Download presentation
Presentation is loading. Please wait.

1
Li, Kingbherly Lichauco, Rafael Lim, Imee Loren Lim, Jason Morven Lim, John Harold Lim, Mary Lim Phoebe Ruth Dr. Jerry Santos

2
Polycrystalline aggregates composed of varying amounts of crystalloid and organic matrix Stone formation requires supersaturated urine Urinary pH, ionic strength, solute concentration, complexation Urinary constituents change dramatically during different physiologic states

3
Greater concentration of 2 ions The more likely they are to precipitate Solubility product (K sp ) = as ion concentrations increase, their activity product reaches a specific point Formation product (K fp ) = concentration above K sp capable of initiating crystal growth and heterogeneous nucleation
 = as ion concentrations increase, their activity product reaches a specific point Formation product (K fp ) = concentration above K sp capable of initiating crystal growth and heterogeneous nucleation")
4
Urinary stones originate from crystals or foreign bodies immersed in supersaturated urine CRYSTAL INHIBITOR THEORY Calculi form owing to absence or low concentration of natural stone inhibitors – Magnesium, citrate, pyrophosphate, trace metals

5
Stones are primarily composed of crystalline component Crystal formation Nucleation, growth, aggregation

6
Theory of mass precipitation Distal tubules or collecting ducts becomes plugged with crystals, establishing an environment of stasis, for further stone growth Tubules enlarge as they entire papilla, transit time is only a few minutes Fixed particle theory Formed crystals retained within cells or beneath tubular epithelium

7
Noncrystalline matrix component 2-10% by weight Mainly protein with hexose and hexosamine Matrix Calculus assoc with previous kidney surgery or chronic UTI Gelatinous texture May serve as a nidus for crystal aggratation

8
Major ion present in urinary crystals 95% calcium filtered at glomerulus is reabsorbed at proximal and distal tubules <2% excreted in urine Diuretics – hypocalciuric effect, decrease calcium excretion Normal waste product of metabolism, relatively insoluble Enters large bowel, consumed by bacterial decomposition Excreted by proximal tubule Supersaturation of calcium oxalate Hyperoxaluria – bowel disorders Calcium Oxalate

9
Important buffer, complexes with calcium in urine Filtered cy glomerulus, reabsorbed in proximal tubules Parathyroid hormone inhibits reabsorption By-product of purine metabolism Any defect in purine metabolism = urinary stone disease Defect in xanthine oxidase Xanthine may ppt in urine PhosphateUric Acid

10
Important role in regulating crystallization of calcium salts in urine High dietary calcium – increases urinary calcium excretion Reduces ability of urine to inhibit calcium oxalate crystal agglomeration Pivotal role in citric acid cycle in renal cells Estrogen increases citrate excretion, factor that decreases incidence of stones in women Alkalosis increases citrate excretion SodiumCitrate

11
Lack of magnesium is associated with increased calcium oxalate stone formation Prevent urinary calculi Complex with calcium Magnesium Sulfate

13
Calcium Calculi Absorptive hypercalciuric nephrolithiasis Resorptive hypercalciuric nephrolithiasis Renal induced hypercalciuric nephrolithiasis Hyperuricosuric Ca nephrolithiasis Hyperoxaluric Ca nephrolithiasis Hypocitraturic Ca nephrolithiasis Non-Calcium Calculi Struvite or Magnesium Ammonium Phosphate Uric Acid Cystine Xanthine Indinavir Rare Silicate Triamterene

14
Calcifications accumulate in collecting system Nephrolithiasis (calcareous) – elevated urinary calcium – elevated urinary uric acid – elevated urinary oxalate – decreased level urinary citrate Symptoms secondary to obstruction: – Pain – Infection – Nausea – Vomiting Asymptomatic hematuria or UTI urinary stone
 – elevated urinary calcium – elevated urinary uric acid – elevated urinary oxalate – decreased level urinary citrate Symptoms secondary to obstruction: – Pain – Infection – Nausea – Vomiting Asymptomatic hematuria or UTI urinary stone")
15
Increased calcium absorption from jejunum Increased calcium filtered from the glomerulus Suppression of PTH Decreased tubular reabsorption of calcium Hypercalciuria

16
Most severe type Independent of diet Elevated urinary calcium level Tx: cellulose phosphate, hydrochlorothiazide Type I Dietary dependent, Most Common Tx: no specific returns to normal on calcium restricted diet Type II “Phosphate renal leak” Decreased serum phosphate increase 1,25 dihydroxyvitamin D synthesis Tx: orthophosphate (inhibit Vit. D synthesis) Type III
 Type III.")
17
typically found in hyperparathyroidism calcium is released from bone in response to the increased activity of osteoclasts caused by excessive and inappropriate serum PTH levels causes significant hypercalcemia PTH causes the kidney to limit calcium excretion, but, with the overwhelming serum calcium load produced with hyperparathyroidism, the kidneys are forced to excrete the extra calcium into the urine, causing the hypercalciuria.

18
Increased tubular defect in calcium excretion Decrease serum calcium Increase PTH level Increase level of calcium back to kidney, renal tubules excrete large amounts of calcium elevated fasting urinary calcium level, normal serum calcium level, elevated PTH level

19
Excessive purine Increased uric acid production Increased urinary monosodium urates Management: Diet modification DOC: allopurinol 300mg/day Potassium citrate

20
Tx: calcium supplementation Intraluminal calcium binds to fat SAPONIFICATION Malabsorption: increase intraluminal fat and bile Severe dehydration Increased oxalate levels

21
Tx: potassium citrate supplementation Decrease excretion of citrate Increased metabolic demands of mitochondria of renal cells Intracellular metabolic acidosis Hypokalemia Fasting Hypomagnesemia Androgens and gluconeogenesis UTI ACTIONS: Citrate complexes with calcium decreasing ionic calcium concentration decrease energy crystallization

23
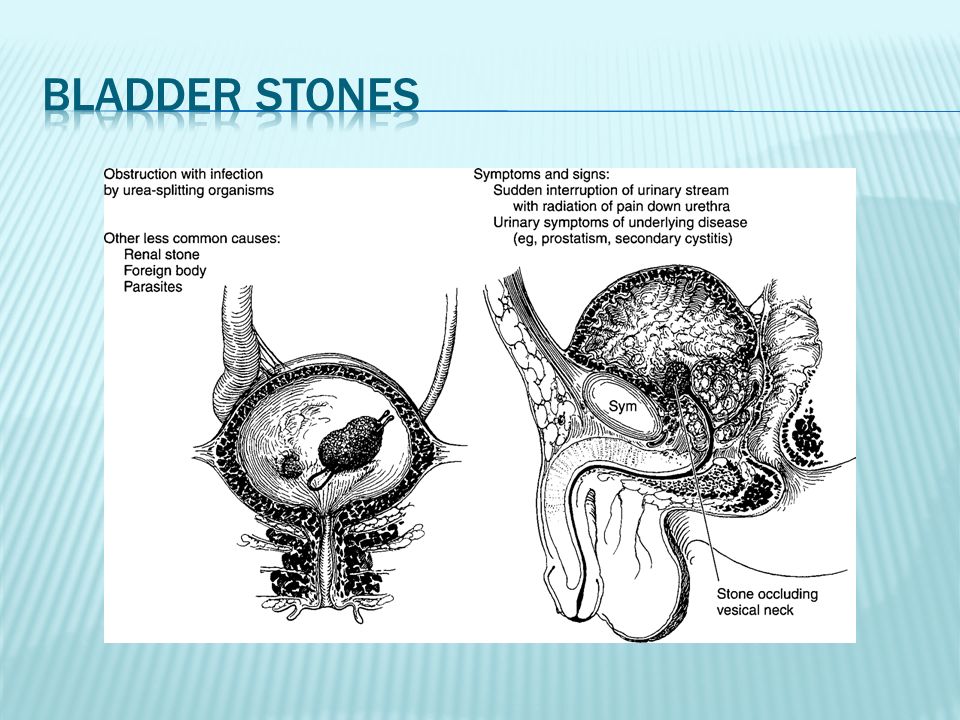
Composed of Magnesium, Ammonium, & Phosphate (MAP) Most common in women Frequently present as renal staghorn calculi Struvite stones are associated with urea- splitting organisms Proteus Pseudomonas Providencia Klebsiella Staphylococci Mycoplasma
 Most common in women Frequently present as renal staghorn calculi Struvite stones are associated with urea- splitting organisms Proteus Pseudomonas Providencia Klebsiella Staphylococci Mycoplasma")
24
Alkaline Urinary pH Results from the high ammonium concentration derived from the urea-splitting organisms pH >7.2 (NV: 5.85) MAP crystals precipitate MAP crystals are soluble in the normal urinary pH range (5-7) Foreign bodies and neurogenic bladders may predispose patients to urinary infections and subsequent struvite stone formation
 MAP crystals precipitate MAP crystals are soluble in the normal urinary pH range (5-7) Foreign bodies and neurogenic bladders may predispose patients to urinary infections and subsequent struvite stone formation")
25
Stone removal is therapeutic Long term management Optimized with removal of foreign bodies All stone fragments should be removed with or w/o the aid of follow-up irrigations Acetohydroxemic acid Inhibits the action of bacterial urease, thereby reducing the urinary pH and decreasing the likelihood of precipitations

26
<5% of all urinary calculi Usually found in men High incidence of Uric Acid Lithiasis Gout Myeloproliferative disease Rapid weight loss Those treated for malignant conditions with cytotoxic drugs

27
Treatment Centered on: Maintaining a urine volume of >2L / dayand a urinary pH of 6 Reducing dietary purines or the administration of allopurinol helps reduce uric acid excretion Alkalinization with oral sodium bicarbonate, potassium citrate, or IV 1/6 normal sodium lactate May dissolve calculi and is dependent on the stone surface area

28
Secondary to an inborn error of metabolism resulting in abnormal intestinal mucosal absorption and renal tubular absorption of dibasic amino acids Cystine Ornithine Lysine Arginine

29
Genetic defects of cystinuria has been mapped to chromosome 2p.16 and 19q13.1 Cystine lithiasis Only clinical manifestation of this defect 1-2% of all urinary stones Suspected in patients with a (+) FH of urinary stones and the radiographic appearance of a faintly opaque, ground-glass, smooth-edged stone Urinalysis: hexagonal crystals
 FH of urinary stones and the radiographic appearance of a faintly opaque, ground-glass, smooth-edged stone Urinalysis: hexagonal crystals")
30
Medical Therapy ◦ High fluid intake (>3L/day) ◦ Urinary alkalinization ◦ Penicillamine Reduce urinary cystine levels Poorly tolerated by some patients (skin rashes, loss of taste, nausea, vomiting, & anorexia) ◦ Mercaptopropionylglycine Forms soluble complex with cystine and can reduce stone formation Surgical ◦ Most stones are recalcitrant to ESWL
 ◦ Urinary alkalinization ◦ Penicillamine Reduce urinary cystine levels Poorly tolerated by some patients (skin rashes, loss of taste, nausea, vomiting, & anorexia) ◦ Mercaptopropionylglycine Forms soluble complex with cystine and can reduce stone formation Surgical ◦ Most stones are recalcitrant to ESWL")
31
Secondary to a congenital deficiency of xanthine oxidase Catalyzes the oxidation of hypoxanthine to xanthine and of xanthine to uric acid Urinary stones develop on 25% of patients with xanthine oxidase deficiency Stones are radiolucent and are tannish yellow in color

32
Treatment Directed by symptoms and evidence of renal obstruction High fluid intake Urinary Alkalinization Stone recurrence Trial of Allopurinol Purine-restricted diet

33
Protease inhibitors are a popular and effective treatment in patients with AIDS Indinavir ◦ 6% of patients prescribed had radiolucent stones ◦ Indinavir calculi > only urinary stones to be radiolucent on non-contrast CT scans Associated with calcium components Stones are tannish red Temporary cessation of the medication with intravenous hydration frequently allows thes stones to pass

34
Silicate Associated with long term use of antacids containing silica Surgical treatment Triamterene Associated with anti-hypertensive medications containing triamterene (Dyazide) Discontinuing the medication eliminates stone recurrence Glafenine Antrafenine
 Discontinuing the medication eliminates stone recurrence Glafenine Antrafenine")
36
Colicky Noncolicky Usually acute in onset, relatively constant, unexpected and severe Urinary obstruction due to a direct increase in intraluminal pressure stretching nerve endings inflammation, edema, hyperperistalsis, and mucosal irritation

37
Affected by: Stone size Location Degree of obstruction Variation of individual anatomy Patients frequently move constantly into unusual positions in contrast to the lack of movement of someone with peritoneal signs

38
1. Renal calyx— deep, dull ache in the flank or back Mild to severe Frequently small may be exacerbated after consumption of large amounts of fluid the presence of infection or inflammation in the calyx or diverticulum may contribute to pain perception. occasionally result in spontaneous perforation with urinoma, fistula, or abscess formation

39
2. Renal pelvis >1 cm in diameter - obstruct the ureteropelvic junction causing severe pain in the costovertebral angle, just lateral to the sacrospinalis muscle and just below the 12th rib dull to excruciatingly sharp, constant, boring Radiates along the course of the ureter and into the testicle

40
Partial or complete staghorn calculi- are not necessarily obstructive, few symptoms, “silent” can often lead to significant morbidity, including renal deterioration, infectious complications, or both

41
3. Upper and midureter severe, sharp back (costovertebral angle) or flank pain progressing down the ureter – more severe and intermittent lodged at a particular site - less pain, especially if it is only partially obstructive Upper ureteral - lumbar region and flank
 or flank pain progressing down the ureter – more severe and intermittent lodged at a particular site - less pain, especially if it is only partially obstructive Upper ureteral - lumbar region and flank.")
42
Midureteral - radiates caudally and anteriorly toward the mid and lower abdomen in a curved, band-like fashion (initially parallels the lower costal margin but deviates caudal toward the bony pelvis and inguinal ligament)
")
43
4. Distal ureter pain that radiates to the groin or testicle in males and the labia majora in females (ilioinguinal or genital branch of the genitofemoral nerves) This pain pattern is likely due to the similar innervation of the intramural ureter and bladder Bladder – urgency and frequency with burning (inflammation of the bladder wall around the ureteral orifice)
 This pain pattern is likely due to the similar innervation of the intramural ureter and bladder Bladder – urgency and frequency with burning (inflammation of the bladder wall around the ureteral orifice).")
44
complete urinalysis : hematuria and crystalluria and documenting urinary pH intermittent gross hematuria or occasional tea- colored urine (old blood) Rarely (in 10–15% of cases), complete ureteral obstruction presents without microhematuria.
 Rarely (in 10–15% of cases), complete ureteral obstruction presents without microhematuria.")
45
Magnesium ammonium phosphate (struvite) stones = infection stones Proteus, Pseudomonas, Providencia, Klebsiella, and Staphylococcus infections Calcium phosphate stones urine pH <6.6 - brushite stones urinary pH >6.6 - infectious apatite stones All stones, however, may be associated with infections secondary to obstruction and stasis proximal to the offending calculus. Infection pain Uropathogenic bacterial exotoxins and endotoxins may alter ureteral peristalsis Local inflammation chemoreceptor activation and perception of local pain

46
1. Pyonephrosis—gross pus in an obstructed collecting system extreme form of infected hydronephrosis Presentation: may range from asymptomatic bacteriuria to florid urosepsis Renal urine aspiration - definitive diagnosis untreated renocutaneous fistula

48
Differential Diagnosis mimic other retroperitoneal and peritoneal pathologic states Peritoneal signs should be sought during physical examination History onset, character, potential radiation, activities that exacerbate or ease the pain, associated nausea and vomiting or gross hematuria, and a history of similar pain

49
1. Crystalluria The rate of stone formation is proportional to the percentage of large crystals and crystal aggregates. Crystal production is determined by the saturation of each salt and the urinary concentration of inhibitors and promoters. Urine samples – fresh, centrifuged and examined immediately

50
2. Socioeconomic factors affluent, industrialized countries 3. Diet less energy-dense diet may decrease the incidence of stones Vegetarians may have a decreased incidence of urinary stones. High sodium intake is associated with increased urinary sodium, calcium, and pH, and a decreased excretion of citrate; Fluid intake and urine output

51
4. Occupation Physicians and other white- collar workers have an increased incidence of stones compared with manual laborers. may be related to differences in diet and physical activity; high temperatures may develop higher concentrations of solutes 5. Climate —hot climates are prone to dehydration Increased calcium and oxalate excretion has been correlated with increased exposure time to sunlight

52
6. Family history Those with a family history of stones have an increased incidence of multiple and early recurrences 7. Medications antihypertensive medication triamterene Long-term use of antacids containing silica Carbonic anhydrase inhibitors Protease inhibitors in immunocompromised patients are associated with radiolucent calculi.

53
acute renal colic Systemic components: tachycardia, sweating, and nausea Costovertebral angle tenderness abdominal mass may be palpable in patients with long- standing obstructive urinary calculi and severe hydronephrosis Fever, hypotension, and cutaneous vasodilation: urosepsis thorough abdominal examination should exclude other causes of abdominal pain

54
Computed tomography imaging modality of choice in patients presenting with acute renal colic rapid and is less expensive than IVP It images other peritoneal and retroperitoneal structures and helps when the diagnosis is uncertain There is no need for intravenous contrast. do not give anatomic details as seen on an IVP Uric acid stones are visualized no differently from calcium oxalate stones. Matrix calculi have adequate amounts of calcium to be visualized easily by CT.

55
Intravenous Pyelogram IV injection of contrast to visualize renal collecting systems, ureters and UB gives a comprehensive view of the patient's anatomy 50 ml of a special dye is injected into the bloodstream that is excreted by the kidneys and by its density helps outline any stone on a repeated X- ray X ray images every few minutes to determine if there is any obstruction to the dye as it is excreted into the bladder

56
Tomography useful to identify calculi in the kidney when oblique views are not helpful. visualizes the kidney in a coronal plane identify poorly opacified calculi, especially when interfering abdominal gas or morbid obesity make KUB films suboptimal

57
KUB films and directed ultrasonography Plain frontal supine radiograph of the abdomen Visualization of: Renal shadows Psoas muscle shadow Calcification (stones, vascular, lymph node or tumor UB shadow Calcium radiopaque

58
About 10% of stones do not have enough calcium to be seen on standard X-rays (radiolucent stones) The distal ureter is easily visualized through the acoustic window of a full bladder. Edema and small calculi missed on an IVP can be appreciated with such studies.

59
Ultrasound presence of hydronephrosis (swelling of the kidney—suggesting the stone is blocking the outflow of urine) detect stones during pregnancy when x-rays or CT are discouraged
 detect stones during pregnancy when x-rays or CT are discouraged")
60
Retrograde pyelography required to delineate upper-tract anatomy and localize small or radiolucent offending calculi. Visualization of urinary collecting system achieved via cystoscope, ureteral catherization and retrograde injection of contrast Used when IVU failed to opcacify renal collecting system and ureters

61
Nuclear scintigraphy radioisotopes (here called radiopharmaceuticals) are taken internally, and the emitted radiation is captured by external detectors (gamma cameras) to form two-dimensional images Bisphosphonate markers can identify even small calculi that are difficult to appreciate on a conventional KUB film
 are taken internally, and the emitted radiation is captured by external detectors (gamma cameras) to form two-dimensional images Bisphosphonate markers can identify even small calculi that are difficult to appreciate on a conventional KUB film")
63
Conservative observation Dissolution agents Relief of Obstruction Extracorporeal Shockwave Lithotripsy (ESWL) Ureteroscopic stone extraction Percutaneous Nephrolithotomy Open stone surgery Pyelolithotomy Anatrophic Nephrolithotomy Radial Nephrotomy Ureterolithotomy others
 Ureteroscopic stone extraction Percutaneous Nephrolithotomy Open stone surgery Pyelolithotomy Anatrophic Nephrolithotomy Radial Nephrotomy Ureterolithotomy others")
64
Conservative management Majority of stones pass out within a 6 week period after the onset of symptoms depends on the size of the calculi and its location Dissolution agents Use alkalinizing agents Given oral, IV or intrarenal Relief of the Obstruction Emergent drainage in patient with signs of UTI

65
Extracorporeal Shockwave Lithotripsy (ESWL)
")
67
excessive weight (>300 lb) may severely limit or preclude ESWL. Pregnant women and patients with large abdominal aortic aneurysms or uncorrectable bleeding disorders should not be treated with ESWL. Individuals with cardiac pacemakers should be thoroughly evaluated by a cardiologist.

68
Highly effective for lower ureteral calculi Stone may be extracted using a wire basket Or lithotrites may be placed through the ureteroscope to fragment the calculi

69
the treatment of choice for large (>2.5 cm) calculi; renal and proximal ureteral calculi, those resistant to ESWL, select lower pole calyceal stones with a narrow, long infundibulum and an acute infundibulo- pelvic angle, and instances with evidence of obstruction Rapid cure
 calculi; renal and proximal ureteral calculi, those resistant to ESWL, select lower pole calyceal stones with a narrow, long infundibulum and an acute infundibulo- pelvic angle, and instances with evidence of obstruction Rapid cure")
71
Classic way to remove calculi Mandatory to obtain a radiograph before the incision is made Not frequently used anymore because of the morbidity of the incision, the possibility of retained stone fragments, and the ease and success of less invasive techniques

72
Effective especially with extrarenal pelvis Transverse pyelotomy - effective and does not require interruption of the renal arterial blood supply Flexible endoscope – ensures stone- free status Coagulum – can retrieve multiple, small renal pelvic calculi and difficult- to-access caliceal calculi Cryoprecipitate Injected into the renal pelvis, endogenous clotting factors result in a Jelly-like coagulum of the collecting system. Small stones are entrapped and removed with the coagu- lum.

73
Used with complex staghorn calculi Complete staghorn calculus Partial staghorn calculus 1. Incision made on the convex surface of the kidney posterior to the line of Brodel 2. Occlusion of the renal artery followed by renal cooling with slushed ice 3. Nerve hook is helpful to tease out calculi 4. Repair of narrowed infundibula helps reduce stone recurrence rates.

75
Allows access to limited calyces of the collecting system Frequently used in blown-out calyces with thin overlying parenchyma Intraoperative ultrasound to localize the calyx and the calculi A shallow incision of the renal capsule can be followed by puncture into the collecting system. Stones may be cut with heavy Mayo scissors, and remaining fragments can be retrieved.

76
Partial nephrectomy – for large stones in a renal pole with marked parenchymal thinnin g Caution should be taken even with a normal contralateral kidney as stones are frequently associated with a systemic metabolic defect that may recur in the contralateral kidney Ileal ureter substitution – to decrease pain with frequent stone passage Autotransplantation with pyelocystostomy – for patients with rare malignant stone disease

77
Partial nephrectomy Ileal ureter substitution

78
Long standing ureteral calculi 1. Preoperative radiograph to document stone location 2. Incision lateral to the sacrospinalis muscles to allow medial retraction of the quadratus lumborum; anterior fascicle of the dorsal lumbar fascia must be incised to gain proper exposure 3. Vessel loop or Babcock clamp placed proximal to the stone to prevent frustrating stone migration 4. Longitudinal incision over the stone with a hooked blade to expose the calculus 5. Nerve hook to tease out the stone

80
About 1.6 L/24 h Encouraged during mealtime Increased approximately 2 h after meals Encouraged to force a nighttime diuresis

81
Stone analysis Outpatient urine collection during typical activities & fluid intake Ca stone formers Initial 24-h urine collection Include tests for Ca, uric acid, oxalate, citrate, Na, volume, & pH Hypercalciuria: most common abnormality

82
Alkalinizing pH agents Potassium citrate: oral agent that elevates urinary pH effectively by 0.7–0.8 pH units Adverse effect: abdominal discomfort Indications: Ca oxalate calculi 2° to hypocitraturia (<320 mg/day), including those with renal tubular acidosis; uric acid lithiasis & nonsevere forms of hyperuricosuric Ca nephrolithiasis. Alternative alkalinizing agents: Na, potassium bicarbonate, orange juice, & lemonade No effective long-term urinary acidifying agents

83
Gastrointestinal absorption inhibitor Cellulose phosphate binds Ca in the gut & inhibits Ca absorption & urinary excretion Decreases urinary saturation of Ca phosphate & Ca oxalate Phosphate supplementation Indicated for renal PO 4 leak

84
Diuretics Thiazides can correct renal Ca leak associated with renal hypercalciuria Prevents 2° hyperparathyroid state & its associated elevated vitamin D synthesis & intestinal calcium absorption Hypokalemia hypocitraturia

85
Calcium supplementation Indication: Enteric hyperoxaluric Ca nephrolithiasis Ca gluconate & Ca citrate Uric acid-lowering medications Allopurinol Urease inhibitor Acetohydroxamic acid: effective adjunctive treatment in chronic urea-splitting urinary tract infections associated with struvite stones Prophylaxis after removal of struvite stone

86
Prevention of cystine calculi Penicillamine: reduces the amount of urinary cystine that is relatively insoluble Mercaptopropionylglycine (Thiola)
")
88
Manifestation of an underlying pathologic condition, including voiding dysfunction or a foreign body Most seen in men Developing countries: frequently found in prepubescent boys Stone analysis: ammonium urate, uric acid, or Ca oxalate stones Irritative voiding symptoms, intermittent urinary stream, UTI, hematuria, or pelvic pain

89
Prostatic calculi: found within prostate gland per se & are found uncommonly within the prostatic urethra Represent calcified corpora amylacea & rarely found in boys Usually of no clinical significance, rarely they are associated with chronic prostatitis Large prostatic calculi: may be misinterpreted as a carcinoma Dx: radiograph or transrectal ultrasound

90
Smooth & hard Associated with hematospermia PE: stony hard gland; multiple stones present with crunching sensation Confused with tuberculosis of the seminal vesicle

91
Originate from bladder Develop 2° to urinary stasis, urethral diverticulum, near urethral strictures, or at sites of previous surgery Females: rarely develop urethral calculi due to short urethra & lower incidence of bladder calculi; associated with urethral diverticula Symptoms : intermittent urinary stream, terminal hematuria, & infection Dx: palpation, endoscopic visualization, or radiographic study

92
Occur in adults Develop 2° to a severe obstructive phimosis or poor hygiene with inspissated smegma Dx confirmed by palpation Tx: dorsal prepucial slit or formal circumcision

Similar presentations











 Calcium phosphate stones (2) Magnesium ammonium phosphate stones (3)Calcium oxalate stones >")



 is well- documented common occurrences in the general population nephrolithiasis (kidney calculi.>")




 Triple phosphate237 (26.4%) Phosphate119 (13.4%) Uric.>")





>")

