Download presentation
Presentation is loading. Please wait.

1
Thyroid Disease PBL

2
Basic Anatomy Level C5 – T1 Surrounded by thin fibrous capsule
Highly vascular 15 – 30 g Norm

3
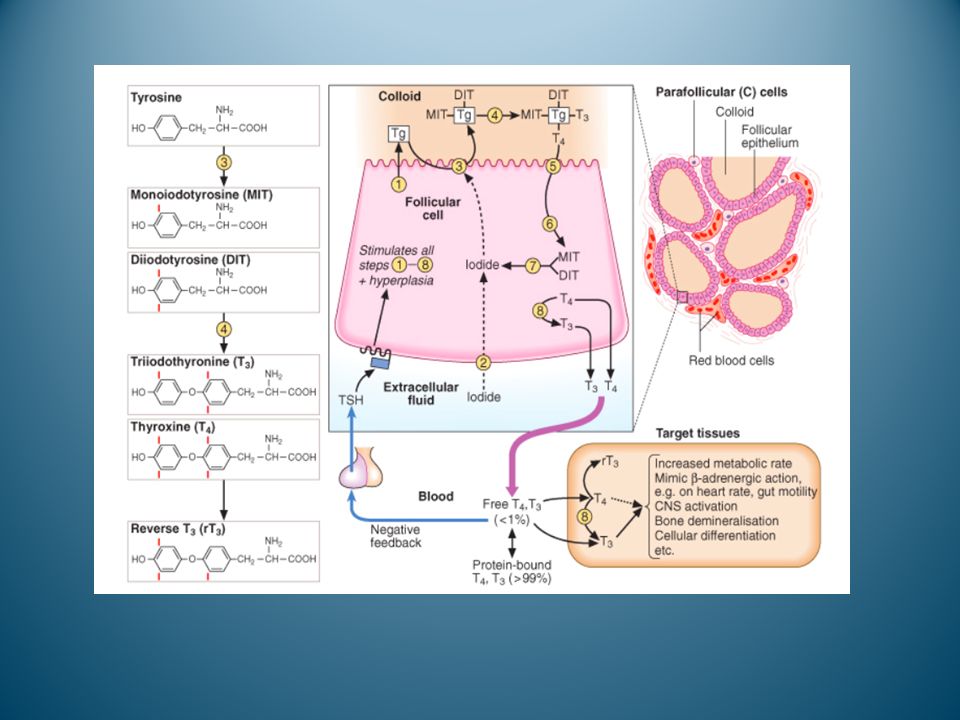
Basic Histology Has numerous spherical follicles – cuboidal epithelium (follicular cells) surrounding the secreted colloid in the centre.
 surrounding the secreted colloid in the centre.")
4
Further Histology Thyroid follicles lined by simple cuboidal epithelium. Size of follicles vary depending on activity of the gland – active = smaller follicles lined by tall cuboidal/columnar cells, less activy = larger follicles lined by flattened epithelial cells. Has C cells (parafolliclar cells) that are scattered around the basement membrane and characteristically have a clear cytoplasm (secrete calcitonin).
 that are scattered around the basement membrane and characteristically have a clear cytoplasm (secrete calcitonin).")
5
Thyroid Hormones Triiodothyronine (T3):
4X more potent than T4, but a smaller pool of it (7%). Most of it formed from iodine cleavage of T4 at peripheral tissues Less strongly protein bound. Half life – 1 to 2 days.
. Most of it formed from iodine cleavage of T4 at peripheral tissues. Less strongly protein bound. Half life – 1 to 2 days.")
6
Thyroid Hormones Thyroxine (T4): Function of T4 and T3:
Less potent but larger pool (93%) – acts as a reservoir pool as it has a longer half life. Half life – 7 days. Function of T4 and T3: Increase basal metabolic rate. Mimic B adrenergic action (heart, gut motility, CNS activation) (upregulates B adrenergic receptors).
 – acts as a reservoir pool as it has a longer half life. Half life – 7 days. Function of T4 and T3: Increase basal metabolic rate. Mimic B adrenergic action (heart, gut motility, CNS activation) (upregulates B adrenergic receptors).")
8
Thyrotoxicosis & Hyperthyroidism
Thyrotoxicosis: Clinical syndrome characterised by elevated serum levels of T3 and T4. It can also be elevated TSH from a pituitary tumour (this is rare). (Excessive thyroid hormone) Affects 2-5% of females at some point in their life. Sex ratio= 5-10 : 1 (F:M) Hyperthyroidism: Excessive thyroid function.
. (Excessive thyroid hormone) Affects 2-5% of females at some point in their life. Sex ratio= 5-10 : 1 (F:M) Hyperthyroidism: Excessive thyroid function.")
9
Graves Disease Most common form of hyperthyroidism.
Autoimmune process where serum IgG antibodies stimulate the TSH receptors (mimic TSH) to stimulate thyroid hormone production. Antibody known as Long Acting Thyriod Stimulator (LADS) Specific Graves disease Ix: Anti-thyroid Peroxidase (TPOAb) presence.
 to stimulate thyroid hormone production. Antibody known as Long Acting Thyriod Stimulator (LADS) Specific Graves disease Ix: Anti-thyroid Peroxidase (TPOAb) presence.")
10
Graves: cardinal signs and symptoms
Graves Eye disease: Lid retraction/lag +/- exophthalmos (due to immune response that causes retro-orbital inflammation). Pre-tibial myxoedema: Accumulation of mucopholysaccharides in the dermis of the skin. Clubbing. Thyroid often has bruit.
. Pre-tibial myxoedema: Accumulation of mucopholysaccharides in the dermis of the skin. Clubbing. Thyroid often has bruit.")
11
Other Sx of Hyperthyroidism
Weight loss but increased appetite. Mood disturbances, irritability, agitation Sympathetic overdrive: sweating, tachycardia, darrhoea, AF, hypertension, tremor, palpitations, warm vasodilated peripheries Menstrual changes Muscle weakness +/- Proximal myopathy

12
Other causes of Thyrotoxicosis
Toxic Adenoma: Soliary nodule producing T3 and T4. <1% of adenomas produce enough hormone to cause thyrotoxicosis. Toxic multi-nodular goitre Rarely 1-2 nodules may become hypersecretory. More common in the elderly and iodine deficient.

13
Other causes of Thyrotoxicosis
De Quervain’s thyroiditis ‘subacute thyroiditis’: Transient hyperthyroidism from an acute inflammatory process, probably viral. Usually also fever, malaise, pain in the neck Thyroid cancer Small cell carcinoma of the lung Secondary causes: drugs – amiodarone

14
Management Aim: reduce thyroid hormone over production and to block its peripheral effects Stages Use anti-thyroid medication to induce euthyroid state Surgery/Radioactive iodine/ to block and replace. Maintain euthyroid state and replace if necessary. Also: symptomatic relief by using B-blockers.

15
Anti-Thyroid Medication
Controls hyperthyroidism, but does not cure it. Often used to shrink thyroid gland before surgery. Include: Thyionamides Radioactive Iodine Iodine/Iodide treatment B-adrenoreceptor agonists

16
Thionamides Inhibits iodination of tyrosine on thyroglobulin, so decreases T3, T4. Carbimazole and propylthiouracil usually preferred (these also reduce breakdown of T4 to T3 in peripheral tissue). Can be taken orally, good for long term use in Graves. Crosses the placenta, can be found in breast milk, can cause hypthyroidism in babies (carbimazole chosen over propylthiouracil to minimise this). SE: rashes (2-25%), headache, nausea, jaundice, joint pains, agranulocytosis (dec WBC).
. Can be taken orally, good for long term use in Graves. Crosses the placenta, can be found in breast milk, can cause hypthyroidism in babies (carbimazole chosen over propylthiouracil to minimise this). SE: rashes (2-25%), headache, nausea, jaundice, joint pains, agranulocytosis (dec WBC).")
17
Radioactive Iodine Treatment
Used for hyperthyroidism and thyroid carcinoma. Given orally, radioactive iodine taken up by thyroid and incorporated into thyroglobin, where it has a localized cytotoxic effect, killing nearby cells. Single dose: cytotoxic effects seen in 1-2 months, peaks at 3-4 months. SE: hypothyroidism, small increased risk of thyroid cancer. C/I: pregnancy and childhood.

18
Iodine/Iodide treatment
Most rapid treatment. High dose of Iodine inhibits release of T3, T4 (via inhibition of TSH and TRH). Very useful for short term managment of hyperthyroidism: thyrotoxic crisis and preparation for thyroidectomy. Takes 24 hours for effect to be seen. Reduction in vascularity and gland size in days. Allergy reaction can occur.
. Very useful for short term managment of hyperthyroidism: thyrotoxic crisis and preparation for thyroidectomy. Takes 24 hours for effect to be seen. Reduction in vascularity and gland size in days. Allergy reaction can occur.")
19
B Adrenoreceptor Agonists
Symptomatic treatment Used when waiting for the effects of radioactive iodine and thionamides to be seen. Sx such as tachycardia, angina, arrhythmia, agitation.

20
Thyroidectomy Not usually used as medical treatment usually successful. Indications: Elective Persistent medication SE Large goitres that will not remit after medical management Poor compliance with drugs

21
Thyroidectomy - complications
Post op bleeding can cause tracheal compression and asphyxiation (but rare) Laryngeal nerve palsy (1%) Transient hypocalcaemia (10%) Hypothyroidism (10% of pt) Recurrent Hyperthyroidism Damage/ removal of parathyroid glands (1% permanent hypoparathyroidism)
 Laryngeal nerve palsy (1%) Transient hypocalcaemia (10%) Hypothyroidism (10% of pt) Recurrent Hyperthyroidism. Damage/ removal of parathyroid glands (1% permanent hypoparathyroidism)")
22
Goitre Goitre – an enlarged thyroid gland, can be diffuse or nodular.
Hypothyroidism (increase TSH): Dietary deficiency of iodine causes reduced levels of thyroid hormones, which leads to increased secretions of TSH from ant pituitary, causing thyroid gland to hypertrophy and cause goitre. Hyperthyroidism (hypertrophy): The follicules are overactive, causing them to hypertrophy (not hyperplasia)
: Dietary deficiency of iodine causes reduced levels of thyroid hormones, which leads to increased secretions of TSH from ant pituitary, causing thyroid gland to hypertrophy and cause goitre. Hyperthyroidism (hypertrophy): The follicules are overactive, causing them to hypertrophy (not hyperplasia)")
23
Tumours Benign Tumours of the thyroid usually benign
Follicular adenoma is the most common cause of a solitary thyroid nodule. Sometimes may be ‘hot’ on radio-isotope scans, and can cause thyrotoxicosis.

24
Tumour - malignant Thyroid cancer not common accounts for <1% of all cancer deaths. 90% present as thyroid nodules, occasionally with cervical LAD (5%), or with lung, hepatic, bone or cerebral mets. Very rarely cause hyperthyroidism, but 90% secrete thyroglobulin – good tumour marker.
, or with lung, hepatic, bone or cerebral mets. Very rarely cause hyperthyroidism, but 90% secrete thyroglobulin – good tumour marker.")
25
Malignant nodule Rx Surgery: total thyroidectomy indicated for any malignancy greater than 1 cm diameter. Remnant ablation: thyroid tissue remaining is destroyed with orally administered radioiodine. NB: this is where thyroglobulin is handy – after thyroidectomy and further radio iodine administratin, there should be no thyroid tissue, hence no thyroglobulin – if there is some, may be from secondary mets.

26
Prognosis Good 10 year survival: 80-95% Factors that worsen prognosis:
Male, poor differentiation, local invasion, distant mets, advanced age, large tumour.

27
Investigations Specific thyroid antibodies:
TPOAb (thyroid peroxidase antibody): Present in Hashimoto’s and Graves’ TgAb (thyroglobulin antibody): Present in Hashimoto’s and Thyroid cancer TRAb (thyroid stimulating hormone receptor antibody): Present in Graves’
: Present in Hashimoto’s and Graves’ TgAb (thyroglobulin antibody): Present in Hashimoto’s and Thyroid cancer. TRAb (thyroid stimulating hormone receptor antibody): Present in Graves’")
28
Further Ix U/S Useful for nodules – can see if they are cyctic or solid. Can help determine multi-nodular goitre when only a single nodule is palpable. Unfortunately, even cystic lesions can be malignant and tumours can arise in multi-nodular goitre, so FNA is usually also done. FNA: In pt with a solitary nodule or dominant nodule in multi-nodular goitre, there is a 5% risk of malignancy. 5% false negative rate – counsel pt.

29
Further Ix Chest and thoracic inlet x-rays
To detect tracheal compression and retrosternal extensions. Thyroid scan FNA largely replaced isotope scans in diagnosing thyroid nodules. Can be useful to distinguish between functioning (hot) and non-functioning (cold) nodules. Hot nodule rarely malignant. 10% of cold nodule malignant
 and non-functioning (cold) nodules. Hot nodule rarely malignant. 10% of cold nodule malignant.")
Similar presentations



,Triiodothyronine T3 (9%) and rT3 (1%). Reverse T3 (rT3) is biologically inactive.>")













 55 F Graves’ disease diagnosed at 彰基 one year ago Initial presentation: sweating, good appetite, easy nervousness Physical.>")

