Download presentation
Presentation is loading. Please wait.

1
Future Therapies of HCV Miranda Surjadi, NP San Francisco General Hospital Department of Gastroenterology/Hepatology

2
Virology of Hepatitis C HCV is a small, enveloped single stranded RNA virus in the Flaviviridae family HCV is a small, enveloped single stranded RNA virus in the Flaviviridae family There are six major genotypes There are six major genotypes and more than 100 subtypes and more than 100 subtypes

4
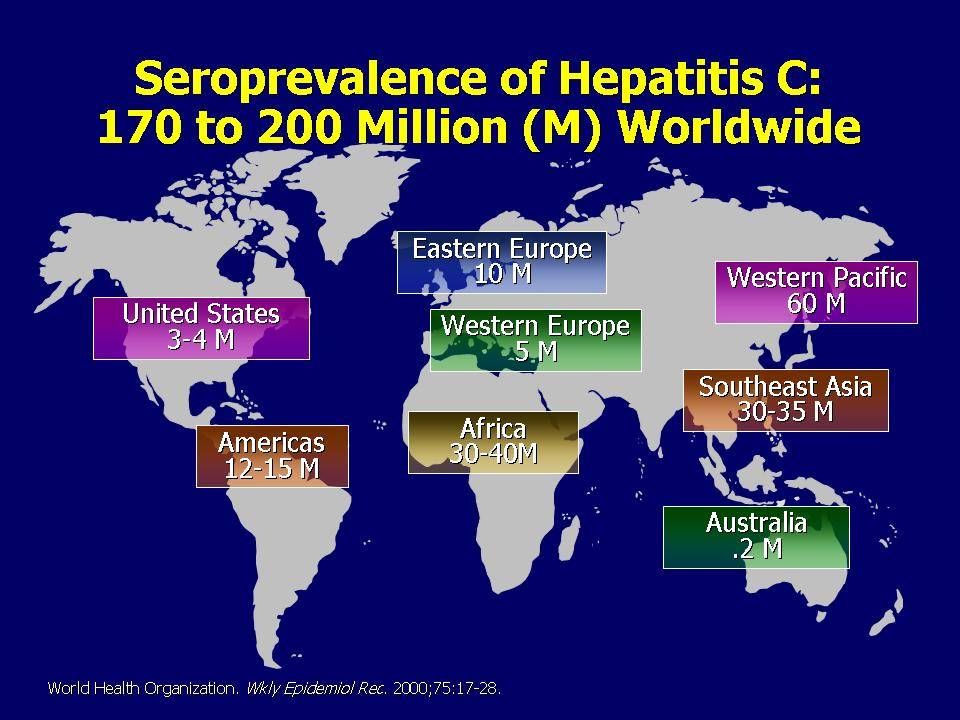
Hepatitis C Blood bank screening for HCV in 1987 Blood bank screening for HCV in 1987 4 million in the US with chronic HCV 4 million in the US with chronic HCV Leading cause of cirrhosis in the US Leading cause of cirrhosis in the US Most common reason for liver transplantation Most common reason for liver transplantation 8000-10,000 deaths/ year 8000-10,000 deaths/ year

5
Natural history of HCV ACUTE HCV INFECTION 15-25% clear HCV 75-85% chronic HCV 20% cirrhosis in 20 yrs 1-5% risk of HCC per year

6
Factors that increase the evolution to cirrhosis Infection at an older age (>40yo) Infection at an older age (>40yo) Male sex Male sex Drinking more than 50grams of alcohol per day (5 drinks) Drinking more than 50grams of alcohol per day (5 drinks) Obese or with hepatic steatosis on biopsy Obese or with hepatic steatosis on biopsy HIV/HBV co-infection HIV/HBV co-infection
 Infection at an older age (>40yo) Male sex Male sex Drinking more than 50grams of alcohol per day (5 drinks) Drinking more than 50grams of alcohol per day (5 drinks) Obese or with hepatic steatosis on biopsy Obese or with hepatic steatosis on biopsy HIV/HBV co-infection HIV/HBV co-infection")
7
Positive HCV Ab HCV RNA positive Evaluate: LFTs, ANA, HBV, HIV, Iron studies, lipids, HCV genotype, imaging Refer to Liver Clinic for treatment HCV RNA negative Recheck in 6 months to verify If HCV RNA negative x 2, then no need for further f/u.

8
History of HCV therapy Interferon was approved for use in HCV in 1992. It was shown to decrease HCV RNA levels and lead to SVR in some patients. Interferon was approved for use in HCV in 1992. It was shown to decrease HCV RNA levels and lead to SVR in some patients. Ribavirin is a nucleoside analog known to have activity against several flaviviruses. Ribavirin does not have much effect on HCV RNA levels alone. However, in combination with interferon, SVR rates were increased. Ribavirin is a nucleoside analog known to have activity against several flaviviruses. Ribavirin does not have much effect on HCV RNA levels alone. However, in combination with interferon, SVR rates were increased. Ribavirin was approved for use as an adjunct to interferon in 1998. Ribavirin was approved for use as an adjunct to interferon in 1998. Pegylated interferon allowed for once weekly injections instead of 3x/week and also yielded higher rates of SVR. This was approved for use in 2001. Pegylated interferon allowed for once weekly injections instead of 3x/week and also yielded higher rates of SVR. This was approved for use in 2001.

9
Goal of HCV therapy Goal of HCV therapy is SVR (sustained viral response). Goal of HCV therapy is SVR (sustained viral response). SVR is defined as an undetectable HCV RNA 24 weeks after finishing HCV therapy SVR is defined as an undetectable HCV RNA 24 weeks after finishing HCV therapy SVR and duration of treatment is determined by HCV genotype SVR and duration of treatment is determined by HCV genotype
. SVR is defined as an undetectable HCV RNA 24 weeks after finishing HCV therapy SVR is defined as an undetectable HCV RNA 24 weeks after finishing HCV therapy SVR and duration of treatment is determined by HCV genotype SVR and duration of treatment is determined by HCV genotype.")
10
Current therapy of HCV Genotype 1: Genotype 1: Duration of treatment: 48 weeks Duration of treatment: 48 weeks SVR: 42-50% SVR: 42-50% 70% of US population 70% of US population Genotypes 2 and 3: Genotypes 2 and 3: Duration of treatment: 24 weeks Duration of treatment: 24 weeks SVR: 80% SVR: 80% 25% of US population 25% of US population

11
IL 28B: strong predictor of SVR IDEAL study: PegIntron vs. Pegasys in genotype 1 IDEAL study: PegIntron vs. Pegasys in genotype 1 Analysis of on treatment response by IL 28B polymorphism found it to be strong predictor of SVR. Analysis of on treatment response by IL 28B polymorphism found it to be strong predictor of SVR. This pattern of SVR is similar across Caucasians, Latinos, and African Americans This pattern of SVR is similar across Caucasians, Latinos, and African Americans CC allele : 69% SVR CC allele : 69% SVR CT allele: 33% SVR CT allele: 33% SVR TT allele: 27% SVR TT allele: 27% SVR

12
SVR rates of past and current HCV therapies 21 37 46 45 61 76

13
Side effects to pegylated interferon More common : Flu-like symptoms Flu-like symptoms Fatigue, muscle aches, joint aches, fever, headaches Fatigue, muscle aches, joint aches, fever, headaches Injection site reaction Injection site reaction Psychiatric symptoms: depression, anxiety, mood lability Psychiatric symptoms: depression, anxiety, mood lability Lab alterations: neutropenia, anemia, thrombocytopenia Lab alterations: neutropenia, anemia, thrombocytopenia Anorexia, nausea Anorexia, nausea Alopecia Alopecia Less common : Autoimmune disorders, like thyroid disorders Numbness/tingling in feet Eye disorders, especially in diabetics (very rare)
")
14
Side effects to ribavirin Hemolytic anemia Hemolytic anemia Teratogenicity, category X Teratogenicity, category X Pruritus, rash Pruritus, rash Insomnia Insomnia

15
Contraindications to HCV treatment * Major, uncontrolled depression/anxiety Major, uncontrolled depression/anxiety Current alcohol or drug use Current alcohol or drug use Autoimmune hepatitis or autoimmune conditions known to be exacerbated by pegIFN and RBV (IBD, SLE, RA, etc.) Autoimmune hepatitis or autoimmune conditions known to be exacerbated by pegIFN and RBV (IBD, SLE, RA, etc.) Recent neoplasm (BCC and SCC ok) Recent neoplasm (BCC and SCC ok) Untreated hyperthyroidism Untreated hyperthyroidism Pregnant or unwilling to comply with double contraception Pregnant or unwilling to comply with double contraception Severe, poorly controlled concurrent medical conditions: CHF, COPD, DM, CAD Severe, poorly controlled concurrent medical conditions: CHF, COPD, DM, CAD *For SFGH Liver Clinic only
 Autoimmune hepatitis or autoimmune conditions known to be exacerbated by pegIFN and RBV (IBD, SLE, RA, etc.) Recent neoplasm (BCC and SCC ok) Recent neoplasm (BCC and SCC ok) Untreated hyperthyroidism Untreated hyperthyroidism Pregnant or unwilling to comply with double contraception Pregnant or unwilling to comply with double contraception Severe, poorly controlled concurrent medical conditions: CHF, COPD, DM, CAD Severe, poorly controlled concurrent medical conditions: CHF, COPD, DM, CAD *For SFGH Liver Clinic only")
16
Monitoring HCV RNA during treatment Rapid viral response: undetectable HCV RNA at wk 4 Rapid viral response: undetectable HCV RNA at wk 4 Early virological response: undetectable HCV RNA at wk 12 Early virological response: undetectable HCV RNA at wk 12 Complete responder: HCV RNA undetectable at the end of therapy Complete responder: HCV RNA undetectable at the end of therapy Patient needs at least a 2-log drop in HCV RNA at wk 12 and an undetectable HCV RNA at wk 24 to continue with treatment. Patient needs at least a 2-log drop in HCV RNA at wk 12 and an undetectable HCV RNA at wk 24 to continue with treatment.

17
Monitoring HCV RNA during treatment Start HCV treatment 2-log drop in HCV RNA in 12 weeks HCV RNA undetectable in 24 weeks HCV RNA undetectable at end of treatment (week 48) SVR= undetectable HCV RNA 6 months s/p treatment Relapser if HCV RNA present Non responder if HCV RNA present at week 24
 SVR= undetectable HCV RNA 6 months s/p treatment Relapser if HCV RNA present Non responder if HCV RNA present at week 24")
18
Future therapies of HCV HCV RNA genome encodes for a single polyprotein. The polyprotein is cleaved during and after translation into mature viral proteins by host and viral encoded proteases. The NS3/4A viral protein contains a serine protease activity that is required for cleavage of the viral polyprotein. NS3/4A Protease inhibitors Phase 3: Telaprevir and Boceprevir Phase 3: Telaprevir and Boceprevir

19
Telaprevir Phase 1 studies show marked reduction in HCV RNA by a mean of 4.4 log IU/ml Phase 1 studies show marked reduction in HCV RNA by a mean of 4.4 log IU/ml Phase 1 studies also show a rapid emergence of viral resistant mutants with telaprevir monotherapy Phase 1 studies also show a rapid emergence of viral resistant mutants with telaprevir monotherapy These resistant mutants are still sensitive to pegylated interferon These resistant mutants are still sensitive to pegylated interferon Subsequent trials combine pegylated interferon, ribavirin, and telaprevir Subsequent trials combine pegylated interferon, ribavirin, and telaprevir

20
Telaprevir: PROVE 1 and 2 TPV/pIFN/RBV 12 wks + pIFN/RBV 36 wks= 69%SVR TPV/pIFN/RBV 12 wks + pIFN/RBV 36 wks= 69%SVR TPV/pIFN/RBV 12 wks + pIFN/RBV 12wks = 60%SVR TPV/pIFN/RBV 12 wks + pIFN/RBV 12wks = 60%SVR Control group: pegIFN/RBVx48wks= 46% SVR Control group: pegIFN/RBVx48wks= 46% SVR 12% of patients had to stop treatment due to TPV related rash 12% of patients had to stop treatment due to TPV related rash All patients in PROVE 1 and 2 are treatment naïve

21
Boceprevir: SPRINT 1 and 2 pIFN/RBV 4wks + BOC/pIFN/RBV x 28 or 48wks = 56%/75% SVR pIFN/RBV 4wks + BOC/pIFN/RBV x 28 or 48wks = 56%/75% SVR BOC/pIFN/RBV x 28 or 48wks = 54%/67% SVR BOC/pIFN/RBV x 28 or 48wks = 54%/67% SVR Control group: pIFN/RBV x 48wks = 38% SVR Control group: pIFN/RBV x 48wks = 38% SVR 10-26% of patients had to stop due to anemia from BOC 10-26% of patients had to stop due to anemia from BOC All patients in SPRINT 1 and 2 were HCV treatment naïve

22
Boceprevir Anemia was more common in the boceprevir arm Anemia was more common in the boceprevir arm 10-26% of patients in the boceprevir group had treatment discontinuations secondary to anemia compared to 9% in the control group 10-26% of patients in the boceprevir group had treatment discontinuations secondary to anemia compared to 9% in the control group The addition of Epogen reduced the discontinuation rate to 2-8% in the boceprevir arms. The addition of Epogen reduced the discontinuation rate to 2-8% in the boceprevir arms.

23
Relapsers and non responders Relapsers: defined as patients who initially responded to pegylated interferon/ribavirin (HCV RNA undetectable at week 12/24 and end of therapy), but their HCV RNA relapsed 24 weeks after finishing HCV treatment. Relapsers: defined as patients who initially responded to pegylated interferon/ribavirin (HCV RNA undetectable at week 12/24 and end of therapy), but their HCV RNA relapsed 24 weeks after finishing HCV treatment. Non responders: defined as patients who did not have a 2-log drop in 12 weeks OR did not have an undetectable HCV RNA at week 24. Non responders: defined as patients who did not have a 2-log drop in 12 weeks OR did not have an undetectable HCV RNA at week 24.
, but their HCV RNA relapsed 24 weeks after finishing HCV treatment. Non responders: defined as patients who did not have a 2-log drop in 12 weeks OR did not have an undetectable HCV RNA at week 24. Non responders: defined as patients who did not have a 2-log drop in 12 weeks OR did not have an undetectable HCV RNA at week 24..")
24
PROVE 3: Telaprevir in relapsers TPV/pIFN/RBV 12 wks + pIFN/RBV 12wks = 69% SVR TPV/pIFN/RBV 12 wks + pIFN/RBV 12wks = 69% SVR TPV/pIFN/RBV 24 wks + pIFN/RBV 24 wks = 76% SVR TPV/pIFN/RBV 24 wks + pIFN/RBV 24 wks = 76% SVR TPV 24 wks + pegIFN 24 wks (no RBV)= 42 %SVR TPV 24 wks + pegIFN 24 wks (no RBV)= 42 %SVR Control group: pegIFN/RBV 48 wks = 20% SVR Control group: pegIFN/RBV 48 wks = 20% SVR
= 42 %SVR TPV 24 wks + pegIFN 24 wks (no RBV)= 42 %SVR Control group: pegIFN/RBV 48 wks = 20% SVR Control group: pegIFN/RBV 48 wks = 20% SVR")
25
PROVE 3: Telaprevir in non responders TPV/pIFN/RBV 12 wks + pIFN/RBV 12wks = 39% SVR TPV/pIFN/RBV 12 wks + pIFN/RBV 12wks = 39% SVR TPV/pIFN/RBV 24 wks + pIFN/RBV 24 wks = 38% SVR TPV/pIFN/RBV 24 wks + pIFN/RBV 24 wks = 38% SVR TPV 24 wks + pegIFN 24 wks (no RBV)= 10 %SVR TPV 24 wks + pegIFN 24 wks (no RBV)= 10 %SVR Control group: pegIFN/RBV 48 wks = 9% SVR Control group: pegIFN/RBV 48 wks = 9% SVR
= 10 %SVR TPV 24 wks + pegIFN 24 wks (no RBV)= 10 %SVR Control group: pegIFN/RBV 48 wks = 9% SVR Control group: pegIFN/RBV 48 wks = 9% SVR")
26
RESPOND 2: BOC in relapsers and non-responders Control: pIFN/RBV 48wks = 21% SVR Control: pIFN/RBV 48wks = 21% SVR pIFN/RBV 4wks + BOC/pIFN/RBV 44wks = 66% SVR pIFN/RBV 4wks + BOC/pIFN/RBV 44wks = 66% SVR Response guided therapy arm: Response guided therapy arm: HCV RNA undetectable at wk 8: pIFN/RBV 4wks + BOC/pIFN/RBV 36wks = 86% SVR HCV RNA undetectable at wk 8: pIFN/RBV 4wks + BOC/pIFN/RBV 36wks = 86% SVR HCV RNA detectable at wk 8, but undetectable at wk 12: pIFN/RBV 4wks + BOC/pIFN/RBV 48wks = 40% HCV RNA detectable at wk 8, but undetectable at wk 12: pIFN/RBV 4wks + BOC/pIFN/RBV 48wks = 40%

27
Boceprevir and anemia Anemia (hgb <10) in up to 43% of patients in the BOC arm (vs. 24% in control group) Anemia (hgb <10) in up to 43% of patients in the BOC arm (vs. 24% in control group) Anemia (hgb <8.5) in up to 14% of patients in the BOC arm (vs. 1% in control group) Anemia (hgb <8.5) in up to 14% of patients in the BOC arm (vs. 1% in control group) Erythropoietin use: 41-46% in BOC arm (vs. 21% in control group) Erythropoietin use: 41-46% in BOC arm (vs. 21% in control group) Mean days of EPO use was 130-135 days in BOC arm Mean days of EPO use was 130-135 days in BOC arm Mean days of EPO use was 65 days in control group Mean days of EPO use was 65 days in control group
 Anemia (hgb <10) in up to 43% of patients in the BOC arm (vs. 24% in control group) Anemia (hgb <8.5) in up to 14% of patients in the BOC arm (vs. 1% in control group) Anemia (hgb <8.5) in up to 14% of patients in the BOC arm (vs. 1% in control group) Erythropoietin use: 41-46% in BOC arm (vs. 21% in control group) Erythropoietin use: 41-46% in BOC arm (vs. 21% in control group) Mean days of EPO use was days in BOC arm Mean days of EPO use was days in BOC arm Mean days of EPO use was 65 days in control group Mean days of EPO use was 65 days in control group.")
28
HIV/HCV: Telaprevir phase II TPV/pIFN/RBV 12wks + pIFN/RBV 36wks TPV/pIFN/RBV 12wks + pIFN/RBV 36wks Group 1: not on ART, CD4 >500, HIV VL 500, HIV VL < 100,000 copies/ml Group 2: on ART, CD4 > 300, HIV VL 300, HIV VL < 50 copies/ml Control: pIFN/RBV x 48wks Control: pIFN/RBV x 48wks All patients naïve to HCV therapy

29
HIV/HCV: TPV week 12 data Group 1: no ART Group 1: no ART 71% had eVR vs. 17% of control 71% had eVR vs. 17% of control Group 2: on ART Group 2: on ART Efavirenz based ART: 75 % had eVR vs. 12% of control Efavirenz based ART: 75 % had eVR vs. 12% of control Reyataz based ART: 57% had eVR vs. 12% of control Reyataz based ART: 57% had eVR vs. 12% of control

30
HCV protease inhibitors and ART ART groups: chosen b/c they were most suitable to be used with telaprevir ART groups: chosen b/c they were most suitable to be used with telaprevir Atripla Atripla Reyataz/tenofovir + emtricitabine or lamivudine Reyataz/tenofovir + emtricitabine or lamivudine Telaprevir has moderate drug/drug interactions with several antiretroviral agents: Lopinavir/ritonavir (Kaletra) Darunavir (Prezista) Fosamprenavir (Lexiva)
 Darunavir (Prezista) Fosamprenavir (Lexiva)")
31
HIV/HCV: TPV side effects No cases of HIV breakthrough in ART group No cases of HIV breakthrough in ART group CD4 counts did not change significantly CD4 counts did not change significantly Main side effects: Main side effects: Nausea 35% Nausea 35% Pruritus 35% Pruritus 35% Dizziness 22% Dizziness 22% Anorexia 19% Anorexia 19% Vomiting 19% Vomiting 19%

32
Direct acting antivirals in Clinical testing NS3/4A protease inhibitors (11) NS3/4A protease inhibitors (11) Nucleoside NS5B polymerase inhibitors (3) Nucleoside NS5B polymerase inhibitors (3) Non-nucleoside NS5B polymerase inhibitors (8) Non-nucleoside NS5B polymerase inhibitors (8) NS5A inhibitors (2) NS5A inhibitors (2) NS4B inhibitors (1) NS4B inhibitors (1) Entry inhibitors (1) Entry inhibitors (1)
 NS3/4A protease inhibitors (11) Nucleoside NS5B polymerase inhibitors (3) Nucleoside NS5B polymerase inhibitors (3) Non-nucleoside NS5B polymerase inhibitors (8) Non-nucleoside NS5B polymerase inhibitors (8) NS5A inhibitors (2) NS5A inhibitors (2) NS4B inhibitors (1) NS4B inhibitors (1) Entry inhibitors (1) Entry inhibitors (1)")
Similar presentations

 Fuad AM Hasan Department Of Medicine Faculty of Medicine Kuwait University.>")

, MN Nurse Practitioner CAHN 2013.>")

 infection is one of the most common chronic liver disease and accounts for 8000 to 13,000 deaths each year.>")













