Download presentation
Presentation is loading. Please wait.

1
WHO bi-regional Health Care Financing Strategies for Countries of the Western Pacific and South-East Asia Regions ( ) and updated HCF strategy for Phusit Prakongsai Kanjana Tisayatikom International Health Policy Program (IHPP) Presentation to the IHPP Journal Club IHPP meeting room 4 June 2009
 Presentation to the IHPP Journal Club. IHPP meeting room. 4 June")
2
Outline of presentation
Background of health care financing in two WHO regions Strategy for health care financing ( ) Updating HCF strategies ( ) Proposed strategy indicators for monitoring and evaluation
 Updating HCF strategies ( ) Proposed strategy indicators for monitoring and evaluation.")
3
Background Health care financing is a key factor to determine access to and availability of health care, and the level of protection against catastrophic costs of illness. Appropriate health care financing arrangements help governments mobilize adequate financial resources for health, allocate them rationally, and use them equitably and effectively. Supporting adequate, sustainable, equitable and effective health financing to improve health outcomes is one of the most important goals of WHO.

4
Definition, Scope and Functions of healthcare financing
Direct payment Source of finance 1. Revenue Collection 2. Pooling 3. Purchasing Health Impact Health Services A process of funding health care system

5
Correlation of HH with catastrophic health expenditure and out-of-pocket payments
Source: Ke Xu, David B Evans, et al (2003)
")
6
Poverty headcount (at $1) increase by OOP share
 increase by OOP share")
7
Catastrophic spending: headcounts of households with OOP payments exceeding a threshold as share of total hh spending (Van Doorslaer, O’Donnell et al, HE, 2007)
")
8
The Regional Strategy on HCF 2006-2010 was endorsed by the RC for WP and SEA in 2005.
WHO carried out a mid-term review of the implementation of the strategy from July to September 2008. The draft mid-term review and updating of the HCF strategy for was discussed during a technical consultation of HCF experts in Manila, March 09.

10
Strategy for health care financing (2006-2010)
Increasing investment and public spending on health Achieving universal coverage and strengthening social safety nets Developing prepayment schemes, including social health insurance Supporting the national and international health and development process Strengthening regulatory frameworks and functional interventions Improving evidence for health financing policy development and implementation Monitoring and evaluation

11
The relationships between strategy areas, health system strengthening objectives, the achievement of universal coverage, and improved population health outcomes

12
Updated HCF Strategy for 2010-2015
Increase investment and public spending on health Improve aid effectiveness Improve efficiency by rationalizing health expenditures Increase pre-payment and pooling Improve provider payment methods Strengthen safety-net mechanisms for the poor and vulnerable Improve evidence and information for policymaking Improve monitoring and evaluation of policy changes

13
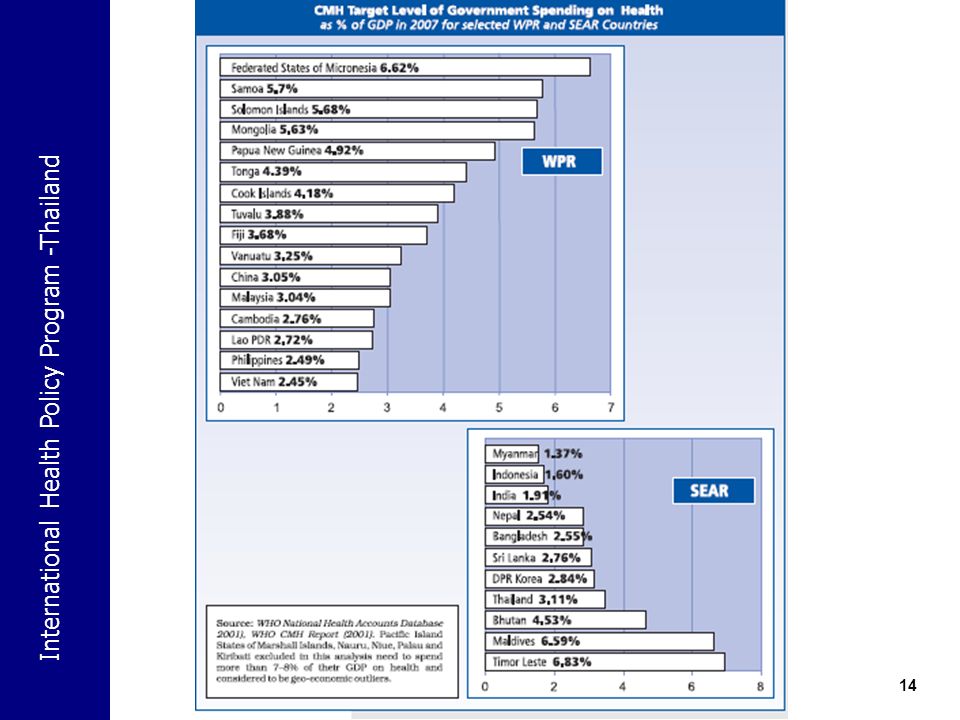
Strategy 1 – Increasing investment and public spending on health
Key challenges Lack of comprehensive national policy on HCF Inadequate and disproportionate funding Low level of health spending Poor assessment of available resources Inefficient and ineffective use of limited budgetary resources.

15
Strategy 1 – Increasing investment and public spending on health
Enhance government commitment and vision and set policy targets and medium and long-term action plans to reach universal coverage and access to quality health services. Produce policy briefs to stimulate dialogues on increasing fiscal space, health investment and government spending on health. Strengthen national capacity for resource mobilization to support national plans and defined health service packages for UC. Provide national and international experience and evidence to policy-makers for increasing investment and government budget and health spending, especially during the economic and financial crisis.

16
Strategy 1 – Increasing investment and public spending on health
Increase overall awareness about economic, social and health gains of public spending and investment especially among political leaders and high level government officials Intensify resource mobilization efforts through international partnerships to protect and secure adequate financial resources for implementation of national health plans for health and social safety nets, especially to maintain poverty reduction goals. Carry out analyses of health service needs for universal coverage compared to current provision, including the quality of services and financing practices, to identify gaps in priority health services with largest potential health impacts. Develop a health workforce development plan with appropriate funding levels and identified funding sources.

17
Strategy 2 – Improve aid effectiveness (1)
Revise national targets, plans, priorities, actions and resource requirements with a clear result focus that will constitute the basis for external aid and support. Carry out need assessments to identify systemic constraints and implementation bottlenecks for the delivery of essential services and the required process to address them. Plan capacity development linked to policy and institutional needs including assessing complementarities with other sectors, and analyzing roles of non-state partners (NGOs, civil society, and private sector). Ensure that the activities and program donor support are fully aligned with government programs and plans.
. Ensure that the activities and program donor support are fully aligned with government programs and plans.")
18
Strategy 2 – Improve aid effectiveness (2)
Reduce fragmentation by improving coordination, harmonization and integration of domestic and external resources to attain nationally defined health policy goals and objectives. Ensure consistency between health development plans, sector-wide approaches, and the overall budget, considering other sectors and macro-economic framework. Increase the proportion of aid that can be programmed by the ministry of health, and general budget support. Work with all partners to increase the duration of commitments and reduce volatility.

19
Strategy 3 – Improve efficiency by rationalizing health expenditures (1)
Improve health sector administration and management skills and practices at all levels of the health systems. Improve national planning processes, by using Medium Term Expenditure Framework (MTEF) and other tools to develop financial plans to attain universal coverage base on available and projected government and external financing resources. Undertake public health expenditure reviews (PER) and result-based budgeting where feasible to attain greater efficiency from public spending. Improve budgeting and financial planning practices to efficient and equitable allocation of resources to fund essential health service package accessible to all population.
 and other tools to develop financial plans to attain universal coverage base on available and projected government and external financing resources. Undertake public health expenditure reviews (PER) and result-based budgeting where feasible to attain greater efficiency from public spending. Improve budgeting and financial planning practices to efficient and equitable allocation of resources to fund essential health service package accessible to all population.")
20
Strategy 3 – Improve efficiency by rationalizing health expenditures (2)
Establish budget disbursement monitoring to assure that primary health care facilities in rural and underserved areas receive sufficient budgets on regular and timely basis. Review tertiary hospital expenditures including all levels of public health facilities to find possible areas of cost savings. Explore options to minimize costs of pharmaceutical supply and distribution including improving prescribing practice and eliminating financial incentives for over-prescription. Strengthen regulation of the private sector and enable the private sector to participate in delivering primary health care. Explore innovative approaches to support rational use of drugs and medical technologies.

21
Strategy 3 – Improve efficiency by rationalizing health expenditures (2)
Establish budget disbursement monitoring to assure that primary health care facilities in rural and underserved areas receive sufficient budgets on regular and timely basis. Review tertiary hospital expenditures including all levels of public health facilities to find possible areas of cost savings. Explore options to minimize costs of pharmaceutical supply and distribution including improving prescribing practice and eliminating financial incentives for over-prescription. Strengthen regulation of the private sector and enable the private sector to participate in delivering primary health care. Explore innovative approaches to support rational use of drugs and medical technologies.

22
Strategy 3 – Improve efficiency by rationalizing health expenditures (3)
Increase health workforce motivation and career development by analyzing government provided salary levels and performance based financial incentives. Review policies to discourage inappropriate health workforce behaviors affecting health care costs and financial burden borne by households. Monitoring employment in the health sector during the economic crisis Promote home-based care and other services for the elderly and the most vulnerable.

23
Strategy 4 – Increase prepayment and pooling (1)
Improve advocacy and public information to support of government policy commitment and actions needed to achieve UC. Generate country-specific evidence on financial protection against catastrophic and impoverishing health payments. Define appropriate prepayment options, including social health insurance schemes with affordable contributions. Undertake costing of nationally defined health benefit package to advocate universal access. Develop and implement action plans to increase population coverage and access to essential and quality health services.

24
Strategy 4 – Increase prepayment and pooling (2)
Strengthen communication strategies and mechanisms to improve public relations, consumer satisfaction and information on prepayment and pooled mechanisms. Increase awareness and understanding of the prepayment and pooling concepts by the health workforce and leadership to enhance their ability to managing resources effectively and deliver quality health care. Improve coordination, collaboration and capacities to negotiate, purchase, and deliver quality health services supported by standards and norms, legislative and accreditation mechanisms.

25
Health care financing triangle – Asia (O’Donnell, Van Doorslaer et al, 2006)
")
26
Strategy 5 – improve provider payment methods (1)
Evaluate current provider payment methods in country situations and their impacts on HSP and HCF. Ensure free access to PHC by using global budget, salaries and capitation payments to guarantee availability of defined health benefit service package at primary care level. Promulgate clear policy and guidelines on user fees and eliminate charges that complement health workers salaries and other practices that inflate health care costs. Increase consumer awareness, information and education about provider payment methods and their applications by different levels of providers.

27
Strategy 5 – improve provider payment methods (2)
Refrain from introducing and expanding use of fees for services that negatively affect equity, access, poverty and impoverishment associated with catastrophic health spending. Restrict providers’ ability to establish own fees and charges that create additional financial barriers for low income and vulnerable population to accessing healthcare. Replace user fees with prospective and results-oriented payment methods Explore alternative provider payment methods such as diagnostic related groups (DRG), results-based financing (RBF) and pay-for-performance (P4P) where feasible to support better use of financial resources.
, results-based financing (RBF) and pay-for-performance (P4P) where feasible to support better use of financial resources.")
28
Strategy 5 – improve provider payment methods (3)
Establish a mechanism to analyze and monitor the effects of provider payments relative to health financing policy objectives to reduce out-of-pocket payments under pooled financing systems. Assign unit in ministries of health or health insurance agencies responsible for examination, evaluation and introduction alternative provider payment methods with evidence-based advantages over fee-for-service payments. Generate evidence for negotiations with providers to support and participate in designing new payment methods, pilot projects and implementation.

29
Strategy 6 – Strengthen safety-net mechanisms for the poor and vulnerable (1)
Develop and implement policy options to strengthen safety nets for health by removing financial barriers, limiting user fees and eradicating unauthorized charges for publicly financed services. Improve country level data, information and evidence on the major forms of OOP expenditure. Improve methods to estimate the impacts of OOP on different income groups to design effective subsidy benefit uptake by the most needed vulnerable population. Analyze health spending patterns and behaviour for low income and vulnerable groups living near or below local poverty lines.

30
Strategy 6 – Strengthen safety-net mechanisms for the poor and vulnerable (2)
Evaluate and implement premium subsidies, user fee exemptions, conditional cash transfers, and other social assistance schemes for poor and vulnerable groups. Review and assess user fees regulations and practices and their impacts on access, equity and poverty. Strengthen the regulatory framework needed to attain universal coverage and provide effective social safety nets for the poor and vulnerable through established systems.

31
Strategy 7 – Improve evidence and information for policymaking (1)
Promote evidence informed policy decisions and actions by developing and promoting research and studies on macroeconomics and health, costs, effectiveness and benefits of health interventions, and health impacts of the global economic and financial crisis. Establish an anti-crisis unit within the health ministry that can collect and analyze real time data and information to respond rapidly to reduce possible health impacts. Improve health financing data and information by expanding national and sub-national health accounts, international standards and classifications. Improve data availability and quality following international standards and practices on national health accounts.

32
Strategy 7 – Improve evidence and information for policymaking (2)
Provide health policy researchers with training, targeted research topics, and financial support to provide information to not only policy makers and government officials, but also civil society groups. Support studies and dialogues to address the reorientation of health services and reallocation of financial resources to attain universal coverage with pro-public and pro-poor health spending. Review and assemble relevant existing country and region specific studies of health equity and health financing to analyse and monitor their causes through robust health indicators, as well as of improving access to health care services in order to reduce the risk of poverty.

33
Strategy 8 – Improve monitoring and evaluation of policy changes (1)
Strengthen national capacity for monitoring and evaluation. Identify information requirements and gaps in managerial and analytical skills. Train staff in health economics and implementation and monitoring of health financing policies. Integrate health financing indicators into overall health monitoring and evaluation framework. Focus on most important outcomes and report OOP levels for all parts of the health system in a timely manner.

34
Strategy 8 – Improve monitoring and evaluation of policy changes (2)
Transform health financing evaluation results into effective health policies Improve collaboration between researchers and policymakers to ensure that research is directed at outcomes of health financing policy reforms Encourage regional collaboration with other groups doing monitoring and evaluation of health financing reforms. Provide timely reports based on NHA data to health planners to track resource allocations to PHC.

35
Proposed strategy indicators to monitor and evaluate progress
Reducing the share of out-of-pocket payments shares below 30% of total health expenditure; Attain over 90% population coverage by various risk-pooling and prepayment arrangements. Attain 100% coverage of vulnerable populations with social assistance, and safety-net schemes. Increases in public financing by at least 1% of GDP, to reach total health spending of 4-5 % of GDP, with 50-70% of public financing.

Similar presentations
















 in Bangladesh Md. Ashadul Islam Director General Health Economics Unit Ministry of Health and.>")



