Download presentation
Presentation is loading. Please wait.

1
Optimizing Antibiotic Use in the ICU A Practical Approach to Antimicrobial Stewardship
George Sakoulas, MD UCSD School of Medicine Sharp Memorial Hospital, San Diego, CA July 2013

2
Some Points to Consider
The antibiotic era is 4.5 billion years old Resistance to antibiotics exists in nature before medicine actually discovers or uses them Unlike any other class of medication, antibiotics treat not only the individual, but have societal impacts 70% of antibiotics in USA go to Animal Husbandry

3
Antimicrobial Treatment Considerations
Must be timely: delay in initiation potentially lethal Appropriate: must cover the offending pathogen(s) Administered at adequate dose and intervals consistent with pK/pD parameters Timely streamlining based on clinical response and microbiological data Prompt discontinuation when practical Deresinski S. Clin Infect Dis 2007; 45:S177-S183 Allerberger F et al. Clin Microbiol Infect 2008; 14:
 Administered at adequate dose and intervals consistent with pK/pD parameters. Timely streamlining based on clinical response and microbiological data. Prompt discontinuation when practical. Deresinski S. Clin Infect Dis 2007; 45:S177-S183. Allerberger F et al. Clin Microbiol Infect 2008; 14:")
4
Importance of Initial, Appropriate Antibiotic Therapy
“…selection of initial appropriate antibiotic therapy (ie, getting the antibiotic treatment right the first time) is an important aspect of care for hospitalized patients with serious infections.” – ATS/IDSA Guidelines A Study by Kollef and Colleagues Evaluating the Impact of Inadequate Antimicrobial Therapy on Mortality 60 52* *P<.001 50 42* 40 Hospital Mortality (%) 30 24 18 20 10 All-Cause Mortality Infection-Related Mortality Inadequate antimicrobial treatment (n=169) Adequate antimicrobial treatment (n=486) ATS=American Thoracic Society; IDSA=Infectious Diseases Society of America. Adapted from Kollef MH et al. Chest. 1999;115: ATS/IDSA. Am J Respir Crit Care Med. 2005;171:
 is an important aspect of care for hospitalized patients with serious infections. – ATS/IDSA Guidelines. A Study by Kollef and Colleagues Evaluating the Impact of Inadequate Antimicrobial Therapy on Mortality * *P< * 40. Hospital Mortality (%) All-Cause Mortality. Infection-Related Mortality. Inadequate antimicrobial treatment. (n=169) Adequate antimicrobial treatment. (n=486) ATS=American Thoracic Society; IDSA=Infectious Diseases Society of America. Adapted from Kollef MH et al. Chest. 1999;115: ATS/IDSA. Am J Respir Crit Care Med. 2005;171:")
5
The relationship between mortality and inadequate empirical antibiotic therapy was evaluated in 2 studies of patients with health-care–associated pneumonia.1,2 The relationship between mortality and inadequate antibiotic therapy was examined in a retrospective cohort analysis of 396 culture-positive patients admitted to an urban teaching hospital with a diagnosis of health-care–associated pneumonia between 2003 and All patients included in the analysis remained alive and hospitalized for more than 48 hours. During the 3-year study period, the mortality rate was 30% in the 107 patients receiving inappropriate empirical antibiotic therapy compared with 18% in the 289 patients receiving appropriate initial therapy (P=.013). Subsequent escalation of treatment, which occurred in 40.2% of patients receiving initial inappropriate empirical antibiotic therapy, did not reduce the risk of hospital mortality. The relationship between inadequate initial empirical antibiotic therapy and mortality in adult patients with suspected ventilator-associated pneumonia (VAP) was evaluated in a prospective cohort study at a university-affiliated teaching hospital from February 1996 through February Pathogens responsible for infection in these patients were identified by culture of lower respiratory specimens obtained by mini-BAL (bronchoalveolar lavage). Hospital mortality attributed to VAP was 24% in 51 patients whose initial antibiotic regimen was changed based on mini-BAL culture results compared with a mortality of 8% in patients in whom antibiotic management remained unchanged after mini-BAL culture (P=.018). References 1. Zilberberg MD, Shorr AF, Micek ST, et al. Antimicrobial therapy escalation and hospital mortality among pataients with health-care-associated pneumonia: a single-center experience. Chest. 2008;134(5): 2. Kollef MH, Ward S. The influence of mini-BAL cultures on patient outcomes. Implications for the antibiotic management of ventilator-associated pneumonia. Chest. 1998;113:
. Subsequent escalation of treatment, which occurred in 40.2% of patients receiving initial inappropriate empirical antibiotic therapy, did not reduce the risk of hospital mortality. The relationship between inadequate initial empirical antibiotic therapy and mortality in adult patients with suspected ventilator-associated pneumonia (VAP) was evaluated in a prospective cohort study at a university-affiliated teaching hospital from February 1996 through February Pathogens responsible for infection in these patients were identified by culture of lower respiratory specimens obtained by mini-BAL (bronchoalveolar lavage). Hospital mortality attributed to VAP was 24% in 51 patients whose initial antibiotic regimen was changed based on mini-BAL culture results compared with a mortality of 8% in patients in whom antibiotic management remained unchanged after mini-BAL culture (P=.018). References. 1. Zilberberg MD, Shorr AF, Micek ST, et al. Antimicrobial therapy escalation and hospital mortality among pataients with health-care-associated pneumonia: a single-center experience. Chest. 2008;134(5): Kollef MH, Ward S. The influence of mini-BAL cultures on patient outcomes. Implications for the antibiotic management of ventilator-associated pneumonia. Chest. 1998;113:")
6
The potential relationship between the adequacy of antimicrobial treatment for bloodstream infections and clinical outcomes in the intensive care unit setting was evaluated in a prospective, cohort study from July 1997 to July at an urban teaching hospital. Inadequate therapy was indicated by a positive blood culture from patients who did not receive effective treatment at the time the causative agent and its susceptibility were known. Of 4913 eligible patients, 492 had a bloodstream infection and were included in the study. The mean age of the patients was 57.8 years, and 30.3% were admitted to the intensive care unit following surgery, whereas 69.7% were admitted to the intensive care unit because of a medical diagnosis. The most common bloodstream pathogens included vancomycin-resistant enterococci, Candida species, oxacillin-resistant staphylococci, coagulase-negative staphylococci, and Pseudomonas aeruginosa. A total of 189 patients (38.4%) died during hospitalization. All-cause mortality was 62% in the group given inadequate antimicrobial therapy and 28% in the group given adequate antimicrobial therapy (relative risk, 2.18; 95% confidence interval: 1.77, 2.69; P<.001). Infection-related mortality was also significantly greater in the group given inadequate treatment (30%) than in the group given adequate treatment (12%) (P<.001). Multivariate analysis revealed that inadequate antimicrobial treatment was the most important risk factor for hospital mortality (P<.001). Reference Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment on bloodstream infections on patient outcomes in the ICU setting. Chest ;118:
 died during hospitalization. All-cause mortality was 62% in the group given inadequate antimicrobial therapy and 28% in the group given adequate antimicrobial therapy (relative risk, 2.18; 95% confidence interval: 1.77, 2.69; P<.001). Infection-related mortality was also significantly greater in the group given inadequate treatment (30%) than in the group given adequate treatment (12%) (P<.001). Multivariate analysis revealed that inadequate antimicrobial treatment was the most important risk factor for hospital mortality (P<.001). Reference. Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment on bloodstream infections on patient outcomes in the ICU setting. Chest. 2000;118:")
7
The potential relationship between the adequacy of antimicrobial treatment for bloodstream infections (BSIs) and clinical outcomes in the intensive care unit setting was evaluated in a prospective, cohort study from July 1997 to July 1999 at an urban teaching hospital. Inadequate therapy was indicated by a positive blood culture from patients who did not receive effective treatment at the time the causative agent and its susceptibility were known. Of the 492 patients identified as having a BSI during this period, 189 (38.4%) died during hospitalization. The difference in overall mortality rate between the 147 patients receiving inadequate antimicrobial treatment for their BSI and the 345 receiving adequate therapy, 61.9% vs 28.4%, was statistically significant (P<.001). A statistically significant relationship was also found between the rates of inadequate antimicrobial treatment for individual microorganisms and their associated rates of hospital mortality (P=.006). Inadequate therapy and high mortality rates were primarily driven by vancomycin-resistant enterococci (VRE), Candida species, and oxacillin-resistant Staphylococcus aureus (ORSA). Rates of inadequate antimicrobial therapy were >95% in patients with BSIs attributable to VRE and Candida species. These patients also had the highest rates of hospital mortality, approximately 60%. The rate of inadequate treatment was approximately 35% and the mortality rate was approximately 40% in patients with BSI caused by ORSA. The rate of inadequate treatment in patients with infections attributable to Pseudomonas aeruginosa was <20% but mortality in this group was approximately 50%. Although P. aeruginosa, Klebsiella species, and Escherichia coli were all associated with low rates of inadequate therapy at the time of this study in the late 1990s, this pattern can be expected to change over time as more resistant pathogens emerge in the institution where the study was performed and antibiotic therapy remains the same. Reference Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment on bloodstream infections on patient outcomes in the ICU setting. Chest ;118(1):
. Inadequate therapy and high mortality rates were primarily driven by vancomycin-resistant enterococci (VRE), Candida species, and oxacillin-resistant Staphylococcus aureus (ORSA). Rates of inadequate antimicrobial therapy were >95% in patients with BSIs attributable to VRE and Candida species. These patients also had the highest rates of hospital mortality, approximately 60%. The rate of inadequate treatment was approximately 35% and the mortality rate was approximately 40% in patients with BSI caused by ORSA. The rate of inadequate treatment in patients with infections attributable to Pseudomonas aeruginosa was <20% but mortality in this group was approximately 50%. Although P. aeruginosa, Klebsiella species, and Escherichia coli were all associated with low rates of inadequate therapy at the time of this study in the late 1990s, this pattern can be expected to change over time as more resistant pathogens emerge in the institution where the study was performed and antibiotic therapy remains the same. Reference. Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment on bloodstream infections on patient outcomes in the ICU setting. Chest. 2000;118(1):")
8
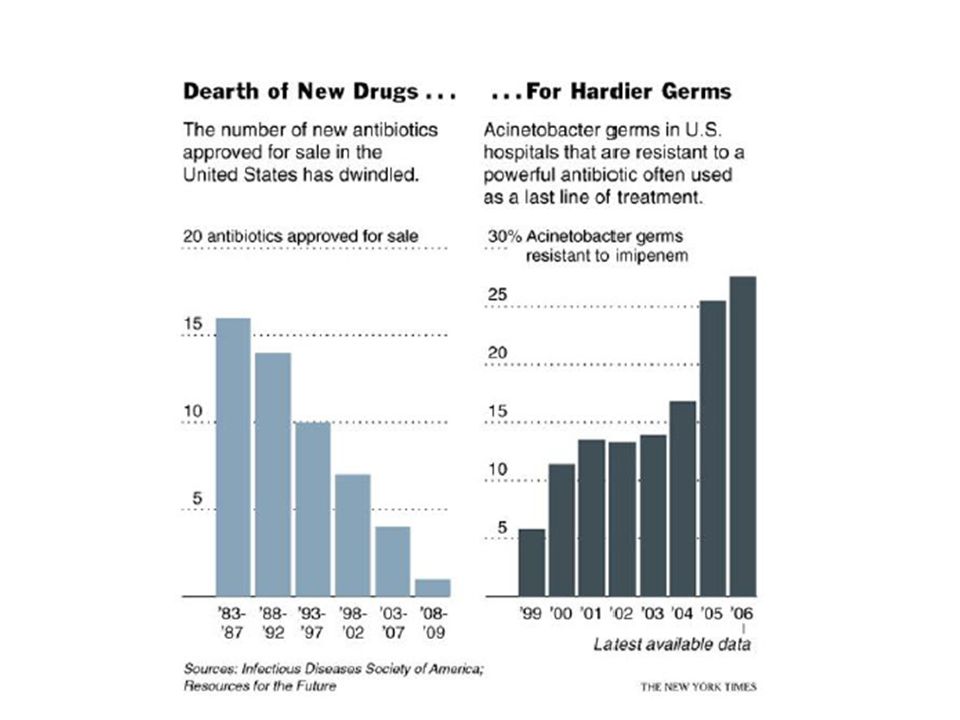
Discovery of New Antibiotic Classes

9
Novel Antibiotic Development

12
Geographic Distribution of KPC Producers in USA

13
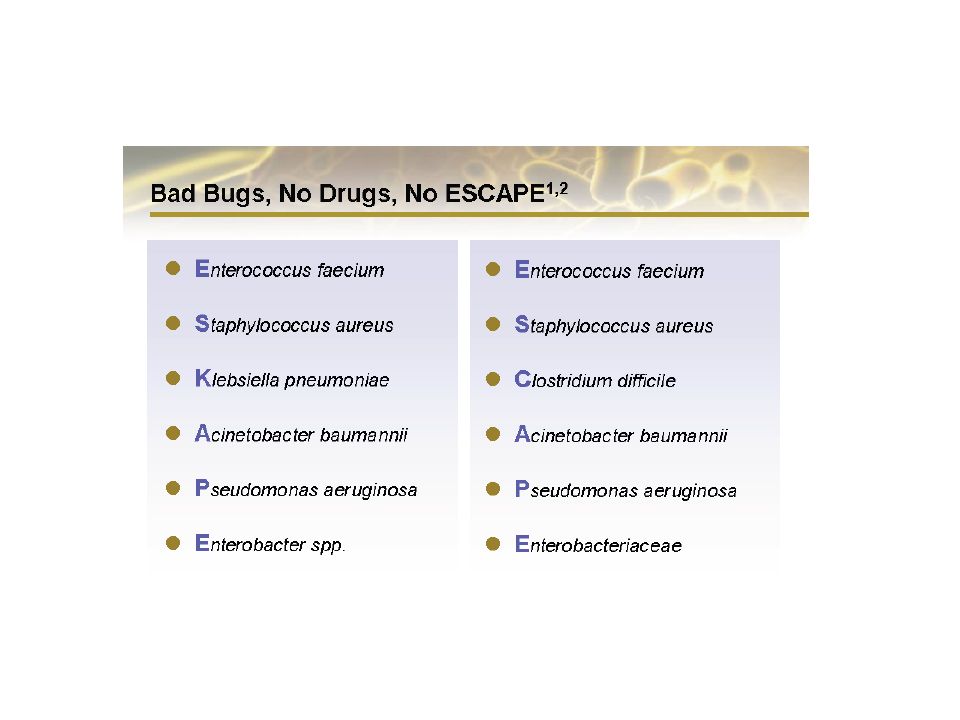
ESKAPE and Mortality in Bacteremia
VRE (n=683) vs VSE (n=931) OR 2.52 ( ) Ref 1 MRSA (n=382) vs MSSA (n=433) 11.8% vs 5.1% (p< 0.001) Ref 2 Klebsiella pneumoniae 52% vs. 29% (p=0.007) Ref 3 ESBL (n=48) vs non-ESBL (n=99) Acinetobacter baumanii 58% vs. 28% (p< 0.05) Ref 4 Imipenam R (n=40) vs S (n=40) Pseudomonas aeruginosa 21% vs. 12% (p=0.08) Ref 5 MDR (n=82) vs non-MDR (n=82) REFERENCES Diaz-Granados et al. Clin Infect Dis 2005;41: Melzer M et al. Clin Infect Dis 2003; 37: Tumbarello M et al. Antimicrob Agents Chemother 2006; 50: Kwon K et al. J Antimicrob Chemother 2007; 59: Aloush V et al. Antimicrob Agents Chemother 2006; 50:
 vs VSE (n=931) OR 2.52 ( ) Ref 1. MRSA (n=382) vs MSSA (n=433) 11.8% vs 5.1% (p< 0.001) Ref 2. Klebsiella pneumoniae 52% vs. 29% (p=0.007) Ref 3. ESBL (n=48) vs non-ESBL (n=99) Acinetobacter baumanii 58% vs. 28% (p< 0.05) Ref 4. Imipenam R (n=40) vs S (n=40) Pseudomonas aeruginosa 21% vs. 12% (p=0.08) Ref 5. MDR (n=82) vs non-MDR (n=82) REFERENCES. Diaz-Granados et al. Clin Infect Dis 2005;41: Melzer M et al. Clin Infect Dis 2003; 37: Tumbarello M et al. Antimicrob Agents Chemother 2006; 50: Kwon K et al. J Antimicrob Chemother 2007; 59: Aloush V et al. Antimicrob Agents Chemother 2006; 50:")
14
Clostridium Dificile Poor Hand Hygiene Poor Environmental Cleanliness
Mechanical scrub with soap and water Poor Environmental Cleanliness Indiscriminate use of antibiotics In summary, to prevent CDAD, -don’t make them: use antibiotics carefully -don’t spread them: wash hands, keep the environment clean

15
Inpatient Cases Have Increased Significantly Since 2001
The source data for this figure are from the Healthcare Cost and Utilization Project (HCUP). The HCUP database is compiled from community hospitals, defined as short-term, non-Federal, general and other hospitals, excluding hospital units of other institutions (eg, prisons). Historical data were drawn from the 1993–2005 HCUP Nationwide Inpatient Sample (NIS). The HCUP (NIS) is a nationwide database of inpatient stays that is nationally representative of all community hospitals (ie, short-term, non-Federal, non-rehabilitation hospitals). This figure illustrates the change in C. difficile-associated disease-related hospital discharges from 1993 through From 1993 to 2001, the total number of hospital discharges increased by 74%, from to per year. During the following 4-year period from 2001 to 2005, the rate increased over 100% to 301,200. C. difficile-associated disease was not the primary diagnosis for most of these cases, particularly in the later years. The use of Clostridium difficile-associated disease rather than diarrhea is consistent with most epidemiological data, which are based on the only ICD-9-CM (International Classification of Diseases, Ninth Edition, Clinical Modifications) code for C. difficile-related disease, This code is defined as intestinal infection due to Clostridium difficile. Reference: Elixhauser A, Jhung M. Clostridium difficile-associated disease in US hospitals, 1993−2005. HCUP Statistical Brief. April 2008.
. The HCUP database is compiled from community hospitals, defined as short-term, non-Federal, general and other hospitals, excluding hospital units of other institutions (eg, prisons). Historical data were drawn from the 1993–2005 HCUP Nationwide Inpatient Sample (NIS). The HCUP (NIS) is a nationwide database of inpatient stays that is nationally representative of all community hospitals (ie, short-term, non-Federal, non-rehabilitation hospitals). This figure illustrates the change in C. difficile-associated disease-related hospital discharges from 1993 through From 1993 to 2001, the total number of hospital discharges increased by 74%, from to per year. During the following 4-year period from 2001 to 2005, the rate increased over 100% to 301,200. C. difficile-associated disease was not the primary diagnosis for most of these cases, particularly in the later years. The use of Clostridium difficile-associated disease rather than diarrhea is consistent with most epidemiological data, which are based on the only ICD-9-CM (International Classification of Diseases, Ninth Edition, Clinical Modifications) code for C. difficile-related disease, This code is defined as intestinal infection due to Clostridium difficile. Reference: Elixhauser A, Jhung M. Clostridium difficile-associated disease in US hospitals, 1993−2005. HCUP Statistical Brief. April")
16
Marked Increase in Mortality Since 2001
C. difficile-associated disease-related deaths were identified by using multiple cause-of-death data from national mortality records for 1999–2004. C. difficile-associated disease-related deaths were defined as all deaths for which the underlying cause or any contributing causes included the ICD-10 code A04.7 (enterocolitis due to C. difficile). For the period 1999–2004, C. difficile-associated disease was reported as a cause of death for persons and as the underlying cause for (59%) of these deaths. Over this same period, all other reported intestinal infectious diseases combined (ICD-10 codes A00 to A09, excluding A047) accounted for 3256 deaths. The overall rate of C. difficile-related deaths during the study period was 12.2 deaths per million population. Mortality rates related to C. difficile-associated disease increased from 5.7 deaths per million in 1999 to 23.7 deaths per million in Based on regression analysis of the study period, mortality rates increased by 35% per year. The new, more virulent BI strain of C. difficile may be responsible for the increased risk of recurrence and mortality of C. difficile-associated disease in the US and Canada. References: Redelings MD, Sorvillo F, Mascola L. Increase in Clostridium difficile-related mortality rates, US, Emerg Infect Dis. 2007;13(9):1417–1419. Kuijper EJ, Coignard B, Tüll P, et al. Emergence of Clostridium difficile-associated disease in North America and Europe. European Society of Clinical Microbiology and Infectious Diseases. Abstract
. For the period 1999–2004, C. difficile-associated disease was reported as a cause of death for persons and as the underlying cause for (59%) of these deaths. Over this same period, all other reported intestinal infectious diseases combined (ICD-10 codes A00 to A09, excluding A047) accounted for 3256 deaths. The overall rate of C. difficile-related deaths during the study period was 12.2 deaths per million population. Mortality rates related to C. difficile-associated disease increased from 5.7 deaths per million in 1999 to 23.7 deaths per million in Based on regression analysis of the study period, mortality rates increased by 35% per year. The new, more virulent BI strain of C. difficile may be responsible for the increased risk of recurrence and mortality of C. difficile-associated disease in the US and Canada. References: Redelings MD, Sorvillo F, Mascola L. Increase in Clostridium difficile-related mortality rates, US, Emerg Infect Dis. 2007;13(9):1417–1419. Kuijper EJ, Coignard B, Tüll P, et al. Emergence of Clostridium difficile-associated disease in North America and Europe. European Society of Clinical Microbiology and Infectious Diseases. Abstract")
17
What is Antimicrobial Stewardship?
Systematic approach to optimize clinical outcomes while minimizing consequence of antibiotic use Toxicity Selection of resistance Selection of virulent organisms Clostridium dificile Combine with comprehensive infection control to limit emergence and transmission of resistance Reduce healthcare costs without adversely impacting care Bottom line-STREAMLINE therapy Dellit T et al. Clin Infect Dis 2007; 44:

18
Antimicrobial stewardship is a multifaceted approach to improving antimicrobial use. The goals of antimicrobial stewardship include combating the emergence of bacterial resistance, improving clinical outcomes, and controlling costs. Reference Lawrence KL, Kollef MH. Antimicrobial stewardship in the intensive care unit. Advances and obstacles. Am J Respir Crit Care Med. 2009;179:

19
Stewardship Strategies in the Prescribing Workflow

20
California SB 739-HAI Initiative
Control and report healthcare-acquired infections (eg. Central line insertion practice) Antibiotic stewardship included “By January 1, 2008, [CDPH] shall take all of the following actions to protect against health care associated infections (HAI) in general acute care hospitals statewide: Require that general acute care hospitals develop a process for evaluating the judicious use of antibiotics, the results of which shall be monitored jointly by appropriate representatives and committees involved in quality improvement activities.”
 Antibiotic stewardship included. By January 1, 2008, [CDPH] shall take all of the following actions to protect against health care associated infections (HAI) in general acute care hospitals statewide: Require that general acute care hospitals develop a process for evaluating the judicious use of antibiotics, the results of which shall be monitored jointly by appropriate representatives and committees involved in quality improvement activities.")
21
Economic Considerations for Antibiotic Stewardship
Antibiotic use restriction and costs should not be the only focus Antibiotic costs are a small percentage of treatment costs Costs from hospital length of stay, total hospital costs, and infection prevention should be considered Return to productivity

22
General Antimicrobial Prescribing Principles
Day 1: Empiric Antibiotics Need rapid diagnotics Mixing vs. Cycling Day 3: DE-ESCALATION What antibiotics are being prescribed? What do the cultures show? Is there infection? LEUKOCYTOSIS = INFECTION Fever is not necessarily due to infection What is the clinical picture?

23
DE-ESCALATION DISCONTINUATION STOP WHEN YOU ARE DONE!!

24
No more recurrent infections More antibiotic-free days
Kaplan-Meier Estimates of the Probability of Survival Probability of survival is for the 60 days after ventilator-assisted pneumonia onset as a function of the duration of antibiotics Figure 2. Kaplan-Meier Estimates of the Probability of Survival Probability of survival is for the 60 days after ventilator-assisted pneumonia onset as a function of the duration of antibiotic administration. No excess mortality No more recurrent infections More antibiotic-free days Chastre, J. et al. JAMA 2003;290:

25
Antibiotic “Sink” The “UTI”
UTI requires at least 1 of the following Pyuria (>10 WBC/hpf) Symptoms (dysuria, hematuria, urgency) BACTERIURIA IS NOT A UTI QUANTITATIVE BACTERIURIA (CFU/ML) IS IRRELEVANT The Only Patients in whom bacteriuria requires therapy Pregnancy Renal transplant patients Pre-op Patient
 Symptoms (dysuria, hematuria, urgency) BACTERIURIA IS NOT A UTI. QUANTITATIVE BACTERIURIA (CFU/ML) IS IRRELEVANT. The Only Patients in whom bacteriuria requires therapy. Pregnancy. Renal transplant patients. Pre-op Patient.")
26
GENERAL UTI SUMMARY No need to treat Treat UTI-> 3 days
Nitrites Bacteriuria other than pregnancy, transplant Treat UTI-> 3 days Pyelonephritis -> 2 weeks

27
Biomarker: Procalcitonin (PCT)
116 amino acid peptide, MW 13 kD; product of CALC-I gene PCT is normally produced, enzymatically processed into calcitonin, and stored in granules in the neuroendocrine C cells of the thyroid Serum concentrations of PCT < 0.5 ng/mL Under condition of infection, PCT is produced constitutively by all cells Direct toxins or LPS Indirect stimualtion by pro-inflammatory cytokines: IL-b, IL-6, TNF-a Serum concentrations up to 2000X increase First described to be elevated in staphylococcal TSS in 1983 Subsequently considered a potential parameter of infection in 1993

28
PCT Kinetics Procalcitonin (PCT) increases after 2-3 hours after induction e.g. by endotoxin May increase to levels up to several hundred nanogram per ml in severe sepsis and septic shock. After successful treatment intervention the procalcitonin value decreases, indicating a positive prognosis Persistingly high or even further increasing levels are indicators for poor prognosis. Levels then rise rapidly, reaching a plateau after 6-12 hours. PCT concentrations remain high for up to 48 hours, falling to their baseline values within the following 2 days. The half-life is about 20 to 24 hours. Brunkhorst F.M. et al., Intens Care Med 1998, 24:

29
PCT Concentration Spectrum

30
Duration of Antibiotics for CAP
Christ-Crain M et al. Am J Respir Crit Care Med Apr 7; Christ-Crain M & Müller B, Swiss Med Wkly 2005, 135:

31
Outcomes: Procalcitonin in CAP
Christ-Crain M et al. Am J Resp Crit Care Med 2006; 174: 84-93

32
PCT and Sepsis: Less Antibiotics, No Impact on Survival
Bouadma L et al. Lancet 2010; 375:

33
PCT DOES NOT Replace Routine Microbiology Or Clinical Judgment
PCT may not elevated in some bloodstream infections S. aureus bacteremia Enterococcus bacteremia Subacute bacterial endocarditis Candidemia

34
Where Else Are Molecular Rapid Diagnostics Needed and Used?
Screening for resistant pathogens RAPID Organism identification in sterile body fluids Fastidious organisms Prior antibiotics negate cultures RAPID Susceptibility report Risk Stratification of Patients More expensive more potent antibiotics perhaps for the sicker patients

35
A number of US Food and Drug Administration–cleared molecular assays are available for rapid microbial identification and susceptibility determination. In a polymerase chain reaction assay, a target sequence is amplified using 2 flanking primers. Amplification of the target sequence is detected by instrumentation through the use of a fluorescently labeled probe.1 Hybridization of fluorescently labeled peptide nucleic acid DNA analogue probes to rRNA in intact bacteria is detected by fluorescence microscopy in peptide nucleic acid fluorescence in situ hybridization.1 Bacterial species-specific phage amplification is measured as a surrogate marker for bacterial viability in a bacteriophage immunoassay.2 References 1. Mothershed EA, Whitney AM. Nucleic acid-based methods for the detection of bacterial pathogens: present and future considerations for the clinical laboratory. Clin Chim Acta. 2006;363(1-2): 2. Smith D. Bacteriophage amplification for bacterial identification. IVD Technology. 2010;16(7):
: Smith D. Bacteriophage amplification for bacterial identification. IVD Technology. 2010;16(7):")
36
US Food and Drug Administration–cleared rapid microbial identification methods are available for earlier organism identification and susceptibility determination compared with standard identification and susceptibility testing methods. Polymerase chain reaction assays are available for the identification of Gram-positive and Gram-negative bacteria, including Staphylococcus aureus, methicillin-resistant S. aureus, Group B streptococci, and Neisseria gonorrhea. Polymerase chain reaction results are available within 1 to 2 hours of obtaining a specimen.1,2 Peptide nucleic acid fluorescence in situ hybridization methods are available for the identification of Gram-positive and Gram-negative bacteria, including S. aureus, coagulase-negative staphylococci, Escherichia coli, Pseudomonas aeruginosa, Enterococcus faecalis, Enterococcus faecium, Acinetobacter spp., and the yeast Candida albicans, Candida parapsilosis, Candida tropicalis, Candida glabrata, and Candida krusei within 1 to 2 hours.1-3 An available bacteriophage assay can identify methicillin-resistant S. aureus and methicillin-susceptible S. aureus from blood cultures in 5 hours.4 References 1. Mothershed EA, Whitney AM. Nucleic acid-based methods for the detection of bacterial pathogens: present and future considerations for the clinical laboratory. Clin Chim Acta. 2006;363(1-2): 2. Tenover FC. Potential impact of rapid diagnostic tests on improving antimicrobial use. Ann NY Acad Sci. 2010;1213:70-80. 3. Peleg AY, Tilahun Y, Fiandaca MJ, et al. Utility of peptide nucleic acid fluorescence in situ hybridization for rapid detection of Acinetobacter spp. and Pseudomonas aeruginosa. J Clin Microbiol. 2009;47(3): 4. Smith D. Bacteriophage amplification for bacterial identification. IVD Technology. 2010;16(7):28-35.
: Tenover FC. Potential impact of rapid diagnostic tests on improving antimicrobial use. Ann NY Acad Sci. 2010;1213: Peleg AY, Tilahun Y, Fiandaca MJ, et al. Utility of peptide nucleic acid fluorescence in situ hybridization for rapid detection of Acinetobacter spp. and Pseudomonas aeruginosa. J Clin Microbiol. 2009;47(3): Smith D. Bacteriophage amplification for bacterial identification. IVD Technology. 2010;16(7):")
37
Results of standardized antimicrobial susceptibility testing for most bacterial species may not be available until 96 hours after collection of a clinical specimen for culture.1 Between 18 and 48 hours may be needed to isolate the pathogen, depending on the growth requirements of the organism, and an additional 8 to 48 hours may be required to perform and report the results of the susceptibility test. Rapid molecular identification methods (eg, polymerase chain reaction [PCR] assays, peptide nucleic acid fluorescence in situ hybridization [PNA FISH], and bacteriophage), however, can yield results within 1 to 5 hours of obtaining a specimen either from a skin infection site or positive blood culture, thus allowing earlier initiation of optimal antimicrobial therapy.1-4 References 1. Tenover FC. Potential impact of rapid diagnostic tests on improving antimicrobial use. Ann NY Acad Sci. 2010;1213:70-80. 2. Mothershed EA, Whitney AM. Nucleic acid-based methods for the detection of bacterial pathogens: present and future considerations for the clinical laboratory. Clin Chim Acta. 2006;363(1-2): 3. Peleg AY, Tilahun Y, Fiandaca MJ, et al. Utility of peptide nucleic acid fluorescence in situ hybridization for rapid detection of Acinetobacter spp. and Pseudomonas aeruginosa. J Clin Microbiol. 2009;47(3): 4. Smith D. Bacteriophage amplification for bacterial identification. IVD Technology. 2010;16(7):28-35.
, however, can yield results within 1 to 5 hours of obtaining a specimen either from a skin infection site or positive blood culture, thus allowing earlier initiation of optimal antimicrobial therapy.1-4. References. 1. Tenover FC. Potential impact of rapid diagnostic tests on improving antimicrobial use. Ann NY Acad Sci. 2010;1213: Mothershed EA, Whitney AM. Nucleic acid-based methods for the detection of bacterial pathogens: present and future considerations for the clinical laboratory. Clin Chim Acta. 2006;363(1-2): Peleg AY, Tilahun Y, Fiandaca MJ, et al. Utility of peptide nucleic acid fluorescence in situ hybridization for rapid detection of Acinetobacter spp. and Pseudomonas aeruginosa. J Clin Microbiol. 2009;47(3): Smith D. Bacteriophage amplification for bacterial identification. IVD Technology. 2010;16(7):")
38
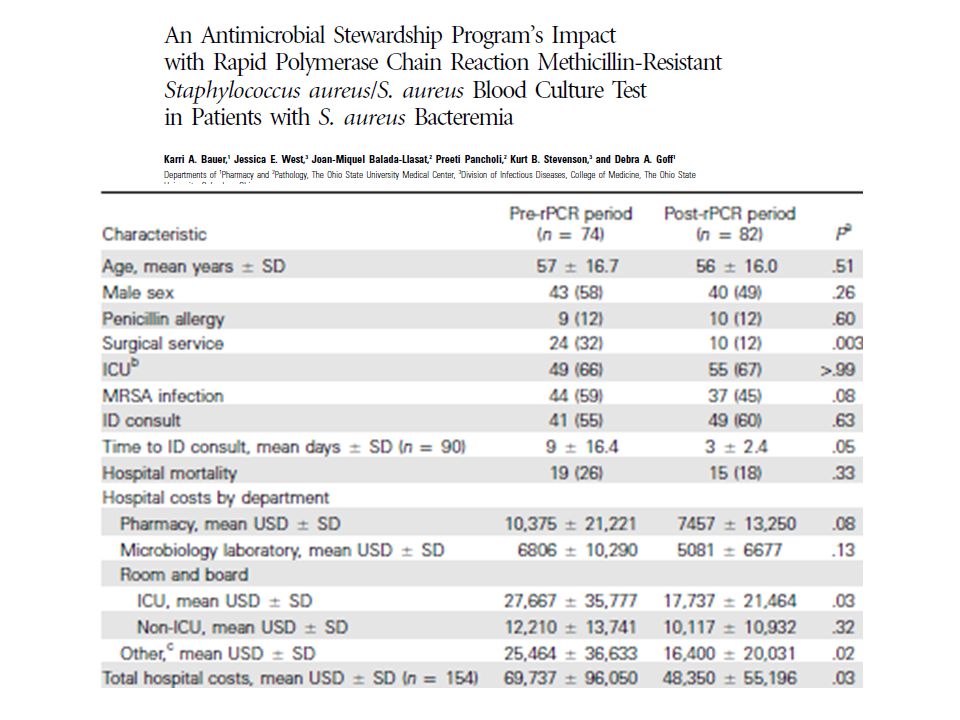
In a prospective, observational study, recurrent bacteremia was assessed in 448 evaluable patients. Patients were followed for 6 months after the completion of therapy. Of these patients, 298 had methicillin-susceptible Staphylococcus aureus (MSSA) and 146 had methicillin-resistant S. aureus (4 had unknown susceptibility). In a subset of patients excluding those with endocarditis as well as those who did not receive at least 18 days of therapy within the first 14 days after the initial positive blood culture, a total of 18 patients with MSSA bacteremia were given nafcillin and 70 were given vancomycin. Persistent bacteremia was defined as the occurrence of positive blood cultures despite receipt of antistaphylococcal antibiotic therapy. Recurrence was defined as the return of S. aureus bacteremia after documentation of negative blood cultures or clinical improvement upon completion of antistaphylococcal therapy. Recurrence was further subclassified as reinfection or relapse based on pulsed-field gel electrophresis (PFGE; relapse is the same PFGE profile and reinfection is a different PFGE profile). Bacteriologic failure was defined as a relapse or persistent bacteremia lasting >7 days. As shown in the slide, nafcillin was more effective than vancomycin in preventing bacteriologic failure (P=.058). Persistent bacteremia after 3 days of treatment was observed in 6% of patients treated with nafcillin and in 21% treated with vancomycin, whereas persistent bacteremia after 7 days of treatment was observed in none of the patients treated with nafcillin and 11% treated with vancomycin. Relapse was observed in 7% of patients treated with vancomycin, and bacteriologic failure was observed in 19% of patients given vancomycin. These analyses excluded patients with endocarditis and patients who did not receive at least 10 days of therapy within the first 14 days from the initial blood culture. Factors predisposing patients to relapse were further evaluated in a logistic model multivariate analysis. In this analysis, only endocarditis (P<.009; odds ratio, 7.6) and vancomycin treatment (P=.048; odds ratio, 6.5) were predictive of relapse. Reference Chang FY, Peacock JE Jr, Musher DM, et al. Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study. Medicine (Baltimore). 2003;82(5):
. Persistent bacteremia after 3 days of treatment was observed in 6% of patients treated with nafcillin and in 21% treated with vancomycin, whereas persistent bacteremia after 7 days of treatment was observed in none of the patients treated with nafcillin and 11% treated with vancomycin. Relapse was observed in 7% of patients treated with vancomycin, and bacteriologic failure was observed in 19% of patients given vancomycin. These analyses excluded patients with endocarditis and patients who did not receive at least 10 days of therapy within the first 14 days from the initial blood culture. Factors predisposing patients to relapse were further evaluated in a logistic model multivariate analysis. In this analysis, only endocarditis (P<.009; odds ratio, 7.6) and vancomycin treatment (P=.048; odds ratio, 6.5) were predictive of relapse. Reference. Chang FY, Peacock JE Jr, Musher DM, et al. Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study. Medicine (Baltimore). 2003;82(5):")
40
Antibiotic Stewardship Must Coincide with Infection Control/Prevention
Optimal management of vascular and urinary catheters Prevention of LRTI Control Hand hygiene Contact precautions Active surveillance Education Environmental cleaning Improved communication between facilities

41
Mindset of MD’s: What Influences Antibiotic Prescribing?

42
Conclusions Physicians needs better tools on how to initiate and stop antibiotics Diagnostics Education Support systems Stewardship teams are just one step to regulate antibiotic prescribing The attitude of prescribing antimicrobials must switch from one of a right to one of a privilege Erase the “potential benefit>> potential harm” mindset of prescribing antibiotics De-escalate to narrower agents ASAP Cut duration of antibiotics Early stop for non-infections Short high dose course in cases of infection

Similar presentations