Download presentation
Presentation is loading. Please wait.

1
All about the IVP April 1 2004 Andrea Wilson

2
Case from U of Hawaii website 16 year old female Severe right flank pain with vomiting. No fever, urgency, or dysuria. PMH: unremarkable VS: T 36.8 P53, RR 24, BP 120/80. Abdomen: Diffuse tenderness, guarding and rebound on the right. Severe R CVA tenderness. UA: >100 RBCs, 20-50 WBCs, positive nitrite. N CBC and Cr

4
5 minutes after contrast

5
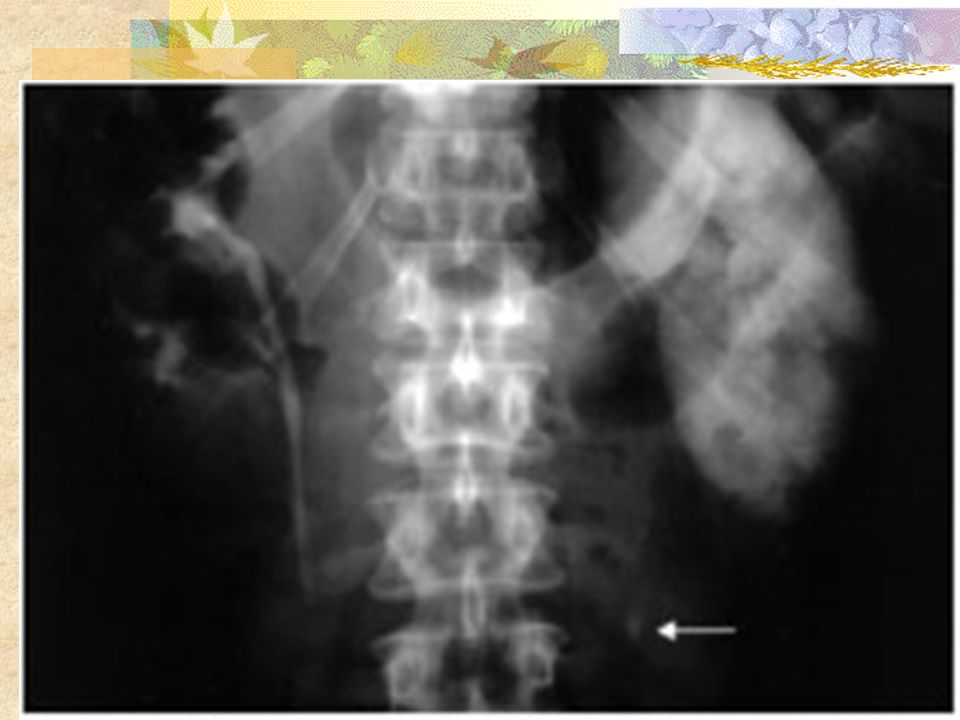
20 minute film

6
5 min film: L shows normal excretion, R ureter not well visualized and calyceal blunting (suggesting obstruction) 20 min film: R- more blunted calyces, hydronephrosis, delayed retention of contrast. There is a narrowing of the ureter on the right in the area of the suspected stone.

7
Procedure Flat plate X-rays are taken immediately before contrast administration and at 5, 10 and 20 minutes etc. Times usually doubled until contrast material fills both ureters

9
Advantages Clear outline of the entire urinary system so can see even mild hydronephrosis. Easier to pick out obstructing stone when there are multiple pelvic calcifications. Can show non-opaque stones as filling defects. Demonstrate renal function and allow for verification that the opposite kidney is functioning normally.

10
Disadvantages need for IV contrast material may provoke an allergic response multiple delayed films (Can take hours bc contrast passes quite slowly into the blocked renal unit and ureter.) May not have sufficient opacification to define the anatomy and point of obstruction. Requires a significant amount of radiation exposure and may not be ideal for young children or pregnant women

11
Intravenous contrast Usually 1.0 cc/kg Contrast allergy and nephrotoxicity (esp if renal insufficiency +/or D.M.) Get a creatinine first Greater incidence of adverse reactions with less expensive ionic dye than with the nonionic. If on metformin, then discontinue med for 2 days post-IVP

12
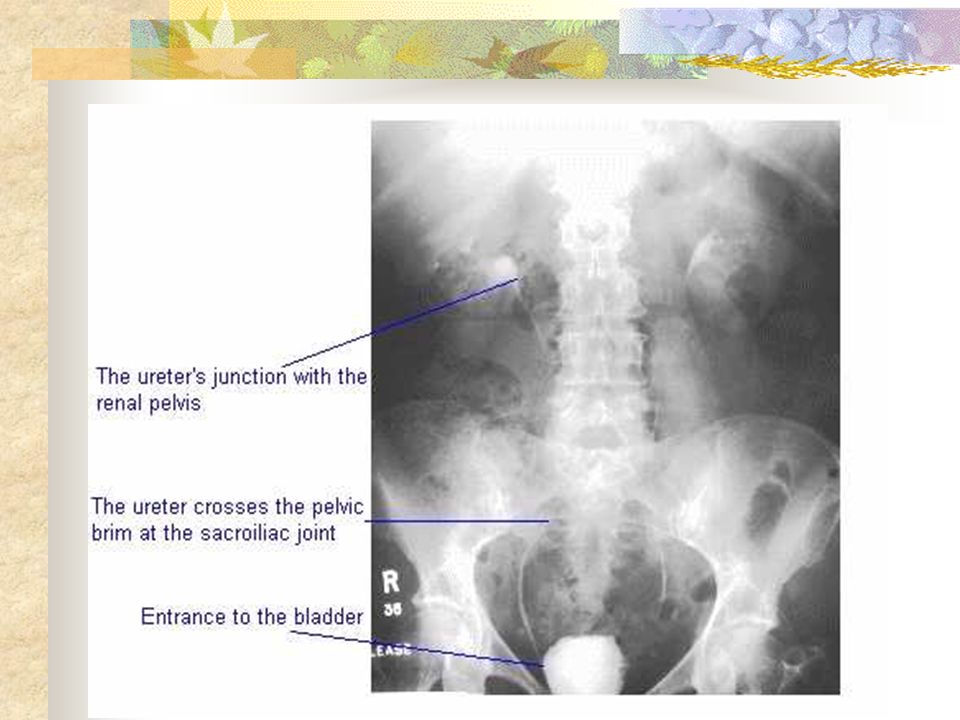
What to look for Scout film : look at kidney and bladder contours, kidney stones, ureteric stone Contrast films: compare sides, nephrogram: absent/delayed/hyperdense (absent= no kidney/non-functioning) Collecting system and ureter: dilatation, non-calcified stone or tumor (black filling defect) Extravasation ?Is the calcification in the ureter or not?
 Collecting system and ureter: dilatation, non-calcified stone or tumor (black filling defect) Extravasation Is the calcification in the ureter or not")
13
Ureteral stone Delayed nephrogram effect Columnization: ureter is peristaltic so shouldn’t see entire ureter unless there’s a stone. Radiopaque = calcium oxalate, cystine, calcium phosphate, magnesium-ammonium- phosphate Radiolucent = uric acid, blood clots, sloughed papillae

16
From Rosen’s 90% of stones <5 mm will pass. 15 % of stones 5-8 mm >8 mm usually lithotripsy or surgical removal

20
15 min film

21
Radiology Cases in Pediatric Emergency Medicine Loren G. Yamamoto, MD, MPH University of Hawaii John A. Burns School of Medicine 14 yo female Severe stabbing pain in her lower back x 2h No fever/chills, +urgency, no dysuria Also some abd pain + menstrual cramps for x 2 days. +nausea and emesis x2 Pain slightly improved with tylenol. LMP 4 wks ago. States not pregnant Another case

22
T36.7, P89, R 20, BP 90/60, 99%. Abd soft and non-tender. Normal bowel sounds. No rebound R>L side lumbar tenderness. Urine dip positive for blood. Preg test -

25
Case continued Normal CBC, lytes, BUN, Cr U/S done but non-diagnositic except for mild hydronephrosis of R kidney. IVP ordered. 20 minute and delayed films shown

26
20 min film

27
Delayed IVP

28
Case continued IVP demonstrates an obstruction in the right ureter, along with a clinical presentation consistent with ureteral colic. Ureteral stone likely…but very large density and location of the calcified density is not exactly in the expected path of the ureter. Now complaining of moderate abd pain with fluctuating nausea

29
Case continued Urologist and surgeon consulted. CT ordered but radiologist reluctant re second dose of contrast. Eventually passes tiny stone. Appendectomy- has appendicolith. Initial CT would have worked better in this case.

30
References Ames CD, Older RA. Imaging in Urinary Tract Obstruction. Departments of Urology and Radiology, University of Virginia Health System, Charlottesville, Virginia, USA www.brazjurol.com.br/julho_2001/ Ames_316_325.htmwww.brazjurol.com.br/julho_2001/ Ames_316_325.htm http://137.222.110.150/calnet/renal1/image Leslie SW. The Diagnostic Evaluation of Renal Colic in the Emergency Department http://www.emedhome.com/features_archive- detail.cfm?SFID=040300&SFTID=news Ouellette H, Tetreault P. Clinical Radiology made ridiculously simple. 2000. Pp37-41 Rosen, Barkin. Emergency Medicine: Concepts and Clinical Practice. 4 th Ed. Vol 3. pp 2252-2256 Yamamoto LG Kidani DCH. Urolithiasis: Radiology Cases in Pediatric Emergency Medicine Volume 7, Case 5 Kapiolani Medical Center For Women And Children. University of Hawaii John A. Burns School of Medicine www.hawaii.edu/.../pediatrics/ pemxray/v7c05.htmlwww.hawaii.edu/.../pediatrics/ pemxray/v7c05.html www.stmichaelshospital.com/.../ image2d.jpg www.urologyassociates.com/ urolith.jpg www.emedicine.com - Intravenous pyelogram www.emedicine.com

Similar presentations











 Calcium phosphate stones (2) Magnesium ammonium phosphate stones (3)Calcium oxalate stones >")





>")


 By Dr. Khalid Shakeel Babar (KSB)>")





