Download presentation
Presentation is loading. Please wait.

1
Peritonitis Priorities Paul Finan Department of Colorectal Surgery Leeds General Infirmary

3
Peritonitis Classification Primary - often spontaneous and single organism Secondary - multiple organisms, perforations, leaks, ischaemia etc Tertiary - no organisms, disturbance in host immune response

4
Priorities in Peritonitis Early Recognition Often classical clinical picture but…. Beware of immuno-suppressed patients Elderly patients Post-operative patients with cardiac problems Unexplained failure to progress clinically

5
Peritonitis Priorities Radiological Support Plain films e.g. free gas or unexplained ileus Abdominal ultrasound – simple collections CT scanning – of particular value in the post-operative patient Labelled white cell scans MR imaging – no experience

6
Peritonitis on CT Scanning

7
Peritonitis Priorities Radiologist Microbiologist Anaesthetist Nursing Staff Surgical Staff Wound Care Specialists Nutritional Team

8
Scoring Systems

9
An effort to quantify case mix and so estimate outcome APACHE – initially 34 variables APACHE II – reduced to 12 variables Sepsis Score (SS) Sepsis Severity Score (SSS)
 Sepsis Severity Score (SSS)")
10
Relationship Between APACHE-II and Mortality

11
Prognostic Scoring Systems in Peritonitis Comparison of APACHE II, APS, SSS, MOF and MPI, in 50 patients with peritonitis All scoring systems predicted outcome in univariate analysis APACHE II and MPI contributed independently in a multivariate analysis All patients with an APACHE II of >20 or MPI >27 died in hospital Bosscha et al 1997

12
Peritonitis Priorities Source Control Damage Limitation

13
Source Control Drainage of abscesses Debridement of devitalised tissue Diversion, repair or excision of focus of infection from a hollow viscus

14
Source Control Drainage of abscesses Surgical or non-surgical drainage governed by.. Clinical state of patient Site of collection Extent of collection Underlying aetiology

15
Diverticular Abscess

16
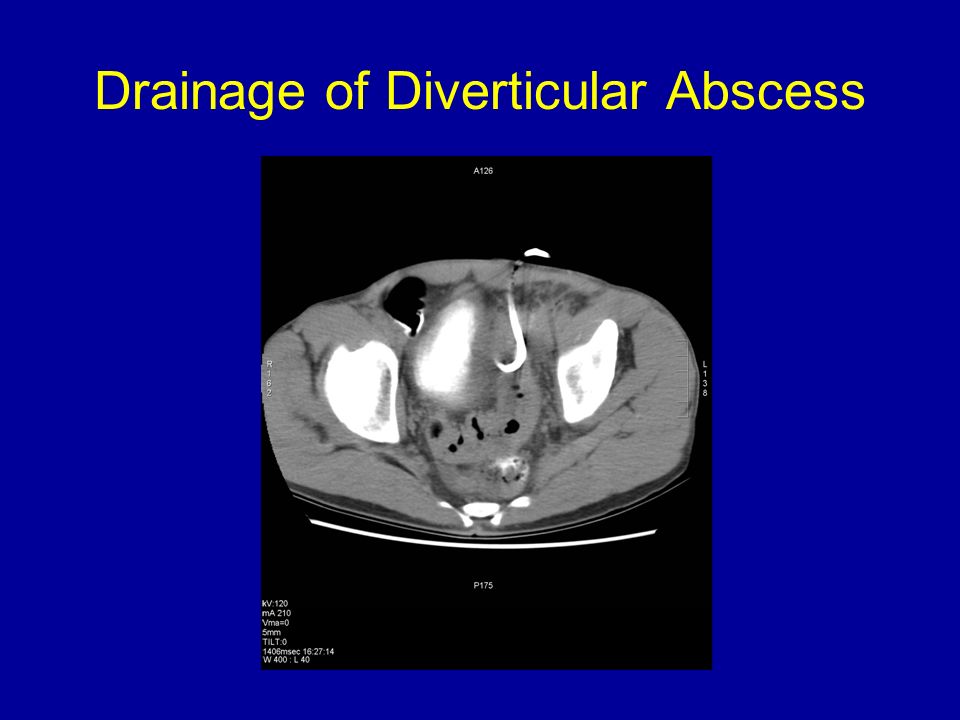
Drainage of Diverticular Abscess

18
Non-surgical Drainage of Intra-abdominal Abscesses A study of PCD in 96 patients with 137 abscesses accumulated over a 3-year period Successful resolution in 70% after a single procedure and 82% with a second drainage More often successful in post-operative abscesses. Poorer results with pancreatic abscesses and those containing yeasts Cinat et al 2002

19
Non-surgical drainage of Intra-abdominal Abscesses A study of 75 patients undergoing PCD of intra- abdominal abscess Successful treatment in 62/75 patients (83%) Success associated with unilocular collections, <200 mls., APACHE score <30 and accessible regions Betsch et al 2002
 Success associated with unilocular collections, <200 mls., APACHE score <30 and accessible regions Betsch et al 2002")
20
Pancreatic Collection

21
Pancreatic Drainage

22
Source Control Debridement of Devascularised Tissue Most commonly encountered in necrotic pancreatitis Removal of dead bowel Debridement of other necrotic intra- abdominal tissue

23
Source Control Management of the Source of Contamination Excision – appendicitis, cholecystitis Repair – perforated ulcer, early iatrogenic injury Diversion +/- excision – leaking anastamosis NB These are the decisions that require experience

24
Damage Limitation Procedures at the time of surgery Decisions in the post-operative period

26
Peritoneal Lavage

27
Damage Limitation Decisions at the time of Surgery Management of the infective source Peritoneal toilet and removal of particulate matter Peritoneal lavage Drains Wound closure

28
VAC Dressing

29
Damage Limitation Post-operative Decisions Re-laparotomy Laparostomy Interval imaging Duration of antibiotic therapy

30
Re-laparotomy in Peritonitis Failure to progress clinically Prompted by radiological imaging Where viability is in doubt Failure to control source of infection

31
Relaparotomy for Secondary Peritonitis Meta-analysis comparing planned relaparotomy and laparotomy on demand No randomised studies Non-significant reduction in mortality with the latter approach Evidence based on eight heterogeneous studies Lamme et al 2002

32
Laparostomy Abdominal wall cannot or should not be closed Major loss of the abdominal wall Visceral or retroperitoneal oedema If decision has already been taken to perform a re-laparotomy Likelihood of creating abdominal compartment syndrome

33
Peritonitis Priorities Radiologist Microbiologist Anaesthetist Nursing Staff Surgical Staff Wound Care Specialists Nutritional Team

34
Antibiotics in Peritonitis Consideration to source of infection and likely bacteria Fewer drugs for shorter periods of time A policy of reculture and change if necessary No clear benefit of a particular regimen in the Cochrane review (Wong et al 2005)
")
35
Peritonitis Priorities Conclusions Multi-disciplinary approach Increasing role of the radiologist Emphasis on source control Need for correct decision at time of laparotomy Lack of trial evidence

Similar presentations