Download presentation
Presentation is loading. Please wait.

1
Estimating the moral hazard effect of prescription drug coverage AcademyHealth Annual Meeting Boston, MA June 28, 2005 Department of Health Policy and Administration

2
Dennis G. Shea, Ph.D. Department of Health Policy and Administration Center for Health Care Policy and Research Penn State Joseph V. Terza, Ph.D. Center for Health Economic and Policy Studies Department of Health Administration and Policy Medical University of South Carolina Bruce C. Stuart, Ph.D. Peter Lamy Center of Drug Therapy and Aging University of Maryland School of Pharmacy Becky Briesacher, Ph.D. University of Massachusetts Medical School Division of Geriatric Medicine Funding for this work was provided by The Commonwealth Fund

3
Introduction and Research Question Two critical economic issues, selection and moral hazard, will play a fundamental role in the success of Medicare Part D All estimates of the effects of Part D made very similar assumptions about moral hazard. Is this assumption appropriate? Department of Health Policy and Administration

4
Why Prior Estimates Could Need an Update Age of Data Sample Representation Detail on variables Econometric Advances Department of Health Policy and Administration

5
Data 1999 Medicare Current Beneficiary Survey Community residing, full-year enrolled Sample includes only those with full-year prescription drug coverage and those with no prescription drug coverage (N=5,270) Key Variables –Dependent: Total annual prescription drug spending –Independent: Full-year prescription drug coverage –Health Status: Diagnostic Cost Group/Hierarchical Coexisting Condition (DCG/HCC) risk adjuster Department of Health Policy and Administration
 Key Variables –Dependent: Total annual prescription drug spending –Independent: Full-year prescription drug coverage –Health Status: Diagnostic Cost Group/Hierarchical Coexisting Condition (DCG/HCC) risk adjuster Department of Health Policy and Administration")
6
Methods Three-stage variant of two-stage residual inclusion (2SRI) estimator discussed in Terza (2005) (http:\\people.musc.edu\~terza\glmendo4.pdf) –Estimate probit on insurance coverage and use those estimates to derive residual estimate of unknown independent variables (x u ) that effect use –Estimate first part of two part model with probit including estimated residual –Estimate second part of two part model with nonlinear least squares exponential regression model, again, including estimated residual as a regressor Department of Health Policy and Administration
 estimator discussed in Terza (2005) ( –Estimate probit on insurance coverage and use those estimates to derive residual estimate of unknown independent variables (x u ) that effect use –Estimate first part of two part model with probit including estimated residual –Estimate second part of two part model with nonlinear least squares exponential regression model, again, including estimated residual as a regressor Department of Health Policy and Administration")
7
Methods: An Example Department of Health Policy and Administration Person Y 0 (x * p =0) Y 1 (x * p =1) (x p =0) 1 2 3 4 5 (y:x p =0) $400 $550 $450 $300 $650 Counterfactual $800 $1200 $1000 $900 $750 (x p =1) 6 7 8 9 10 Counterfactual $450 $250 $700 $300 $600 (y:x p =1) $1300 $900 $750 $1400 $1000
 Y 1 (x * p =1) (x p =0) (y:x p =0) $400 $550 $450 $300 $650 Counterfactual $800 $1200 $1000 $900 $750 (x p =1) Counterfactual $450 $250 $700 $300 $600 (y:x p =1) $1300 $900 $750 $1400 $1000")
8
Results: Spending Average spending in counterfactual no drug coverage model is $401 Average spending in counterfactual complete drug coverage model is $1,112 Policy effect of expanding drug coverage is $711 Elasticity estimate based on this model is -0.93 Department of Health Policy and Administration

9
Results: 2SRI and Endogeneity Risk adjuster (DCG/HCC) offers opportunity to test methods DCG/HCC is highly significant in models indicating it captures significant health effects not captured by health status, conditions, ADLs, and other included health variables Re-ran regressions excluding risk adjuster as regressor, thus creating unmeasured health effects in model Endogeneity clearly evident in models as coefficients on x u are significant But, parameter estimates on prescription drug coverage variable do not change significantly, indicating 2SRI captures the unmodeled DCG/HCC effects. Department of Health Policy and Administration

10
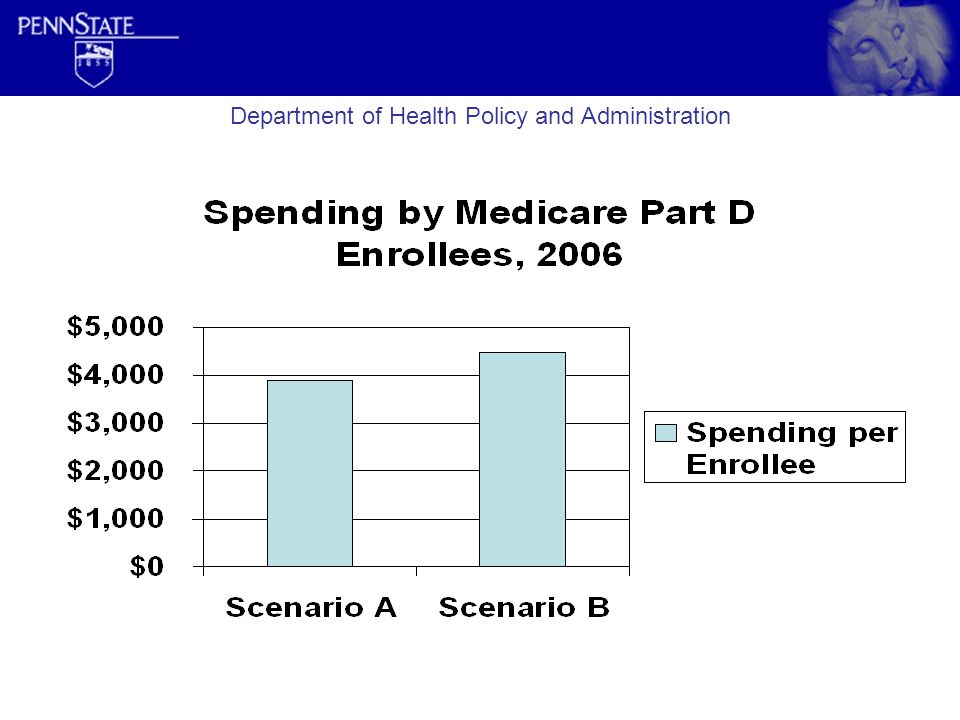
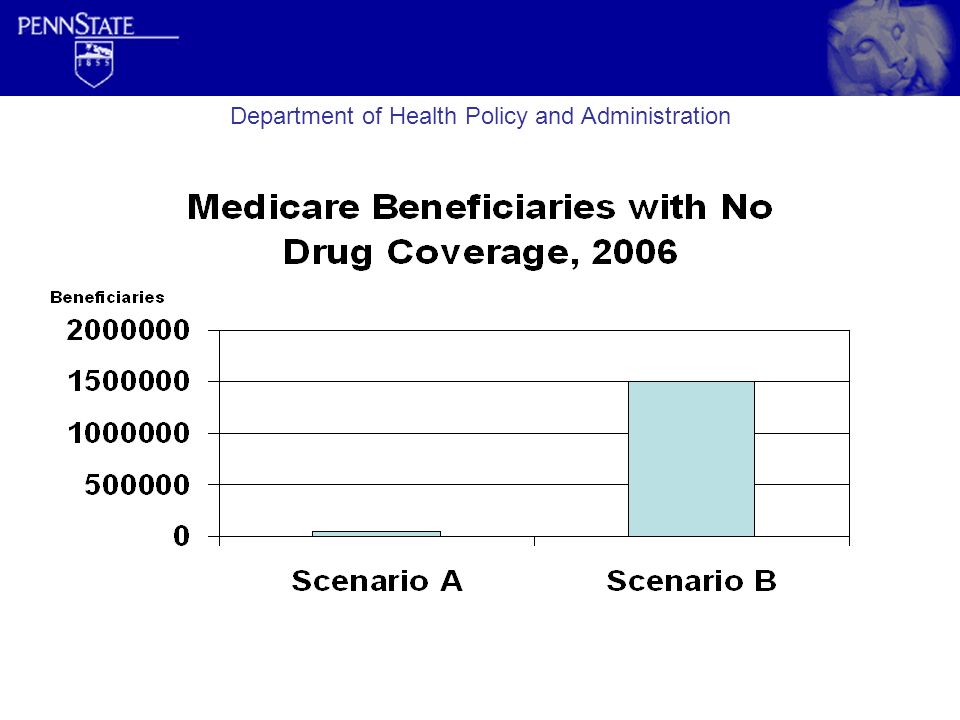
Implications for Part D Simulation of Part D under two scenarios –Scenario A assumes elasticity of drug coverage is -0.3 –Scenario B assumes elasticity of drug coverage is -0.93 Department of Health Policy and Administration

12
Gross program costs do not account for Medicaid clawbacks, employer subsidies, or other adjustments.

13
Department of Health Policy and Administration

15
Summary and Conclusions Our model, which appears to capture unmeasured health effects very well, suggests that moral hazard from prescription drug coverage is much higher than previous estimates Using our estimated elasticity suggests current Part D estimates significantly underpredict spending and overpredict enrollment in Medicare Part D Department of Health Policy and Administration

Similar presentations