Download presentation
Presentation is loading. Please wait.

1
Nutrition in the Elderly 36.4 Artificial Nutrition Stéphane M. Schneider, MD, PhD Nutritional Support Unit, Nice University Hospital, France

2
Learning objectives Know the most frequent indications for artificial nutrition Know the techniques and outcome Know the indications and results in specific clinical situations Understand the need for ethical elements alongside the medical ones in deciding upon starting an elderly patient on artificial nutrition

3
In which of the following patients is nutritional support NOT warranted? 77 year old previously healthy female with severe dysphagia two weeks after a CVA 69 year male with COPD and esophageal cancer who has lost 10 kilos 65 year old newly edentulous patient who can’t chew a regular diet

5
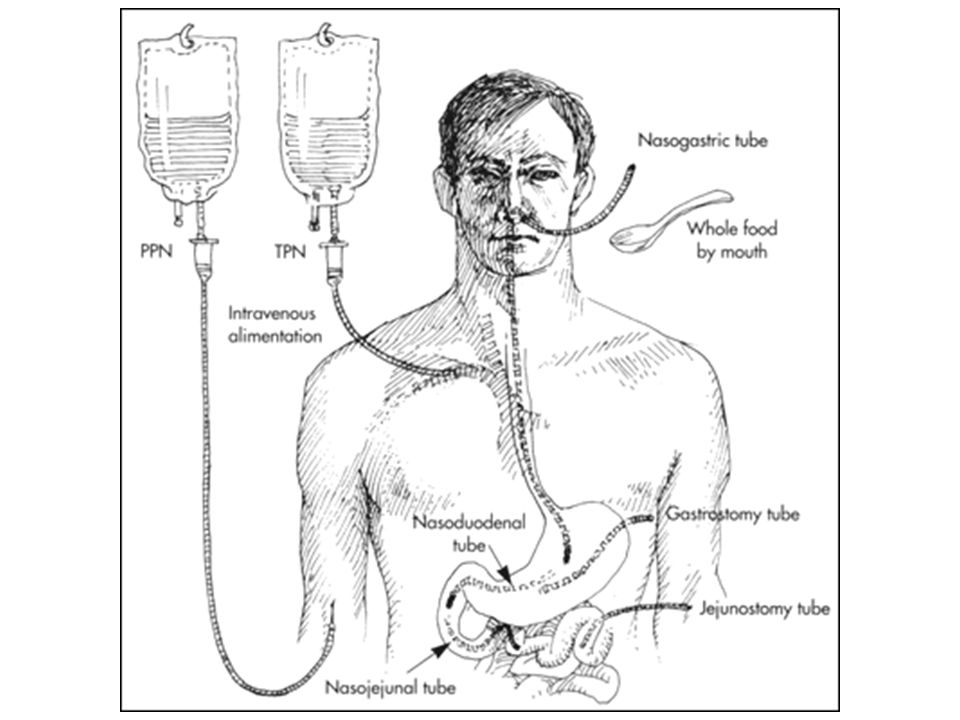
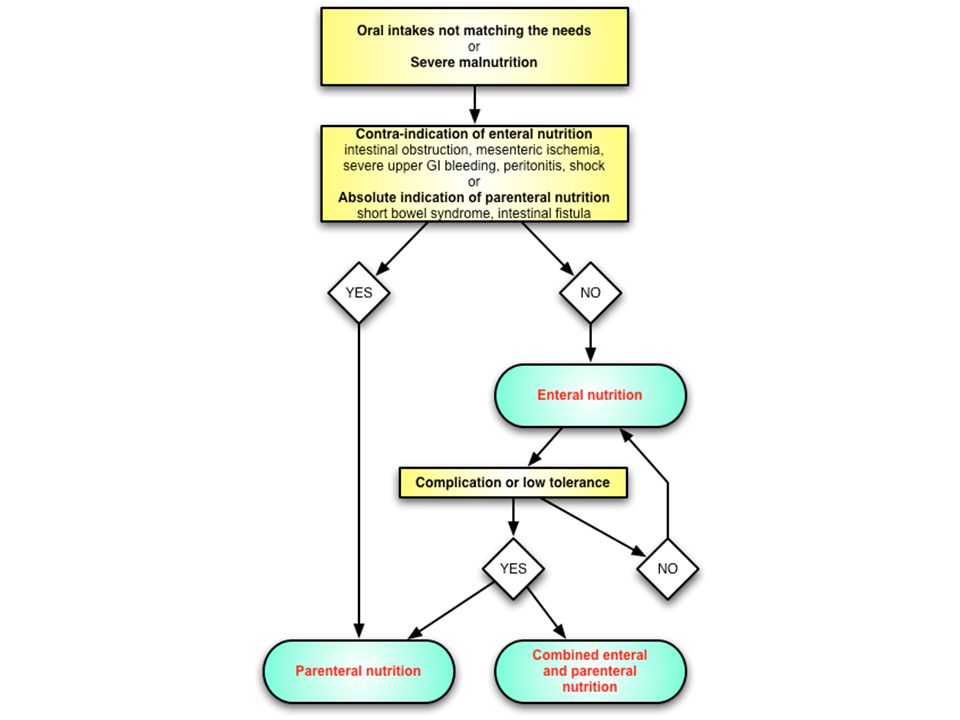
Enteral vs Parenteral? When the gut works use it! Even though using the gut can sometimes be a pain in the ***

6
Benefits of Enteral vs Parenteral Nutrition Maintains morphologic, functional integrity of GI tract Avoids mechanical, metabolic complications of TPN Decreases cost Use of line for other purposes

8
Hypodermoclysis Subcutaneous infusion < 700 mOsm/L et 500 mL/j Water, glucose, minerals, vitamins, trace elements Pros –Easy –No DVT –Free arms –Little monitoring Cons –Infection, pain, œdema –Proofs ?

9
Feeding route (1) Duration –Less than a month –More than a month Risk of aspiration –Standard –Increased Previous aspiration, decreased consciousness, dysphagia, endotracheal intubation, vomiting, supine position Need for digestive surgery
 Duration –Less than a month –More than a month Risk of aspiration –Standard –Increased Previous aspiration, decreased consciousness, dysphagia, endotracheal intubation, vomiting, supine position Need for digestive surgery")
10
Feeding route (2) Short-termLong-term Risk of aspiration StdHighStdHigh ENNGTNJTG tube(G)J tube PNStandard lineTunnelled line / PAC
 Short-termLong-term Risk of aspiration StdHighStdHigh ENNGTNJTG tube(G)J tube PNStandard lineTunnelled line / PAC")
11
Water –30-40 mL/kg/day –Beware heart failure Electrolytes –Add Na to EN formulas –Ca: 1,2 g/day in the elderly Energy –Formulas such as Harris-Benedict –kcal/kg method –Indirect calorimetry Requirements

12
Energy Requirements

13
Protein Requirements

14
Indications Howard and Malone AJCN 1997 Hospital –Secondary anorexia+++ Home

15
Outcome in EN patients Schneider et al. JPEN 2001

16
EN in Geriatrics (1) What are the aims of EN therapy in geriatrics? –Provision of sufficient energy, protein and micronutrients (quality and quantity) –Maintenance or improvement of nutritional status –Maintenance or improvement of function, activity and capacity for rehabilitation –Maintenance or improvement of quality of life –Reduction in morbidity and mortality Volkert et al. Clin Nutr 2006
 –Maintenance or improvement of nutritional status –Maintenance or improvement of function, activity and capacity for rehabilitation –Maintenance or improvement of quality of life –Reduction in morbidity and mortality Volkert et al. Clin Nutr")
17
EN in Geriatrics (2) EN increases energy and nutrient intake in geriatric patients (Ia). PEG feeding is superior to nasogastric feeding in this respect (Ia). EN also maintains or improves nutritional parameters irrespective of the underlying diagnosis. Adequate nutrition is a prerequisite for any functional improvement, although studies are too few and diverse to allow a general statement. The effect of EN on quality of life is uncertain. Volkert et al. Clin Nutr 2006
. EN also maintains or improves nutritional parameters irrespective of the underlying diagnosis. Adequate nutrition is a prerequisite for any functional improvement, although studies are too few and diverse to allow a general statement. The effect of EN on quality of life is uncertain. Volkert et al. Clin Nutr")
18
Good indications for EN Undernutrition Depression Neurological dysphagia Hip fracture Depression Early/moderate dementia

19
Survival in HEN H&N cancerNeurol.Dementia Number7614854 Age657585 BMI19,9 17,4 Reason for HEN Dysphagia (100%)Dysphagia (97%)Anorexia (100%) 1-mo survival88%83%54% 1-yr survival37%41%20% 5-yr survival24%21%3% Schneider et al. JPEN 2001

20
Bad indications for EN Terminal illness Late-stage dementia –Whether Alzheimer’s or not –« Refuses to eat » –« Pulls out his/her NGT » Do not harm: ethical aspects –Patient, family, caregivers, nursing team –Ethics committee

21
Net improvement of nutritional parameters during cyclic enteral nutrition in young and elderly malnourished patients kg 0.0 0.2 0.4 0.6 0.8 1.0 P<0.05 Serum transferrin g/L NS D15D28 <65 years ≥65 years P<0.05 Serum albumin g/L NS D15D28 1.0 3.0 4.0 2.0 0.0 kg P<0.01 P<0.001 Body weight D15D28 0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 0.00 0.02 0.04 0.06 0.08 0.10 P<0.05 Serum prealbumin NS D15D28 g/L Hébuterne et al. JAMA 1995

22
Estimation of energy excess for the gain of 1 kg in young and elderly malnourished patients Hébuterne et al. Personal data

23
Effects of age on energy needs during TPN -50 0 50 100 150 200 250 1020304050607080 20 yr 40 yr 60 yr 80 yr Energy provided (kcal/kg/d) Correlation between daily BCM changes and energy provided during a 2-wk TPN in 325 mildly malnourished patients aged 20- 80. Body cell mass gain (g/d) Shizgal et al. Am J Clin Nutr 1992
 Shizgal et al. Am J Clin Nutr")
24
Key messages Most indications are ideally addressed with enteral nutrition, rarely parenteral nutrition Indications, products and techniques do not differ from adults, but the outcome is worse Prolonged artificial nutrition will be performed at home or in an institution Most demented patients will not benefit from artificial nutrition

Similar presentations
 to Nutritional Support Alan Shenkin Department of Clinical Chemistry University of Liverpool.>")


















