Download presentation
Presentation is loading. Please wait.

1
Is There Still a Controversy About Stent Type for TASC C&D Lesions
Is There Still a Controversy About Stent Type for TASC C&D Lesions? Insights From COBEST Randomized Trial Aravinda Nanjundappa, MD, FACC, FSCAI Associate Professor of Medicine and Surgery West Virginia University Charleston, WV

2
Claudication treatment options
Treatment Benefit QOL Limitation Exercise % ↑↑ Not available Angioplasty % ↑ Distal lesions Surgery % ↑↑ 2-5% risk Cilostazol % ↑ Not in CHF

3
Claudication treatment options
Treatment Mechanism TASC II Exercise Metabolic, Walking efficiency A Endothelial Angioplasty Hemodynamic A Cilostazol Metabolic, Hemodynamic A Vascular smooth muscle

4
Results of Iliac Angioplasty
Gruntzig (1979) Spence (1981) Schwarten (1984) Kumpe (1982) Gallino (1982) Two to Four Year Patency 100 95 89% 90 87% 87% % 85 82% 82% 80 2 Year 2 Year 4 Year 2 Year 3 Year 75 70
 Spence (1981) Schwarten (1984) Kumpe (1982) Gallino (1982) Two to Four Year Patency % % 87% % % 82% Year. 2 Year. 4 Year. 2 Year. 3 Year")
5
Results of Iliac Angioplasty
Late Clinical Success % 75.2 667 iliac procedures analyzed One month clinical success 90.2% 80 64.9 70 59.7 56.7 53.4 60 50 40 1 Year 2 Years 3 Years 4 Years 30 5 Years 20 10 Ann Surg 1987;206:403-13

6
Stenting of Iliac Arteries Multicenter Experience
Stage 0 Effect on Clinical Stage Stage I Stage II Stage III 80 Stage IV 70 60 50 % 40 30 20 10 Before Treatment After Treatment Cardiovasc Intervent Radiol 1992;15:291-7.

7
Stenting of Iliac Arteries Multicenter Experience
587 procedures in 486 patients. 1.9 ± 1.3 stents per patient (1 - 8). 405 patients - unilateral stents. 81 patients - bilateral stents. Mean follow-up: 13.3 ± 11 months (1 - 48). 201 patients underwent angiographic follow-up at 8.7 ± 5.7 months. Cardiovasc Intervent Radiol 1992;15:291-7.
. 405 patients - unilateral stents. 81 patients - bilateral stents. Mean follow-up: 13.3 ± 11 months (1 - 48). 201 patients underwent angiographic follow-up at 8.7 ± 5.7 months. Cardiovasc Intervent Radiol 1992;15:")
8
Stenting of Iliac Arteries Multicenter Experience
Angiographic patency (defined as < 50% stenosis within stent): 92% Sustained clinical benefit: 90.9% at 1 year 84.1% at 2 years 68.6% at 43 months Diabetes and poor run off had a negative influence on the clinical outcome
: 92% Sustained clinical benefit: 90.9% at 1 year. 84.1% at 2 years. 68.6% at 43 months. Diabetes and poor run off had a negative influence on the clinical outcome.")
9
Four Year Patency Critical Limb Ischemia Radiology 1997;204:87-96

10
Four Year Patency Claudication Radiology 1997;204:87-96

11
PTA vs. Stenting For Aortoiliac Occlusive Disease
Meta-analysis of 6 PTA studies (1,300 patients) and 8 stent studies (816 patients) Immediate technical success: PTA 91% Stent 96% Risk of long-term failure reduced by 39% after stenting P < 0.05 Radiology 1997;204:87-96
 and 8 stent studies (816 patients) Immediate technical success: PTA 91% Stent 96% Risk of long-term failure reduced by 39% after stenting. P < Radiology 1997;204:")
12
Randomized Trial: Mean Restenosis
% Luminal Narrowing G. Richter et al, 1992

13
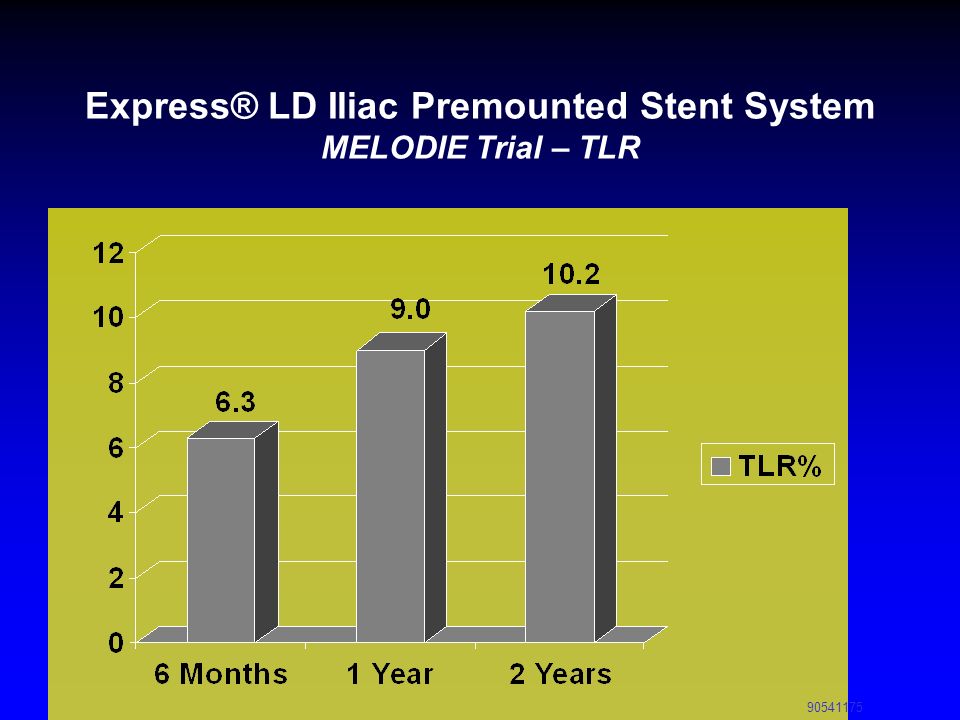
Express® LD Iliac Premounted Stent System, MELODIE Trial - Overview
Trial Design: A prospective, multi-center, single arm study to obtain additional data on the safety and efficacy of the Express™ LD Stent implantation in the treatment of stenosed or occlusive atherosclerotic disease (de novo or restenotic) in iliac arteries (common and/or external). Objective: The objective was to demonstrate non-inferiority of the Express™ LD Stent for the treatment of atherosclerotic iliac artery lesions as compared to an objective performance criterion* (OPC), with a primary endpoint of mean percent luminal diameter loss at 6 months. Enrollment: 151 patients (163 lesions) with de novo or restenotic atherosclerotic lesions <100mm long in vessels between 5 and 10 mm in diameter with stenosis > 50%. *Objective Performance Criterion An objective performance criterion (OPC) is a benchmark used to compare a trial’s results against a literature derived control group. For the MELODIE study the objective performance criterion was constructed from the Palmaz® Balloon Expandable Stent iliac study, Cardiovasc Intervent Radiol 15: , 1992, and was defined as 15% mean percent luminal diameter loss at 6 months. Palmaz is a trademark of Johnson and Johnson.
 in iliac arteries (common and/or external). Objective: The objective was to demonstrate non-inferiority of the Express™ LD Stent for the treatment of atherosclerotic iliac artery lesions as compared to an objective performance criterion* (OPC), with a primary endpoint of mean percent luminal diameter loss at 6 months. Enrollment: 151 patients (163 lesions) with de novo or restenotic atherosclerotic lesions <100mm long in vessels between 5 and 10 mm in diameter with stenosis > 50%. *Objective Performance Criterion An objective performance criterion (OPC) is a benchmark used to compare a trial’s results against a literature derived control group. For the MELODIE study the objective performance criterion was constructed from the Palmaz® Balloon Expandable Stent iliac study, Cardiovasc Intervent Radiol 15: , 1992, and was defined as 15% mean percent luminal diameter loss at 6 months. Palmaz is a trademark of Johnson and Johnson")
14
Express® LD Iliac Premounted Stent System MELODIE Trial – TLR
15
Role of covered stents Several studies have demonstrated that PTFE covered stents may provide better results as compared to bare metal stents, particularly in TASC C and D lesions. Chang, et al demonstrated that covered stents show a significantly higher patency rate long term (at 5 years) as compared to bare metal stents when used to treat TASC C & D iliac lesions (87% vs. 53% p≤.01)6.
 as compared to bare metal stents when used to treat TASC C & D iliac lesions (87% vs. 53% p≤.01)6.")
16
Covered stents Of note, the covered stent lesion characteristics were statistically more advanced than those in the bare metal group (38% of covered stent group had type C & D lesions versus 7% for BMS p=0.034). The covered stent group had superior outcomes, regardless of the type of lesions treated
. The covered stent group had superior outcomes, regardless of the type of lesions treated.")
17
TASC II aorto-iliac lesions Type C and Type D

18
Atrium’s Bx Covered Stents Advanta™ V12 and iCAST™
iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only)
")
19
Atrium’s FilmCast™ Encapsulation Technology
Stent type Length Uncoated corrugated ring (28 day) 72±23 ePTFE+corrugated ring (28 day) 18±03* Uncoated slotted tube (28 day) 93±16 ePTFE+slotted tube (28 day) 17±04*** Neointimal (µm) ePTFE+slotted tube (56 day) 13±02 * P<0.007 compared to uncoated corrugated ring **P< compared to uncoated slotted tube BMS at 28 days Covered Stent at 28 days Rogers, C & E. Edelman. A Non-GLP Study of Biologic Responses to Uncoated and PTFE Coated Steel Stents in Rabbit Iliac Arteries. (1997) iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
 72±23. ePTFE+corrugated ring (28 day) 18±03* Uncoated slotted tube (28 day) 93±16. ePTFE+slotted tube (28 day) 17±04*** Neointimal (µm) ePTFE+slotted tube (56 day) 13±02. * P<0.007 compared to uncoated corrugated ring. **P< compared to uncoated slotted tube. BMS. at 28 days. Covered Stent. at 28 days. Rogers, C & E. Edelman. A Non-GLP Study of Biologic Responses to Uncoated and PTFE Coated Steel Stents in Rabbit Iliac Arteries. (1997) iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
20
iCAST is FDA approved for the treatment of tracheobronchial strictures.
Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
.")
22
COBEST Trial What is COBEST: (Covered Balloon Expandable Stent Trial)
A prospective, randomized, controlled, multi-center (12 sites) clinical trial comparing Atrium’s balloon expandable covered stent to bare metal stents for use in iliac occlusive disease. Inclusion criteria: Type B, C, or D lesions. Dissection after angioplasty. Recurrent stenosis after angioplasty. Follow up: Patients were followed clinically (with ABI and symptom relief) and by duplex US scan at 6, 12, and 18 months. Primary Objective: Binary restenosis (<50% stenosis on DU/Angiogram)=primary patency at 6, 12 and 18 months. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
 clinical trial comparing Atrium’s balloon expandable covered stent to bare metal stents for use in iliac occlusive disease. Inclusion criteria: Type B, C, or D lesions. Dissection after angioplasty. Recurrent stenosis after angioplasty. Follow up: Patients were followed clinically (with ABI and symptom relief) and by duplex US scan at 6, 12, and 18 months. Primary Objective: Binary restenosis (<50% stenosis on DU/Angiogram)=primary. patency at 6, 12 and 18 months. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
23
COBEST Trial-18 Month Results
Atrium’s covered stent technology is superior to bare metal stents for iliac occlusive disease. • V12 showed lower binary restenosis rates (p=0.037). Binary restenosis defined as vessel patency <50% This proves the V12 offers higher patency than bare metal stents The Kaplan Meier curve shows that the V12 group had less binary restenosis compared to the bare metal stent group and was considered statistically significant. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
. Binary restenosis defined as vessel patency <50% This proves the V12 offers higher patency than bare metal stents. The Kaplan Meier curve shows that the V12 group had less binary restenosis compared to the bare metal stent group and was considered statistically significant. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
24
COBEST Trial-18 Month Results
V12 group experienced the greatest improvement in Type C & D lesions These findings are highly statistically significant (p<.002) V12 outperforms bare metal stents with more challenging C & D lesions iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
 V12 outperforms bare metal stents with more challenging C & D lesions. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
25
COBEST Trial-18 Month Results
V12 showed significantly lower target lesion revascularization Rates (TLR) If the patient received a bare metal stent, they were 5X more likely to need a re-intervention This is a huge burden on a patients quality of life and an enormous economic impact on the overall health system iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
 If the patient received a bare metal stent, they were 5X more likely to need a re-intervention. This is a huge burden on a patients quality of life and an enormous economic impact on the overall health system. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
26
Outcomes of Kissing Covered Stents Compared to Non-Covered Stents for Aortic Bifurcation Lesions
Objective: Retrospective review Kissing Stents for aorto-iliac lesions Compared bare metal stents to covered stents Methods: 26 patients received Atrium covered stents 28 patients received bare metal stents 17 patients with Palmaz Genesis (Cordis) and 11 patients with Express LD (BS) Median follow up was 21 months 25 months for the non covered stent group 20 months for the covered stent group Indications for stent placement included claudication and limb-threatening ischemia. iCAST is FDA approved for the Sabri SS, Angle JF, Choudrhi AF, Dake MD Journal of Vascular and Interventional Radiology July 2010 treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
 and 11 patients with Express LD (BS) Median follow up was 21 months. 25 months for the non covered stent group. 20 months for the covered stent group. Indications for stent placement included claudication and limb-threatening ischemia. iCAST is FDA approved for the Sabri SS, Angle JF, Choudrhi AF, Dake MD Journal of Vascular and Interventional Radiology July 2010 treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
27
38% of Atrium covered stent patients had type C & D lesions (p=0.034)
Outcomes of Kissing Covered Stents Compared to Non-Covered Stents for Aortic Bifurcation Lesions Results: Treated lesion characteristics were statistically more advanced in the patients with covered stents: 38% of Atrium covered stent patients had type C & D lesions (p=0.034) 7% of BMS patients had type C lesions 0% of BMS patients had type D lesions 92% of BMS patients had simple type A & B lesions Technical success was achieved in 100% in both groups. Primary patency rates at 1 & 2 years: Bare Metal Stents = 78% and 62% iCAST covered stents = 92% and 92% (p value = 0.023) ABI’s at follow up: Covered stent group- increased from 0.74/0.61 (right/left) to 0.80/0.88 Bare metal stent group-decreased from 0.77/0.070 (right/left) to 0.74/0.79 iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
 7% of BMS patients had type C lesions. 0% of BMS patients had type D lesions. 92% of BMS patients had simple type A & B lesions. Technical success was achieved in 100% in both groups. Primary patency rates at 1 & 2 years: Bare Metal Stents = 78% and 62% iCAST covered stents = 92% and 92% (p value = 0.023) ABI’s at follow up: Covered stent group- increased from 0.74/0.61 (right/left) to 0.80/0.88. Bare metal stent group-decreased from 0.77/0.070 (right/left) to 0.74/0.79. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).")
28
Outcomes of Kissing Covered Stents Compared to Non-Covered Stents for Aortic Bifurcation Lesions
Results Continued: Sustained clinical improvement at follow up: 85% of Atrium covered stent patients had sustained clinical symptom improvement during follow up period. 54% of BMS patients had sustained clinical symptom improvement TVR at 2 years: Atrium Covered Stent = 8% BMS = 38 % Conclusion: There is a clinically and statistically significant difference in the patency rates of balloon expandable covered versus bare metal balloon expandable stents employed in the treatment of atherosclerotic occlusive disease of the aortic bifurcation and proximal CIA’s. iCAST is FDA approved for the treatment of tracheobronchial strictures. Advanta V12 is CE approved for restoring the patency of iliac and renal arteries (renal approval is for 5-7mm sizes only).
.")
29
iCARUS Trial What is iCARUS? Atrium iCAST Iliac Stent Trial
IDE trial to support a PMA application Objective: To evaluate the iCAST covered stent for treating iliac artery stenosis (as compared to other FDA approved iliac stents) in patients with de novo or restenotic lesions in the common and/or external iliac arteries.
 in patients with de novo or restenotic lesions in the common and/or external iliac arteries.")
30
iCARUS Trial Study design:
Prospective, multi-center, non-randomized, single arm registry Primary endpoint: A composite endpoint defined as: Occurrence of death with 30 days, Target site revascularization or Restenois within 9 months post-procedure

31
iCARUS Trial Secondary Endpoints: MAVE MAE Device Success
Acute Procedural Success Clinical Success Patency Composite rate of 30 day death, 9-month target site revascularization and 9 month restenosis in subjects without total occlusions of the iliac

32
iCARUS Trial Clinical sites: 25 sites in the US 1 international site
165 Patients enrolled Enrollment: Completed in October 2010 9 month follow up Last patient scheduled for 9 month follow up in July 2011 PMA submission by end of 2011

33
Conclusions Covered stents are safe, less TVR and less re stenosis for patients with TASC C and D lesions Results of iCARUS are awaited Cost benefit ratio of covered stent versus BMS: Less TVR and less readmissions

Similar presentations



 Speaker Slideset GORE ®, VIABAHN ®, and designs are trademarks of W. L. Gore & Associates.>")
 study with the Sirolimus coated BX™ VElocity balloon expandable stent (CYPHER™)>")


 Final Results Hans Krankenberg (on behalf of the FAST Investigators) Hamburg University Cardiovascular Center Prof.>")
 and of restenoses after stent deployment (ISR) still show.>")


 +/- stenting in a subgroup of patients.>")







