 Home Measurement < 135/85 Diabetics < 130/80 Diabetics < 130/80 Lifestyle Modification: Lifestyle Modification: Sodium restriction, DASH diet, physical activity, weight loss, alcohol restriction, smoking cessation Sodium restriction, DASH diet, physical activity, weight loss, alcohol restriction, smoking cessation Expect to use combination therapy Expect to use combination therapy ACE inhibitor, ARB, diuretic ACE inhibitor, ARB, diuretic

46
Percent (%) Hypertension outcome trials Kjeldsen et al. Blood Pressure 2001;10:190-192. 7654321076543210 STOP-1 SHEP STONE SYST-EUR SYST-CHINA HOT CAPP STOP-2 NICS NORDIL INSIGHT Stroke Myocardial infarction

47
Reference: Lancet 2001; 358: 1033-41 PROGRESS TRIAL Randomised placebo-controlled trial designed to determine the effects of a blood pressure-lowering regimen on the risks of stroke and other major vascular events in hypertensive and non hypertensive patients with a history of stroke or TIA Randomised placebo-controlled trial designed to determine the effects of a blood pressure-lowering regimen on the risks of stroke and other major vascular events in hypertensive and non hypertensive patients with a history of stroke or TIA

48
Reference: Lancet 2001; 358: 1033-41 Proportion with event Placebo Active* 01234 Follow-up time (years) 28% risk reduction 95% CI 17 - 38% p<0.0001 *Active: perindopril 4 mg ± indapamide PROGRESS TRIAL STROKE RISK REDUCTION 0.00 0.05 0.10 0.15 0.20
 28% risk reduction 95% CI % p< *Active: perindopril 4 mg ± indapamide PROGRESS TRIAL STROKE RISK REDUCTION")
49
Hypertension: ARB Studies LIFE LIFE (Losartan Intervention for Endpoint Reduction in Hypertension) Randomized controlled trial Randomized controlled trial Treatment: Treatment: Losartan + Atenelol placebo vs Atenelol + Losartan placebo Losartan + Atenelol placebo vs Atenelol + Losartan placebo Hydrochlorothiazide added at 2 months Hydrochlorothiazide added at 2 months At 4 months - Losarten or Atenelol doubled to achieve target BP < 140/90 At 4 months - Losarten or Atenelol doubled to achieve target BP < 140/90 Results Results More patients reached target BP with Losarten vs Atenelol arm More patients reached target BP with Losarten vs Atenelol arm 25% decrease incidence of diabetes 25% decrease incidence of diabetes Less incidence of stroke, MI and death in Losarten arm Less incidence of stroke, MI and death in Losarten arm Lancet 2002;359:995-1003
 Randomized controlled trial Randomized controlled trial Treatment: Treatment: Losartan + Atenelol placebo vs Atenelol + Losartan placebo Losartan + Atenelol placebo vs Atenelol + Losartan placebo Hydrochlorothiazide added at 2 months Hydrochlorothiazide added at 2 months At 4 months - Losarten or Atenelol doubled to achieve target BP < 140/90 At 4 months - Losarten or Atenelol doubled to achieve target BP < 140/90 Results Results More patients reached target BP with Losarten vs Atenelol arm More patients reached target BP with Losarten vs Atenelol arm 25% decrease incidence of diabetes 25% decrease incidence of diabetes Less incidence of stroke, MI and death in Losarten arm Less incidence of stroke, MI and death in Losarten arm Lancet 2002;359:")
50
LIFE: Fatal/Nonfatal Stroke B Dahlof et al. Lancet 2002;359:995-1003 0 6 12 18 24 30364248546066 Study Month

51
Treatment of Hypertension with Cerebrovascular Disease Strongly consider blood pressure reduction Strongly consider blood pressure reduction in all patients after the acute phase of non disabling stroke or TIA in all patients after the acute phase of non disabling stroke or TIA Recommended agents: Recommended agents: ACE-I, diuretics ARB - ongoing studies ß-blockers, CCB

52
Hypercholesterolemia: Using Statins for Secondary Prevention of Stroke Lipid-lowering trials using statins have shown benefit in decreasing progression and/or inducing regression of carotid artery plaque Lipid-lowering trials using statins have shown benefit in decreasing progression and/or inducing regression of carotid artery plaque Lipid-lowering trials using statins for secondary prevention (of CHD) have shown benefit in stroke prevention Lipid-lowering trials using statins for secondary prevention (of CHD) have shown benefit in stroke prevention
 have shown benefit in stroke prevention Lipid-lowering trials using statins for secondary prevention (of CHD) have shown benefit in stroke prevention")
53
Why Should Statins Prevent Ischemic Stroke? Lipid effects = LDL lowering Lipid effects = LDL lowering Target LDL-C < 2.0 mmol/L (in stroke patients) Target LDL-C < 2.0 mmol/L (in stroke patients) Non-lipid effects = Non-lipid effects = Stabilizing plaques Stabilizing plaques Improving endothelial function Improving endothelial function Decreasing inflammation Decreasing inflammation Decreasing platelet aggregation Decreasing platelet aggregation Directly lowering blood pressure Directly lowering blood pressure Decreasing cardiac emboli Decreasing cardiac emboli
 Target LDL-C < 2.0 mmol/L (in stroke patients) Non-lipid effects = Non-lipid effects = Stabilizing plaques Stabilizing plaques Improving endothelial function Improving endothelial function Decreasing inflammation Decreasing inflammation Decreasing platelet aggregation Decreasing platelet aggregation Directly lowering blood pressure Directly lowering blood pressure Decreasing cardiac emboli Decreasing cardiac emboli.")
54
Statin Studies SPARCL SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) Double Blind Randomized Controlled Trial Double Blind Randomized Controlled Trial Stroke or TIA within 1-6 months Stroke or TIA within 1-6 months Treatment: Treatment: Atorvastatin 80 mg once daily or placebo Atorvastatin 80 mg once daily or placebo Results Results 5 year absolute reduction in risk of stroke - 22% 5 year absolute reduction in risk of stroke - 22% 5 year absolute reduction in risk of major CV events - 3.5% 5 year absolute reduction in risk of major CV events - 3.5% Significant increase in hemorrhagic stroke Significant increase in hemorrhagic stroke N Engl J Med 2006;355:549-559
 Double Blind Randomized Controlled Trial Double Blind Randomized Controlled Trial Stroke or TIA within 1-6 months Stroke or TIA within 1-6 months Treatment: Treatment: Atorvastatin 80 mg once daily or placebo Atorvastatin 80 mg once daily or placebo Results Results 5 year absolute reduction in risk of stroke - 22% 5 year absolute reduction in risk of stroke - 22% 5 year absolute reduction in risk of major CV events - 3.5% 5 year absolute reduction in risk of major CV events - 3.5% Significant increase in hemorrhagic stroke Significant increase in hemorrhagic stroke N Engl J Med 2006;355:")
55
Hypercholesterolemia: Using Statins for Secondary Prevention of Stroke Should statins be used if lipids normal? Should statins be used if lipids normal? consider statin if event presumed to be of atherosclerotic origin even if no preexisting indications Stroke 2006;37:577-617

56
Cholesterol Lowering----- Statins as first line therapy Statins as first line therapy Ezetimibe: Ezetimibe: a) First line for patients intolerant to a) First line for patients intolerant to statins statins b) Dual inhibition b) Dual inhibition
 First line for patients intolerant to a) First line for patients intolerant to statins statins b) Dual inhibition b) Dual inhibition")
57
Secondary Stroke Prevention Evaluate the Event : Identify Events requiring Urgent intervention / Identify cause Identify Events requiring Urgent intervention / Identify cause TIA / Minor Stroke Risk Assessment TIA / Minor Stroke Risk Assessment Investigations Investigations CT, MRI, ECG, Carotid imaging, echocardiogram CT, MRI, ECG, Carotid imaging, echocardiogram Implement Interventions Carotid Endarterectomy Carotid Endarterectomy Initiate Medications Antiplatelets /anticoagulants, ACE-I, Diuretics, ARB, statins Antiplatelets /anticoagulants, ACE-I, Diuretics, ARB, statins Modify Stroke Risk Factors Vascular Risk Factors Vascular Risk Factors Behavioral/Lifestyle Risk Factors Behavioral/Lifestyle Risk Factors

58
Impact of Prevention Strategies Do they work ?

59
*Based on estimated 700,000 annual strokes. Gorelick PB. Arch Neurol. 1995;52:347-355. Gorelick PB. Stroke. 2002;33:862-875. 0100,000200,000300,000400,000 360,500 146,000 89,500 68,500 34,500 Number of Preventable Strokes* Hypertension Cholesterol Cigarettes Atrial Fibrillation Heavy Alcohol Use How Many Strokes Annually Can Be Prevented by Risk-Factor Control? 25,000 10,000 5000 6400 2500

60
Cumulative Relative risk reduction Survivors of first stroke and a TIA Survivors of first stroke and a TIA Diet, Exercise, Aspirin, Statins and Anti- hypertensives Diet, Exercise, Aspirin, Statins and Anti- hypertensives RR of 80% RR of 80% NNT 5 to prevent 1 event in 5 years NNT 5 to prevent 1 event in 5 years Stroke. June, 2007

61
BRAIN ATTACK STROKE CAN BE PREVENTED!

Similar presentations


















>")
