Download presentation
Presentation is loading. Please wait.

1
Chapter Quality Network (CQN) Asthma Pilot Project Team Progress Presentation Ohio Chapter Cleveland Clinic Foundation Marymount/ Independence Dr. Michelle Medina Dr. Charles Davis Dr. Richard So Dr. Karen Vargo Joyce Trusnik MA Kathy Maclean LPN Lynda Stamm LPN Ginger Bassett LPN Bridgette Vilella MA

3
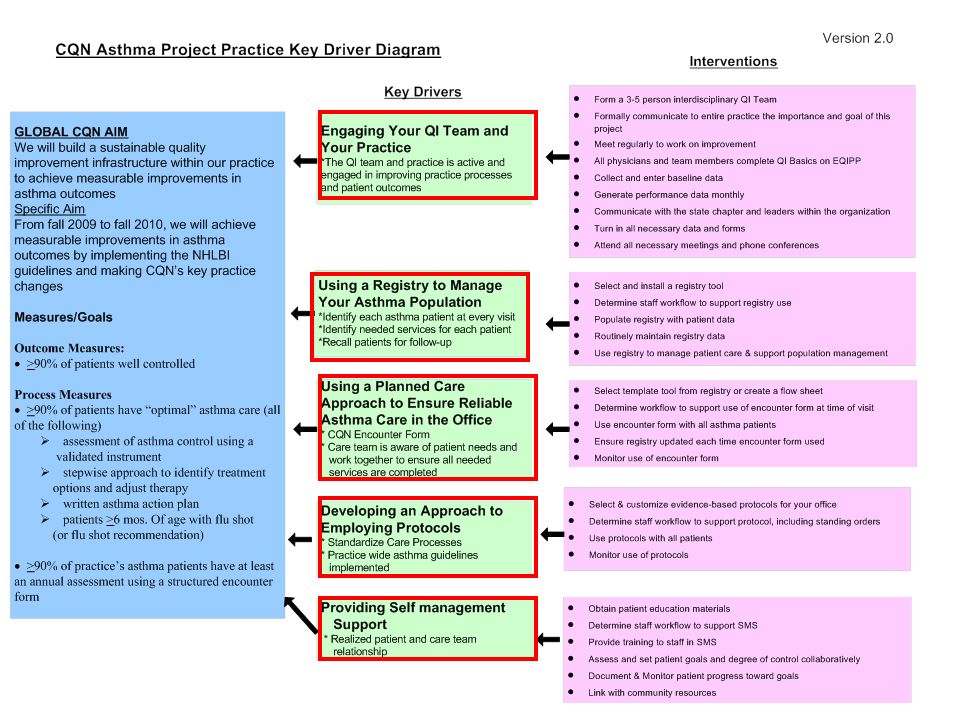
Progress Summary Since Learning Session 1 Key Driver: Engaging your Asthma QI Team and practice Team now composed of 4 doctors, 5 nurses and 1 PSR across 2 sites; have all completed QI basics Doctors have come on-board sequentially Monthly meetings to discuss progress; regular communication by email among team members

4
Progress Summary Since Learning Session 1 Key Driver: Using a Registry to Manage your Asthma population Patient Lists exist that may be used towards a registry Asthmatics at the moment are being identified and surveyed as they come in for appointments but not prospectively At Marymount site, responsibility for maintaining list shared by doctor and MA/RN

5
Progress Summary Since Learning Session 1 Key Driver: Using a Planned Care Approach to ensure Reliable asthma care in the office SmartSets developed within EMR (Epic) Use of SmartSets not universal MDs responsible for loading template within the visit---should MAs do this as they room?
 Use of SmartSets not universal MDs responsible for loading template within the visit---should MAs do this as they room")
6
Asthma Smart Set

7
Progress Summary Since Learning Session 1 Key Driver: Developing an approach to Employing Protocols Use of MaineHealth asthma guidelines flip-charts universal SmartSets incorporate stepwise guidelines and can be accessed in EMR Use of protocols universally has not been tracked

8
Stepwise Guidelines within Smart Set

9
Progress Summary Since Learning Session 1 Key Driver: Providing Self-management Support Online and paper materials available Some nurses/MAs aware of materials and have a long history of using them/ providing teaching Not all nurses/MAs trained yet Collaborative approach with patients is working, with anecdotal positive feedback from families; systematic accounting of goal-setting and degree of control achieved not yet in place

10
Optimal Asthma Care

11
Asthma Action Plan

12
Use of a Validated Instrument to Measure Control

13
Stepwise Approach to Therapy

14
Flu Shot

15
Use of Spirometry To Establish DiagnosisEvery 1-2 years

16
Asthma Complications ED/ Urgent Care VisitsHospitalizations

17
Well Controlled Asthmatics

18
TEST 1 Use CQN form in 5 visits Pre-identified Asthmatics Dr. Medina, MA Marymount office November 2009 PD SA TEST 2 Use CQN form in all visits Pre-identified, newly-identified & Unidentified Asthmatics Dr. Medina, MA, RN, PSR Marymount office December-January 2010 PD SA TEST 3 Track use of CQN form Pre-ID, New-ID, & Un-ID Asthmatics Dr. Medina, MA, RN, PSR Marymount office January- February 2010 PD SA TEST 4 Track use of CQN form All Asthmatic encounters All MDs, RNs, MAs Marymount & Indep office Ongoing PD SA TEST 1 Use CQN form in 5 visits Pre-identified Asthmatics Dr. Davis, Dr. So, LPNs Independence office December 2009 PD SA TEST 2 Use CQN form in all visits Pre-identified, newly-identified & Unidentified Asthmatics Dr. Davis, Dr. So, LPNs Independence office January 2009 PD SA TEST 3 Use CQN form in 5 visits Pre-identified Asthmatics Dr. Vargo, LPN Independence office March 2009 PD SA TEST 4 Track use of CQN form All Asthmatic encounters All MDs, RNs, MAs Marymount & Indep office Ongoing PD SA TEST 1 Provide written asthma plan for 5 Pre-identified Asthmatics Dr. Medina Marymount office November 2009 PD SA TEST 2 Provide written asthma plan Pre-identified, newly-identified & Unidentified Asthmatics Dr. Medina Marymount December – January 2010 PD SA TEST 3 Provide AAP from SmartSet All Asthmatic encounters Dr. Medina Marymount January – February 2010 PD SA TEST 4 Provide AAP from SmartSet/EPIC Templates All Asthmatic encounters All MDs Marymount & Indep office February- April 2010 PD SA Use of encounter formsEngage Independence in QI projectAsthma Action Plan PDSA Ramps

19
Reliability PDSA Aim: To monitor the reliability of use of the CQN Encounter Form in every visit with an Asthmatic PLAN: ID every patient with hx of asthma in MD daily schedule and provide them encounter form DO: MA reviews history/problem list/ directly asks pt about asthma during check-in; MA provides encounter form; MD/RN checks list of asthmatics scheduled against #forms completed at end of the day STUDY: Reliability increased over a period of 7 weeks as more doctors and nursing staff added to study from 45% to 100% ACT: Adopt identification of asthma in MA check-in procedure and recheck sustainability of change in another few weeks

20
Reliability of CQN Form

21
Scheduled asthma patients identified daily (well visit, asthma follow-up visit) by nurse leader; list generated and note attached to appointment schedule Identified asthma patient arrives; MA rooms patient and hands parent/patient asthma patient questionnaire; MA attaches provider questionnaire to visit slip for MD Parent/ patient completes questionnaire and hands form to MD; ensuing discussion based on answers to both questionnaires Management decision- making collaboratively between MD and patient based on NHLBI guidelines Pre-Office Visit During Office Visit Post Visit Activities Nurse Leader compiles encounter forms and assures completeness Nurse leader enters patient data into EQIPP bi-weekly and files paper forms; Each MD reviews run charts regularly; Monthly meeting to discuss progress and plan changes Office Work Flow – CCF Marymount/Independence Patient identified with asthma not previously noted (acute visit, add-on visit, new diagnosis of asthma); MD/MA hands patient questionnaire Other pre-work preparations: MA stocks each room with asthma encounter forms MA ensures available spacers Change in patient’s plan of care: Asthma action plan updated & copy provided Spirometry ordered if indicated Rx escripted; spacer provided Pertinent written asthma materials provided Flu vaccination provided as appropriate Follow up in 2-4 weeks Consults ordered as needed No change in patient’s plan of care: Asthma action plan copy provided Spirometry ordered if indicated Refills escripted; spacer use confirmed Pertinent written asthma materials provided Flu vaccination provided as appropriate Routine follow up MA carries out orders; Patient checks out; PSR schedules appropriate consults and follow-up MD/ MA hands completed forms to Nurse Leader Nurse leader and MD review asthma registry to determine patients who need follow-up (work on registry in progress) Nurse/ MA/ PSR conduct phone follow-up; Appointments scheduled; Nurse may start encounter form based on phone interview
 by nurse leader; list generated and note attached to appointment schedule Identified asthma patient arrives; MA rooms patient and hands parent/patient asthma patient questionnaire; MA attaches provider questionnaire to visit slip for MD Parent/ patient completes questionnaire and hands form to MD; ensuing discussion based on answers to both questionnaires Management decision- making collaboratively between MD and patient based on NHLBI guidelines Pre-Office Visit During Office Visit Post Visit Activities Nurse Leader compiles encounter forms and assures completeness Nurse leader enters patient data into EQIPP bi-weekly and files paper forms; Each MD reviews run charts regularly; Monthly meeting to discuss progress and plan changes Office Work Flow – CCF Marymount/Independence Patient identified with asthma not previously noted (acute visit, add-on visit, new diagnosis of asthma); MD/MA hands patient questionnaire Other pre-work preparations: MA stocks each room with asthma encounter forms MA ensures available spacers Change in patient’s plan of care: Asthma action plan updated & copy provided Spirometry ordered if indicated Rx escripted; spacer provided Pertinent written asthma materials provided Flu vaccination provided as appropriate Follow up in 2-4 weeks Consults ordered as needed No change in patient’s plan of care: Asthma action plan copy provided Spirometry ordered if indicated Refills escripted; spacer use confirmed Pertinent written asthma materials provided Flu vaccination provided as appropriate Routine follow up MA carries out orders; Patient checks out; PSR schedules appropriate consults and follow-up MD/ MA hands completed forms to Nurse Leader Nurse leader and MD review asthma registry to determine patients who need follow-up (work on registry in progress) Nurse/ MA/ PSR conduct phone follow-up; Appointments scheduled; Nurse may start encounter form based on phone interview")
22
CCF CQN Encounter Form Asthma Improvement Project Parent Questionnaire Patient name______________________________DOB __________ Provider name______________________________DOV __________ 1.Has your child visited the Emergency Room or Urgent Care Center due to asthma in the past 12 months? Yes No 2.Has your child been admitted to the hospital due to asthma in the past 12 months? Yes NoIf yes, how many times? Over the previous 2 to 4 weeks, how frequently has your child experienced episodes of cough, shortness of breath, wheezing, or reduced activity due to asthma during the DAY? Less than or equal to 2 days per week More than two days per week but not daily Daily Throughout the day Over the previous 2 to 4 weeks, how frequently has your child experienced episodes of cough, shortness of breath, wheezing or waking up due to asthma at NIGHT? Less than or equal to 2 times per month 3-4 times a month More than 1 time per week but not nightly Often 7 times per week During the past week, how often did your child use a fast acting or quick relief medication, at times other than before exercise? (includes Albuterol, Ventolin®, ProAir®, Proventil®, Xopenex®) Not at all Less than once per day 1-3 times per day 4 or more times per day Not sure How often does asthma limit your child’s activities? Not at all a little of the time Some of the time Most of the time All of the time How many days of school/daycare has your child missed due to asthma in the past 6 months? _______ # of days Does not attend How many work days have you or your spouse missed due to your child’s asthma in the past 6 months? _______ number of days How comfortable are you in your ability to manage your child’s asthma, rated on a scale of 1-10? (Please circle) Not Comfortable =1 2 3 4 5 6 7 8 9 10= Very Comfortable When are asthma symptoms worse? (Check all that apply) Winter Spring Summer Fall During exercise How would you rate your child’s asthma control during the past month? Not controlled at all Poorly controlled Somewhat controlled Well controlled Completely controlled
 Not at all Less than once per day 1-3 times per day 4 or more times per day Not sure How often does asthma limit your child’s activities. Not at all a little of the time Some of the time Most of the time All of the time How many days of school/daycare has your child missed due to asthma in the past 6 months. _______ # of days Does not attend How many work days have you or your spouse missed due to your child’s asthma in the past 6 months. _______ number of days How comfortable are you in your ability to manage your child’s asthma, rated on a scale of (Please circle) Not Comfortable = = Very Comfortable When are asthma symptoms worse. (Check all that apply) Winter Spring Summer Fall During exercise How would you rate your child’s asthma control during the past month. Not controlled at all Poorly controlled Somewhat controlled Well controlled Completely controlled.")
23
CCF CQN Encounter Form Asthma Improvement Project Provider Questionnaire Patient name______________________________DOB __________ Provider name______________________________DOV __________ 3. Were one or more asthma key indicators present when considering the diagnosis of asthma? Yes No Not documented 4. Were lung function measures by spirometry used to establish the asthma diagnosis? Yes No Age inappropriate, younger than 5 years 5. Was a validated instrument used to determine the current level of asthma control? Yes No 6. What is the patient’s current level of control during the past month? Well controlled Not well controlled Very poorly controlled 6b. If “not well controlled” or “very poorly controlled”: Did you identify reason(s) for lack of control? (Examples: exposure to allergens, tobacco smoke, indoor or outdoor pollutants and irritants, non-adherence to medication regimen) Yes No 7. Is spirometry currently scheduled or have results been obtained within the last 1 or 2 years? Yes No Age inappropriate, younger than 5 years 8. Have you used the age-appropriate NHLBI stepwise table used to identify treatment options or to adjust therapy based on asthma control? Yes No 9. Has a flu shot been administered or recommended within the past 12 months? Yes No Patient younger than 6 months or contraindications 10. Does the patient have a written asthma action plan? Yes No 10b. If yes, was the plan updated as needed and reviewed at this visit? Yes No 11. Were asthma self-management education and materials (other than or in addition to the asthma action plan) provided and explained to the patient and family at any visit? Yes No 12. Was a follow-up appointment scheduled to monitor asthma control? Yes No Asthma severity level: Severe Persistent Moderate Persistent Mild Persistent Intermittent Is the patient on a controller medication? Yes No If yes, does the patient/parent report using controller medications daily? Yes No Started this visit For patients who use rescue/controller inhalers, is a spacer utilized? Yes No Not applicable Has the patient received oral corticosteroids for asthma within the past 12 months? Yes No Has the patient been seen by an allergist or pulmonologist during the last 12 months for assistance with asthma management due to severity of illness? Yes No Referred this visit
 for lack of control. (Examples: exposure to allergens, tobacco smoke, indoor or outdoor pollutants and irritants, non-adherence to medication regimen) Yes No 7. Is spirometry currently scheduled or have results been obtained within the last 1 or 2 years. Yes No Age inappropriate, younger than 5 years 8. Have you used the age-appropriate NHLBI stepwise table used to identify treatment options or to adjust therapy based on asthma control. Yes No 9. Has a flu shot been administered or recommended within the past 12 months. Yes No Patient younger than 6 months or contraindications 10. Does the patient have a written asthma action plan. Yes No 10b. If yes, was the plan updated as needed and reviewed at this visit. Yes No 11. Were asthma self-management education and materials (other than or in addition to the asthma action plan) provided and explained to the patient and family at any visit. Yes No 12. Was a follow-up appointment scheduled to monitor asthma control. Yes No Asthma severity level: Severe Persistent Moderate Persistent Mild Persistent Intermittent Is the patient on a controller medication. Yes No If yes, does the patient/parent report using controller medications daily. Yes No Started this visit For patients who use rescue/controller inhalers, is a spacer utilized. Yes No Not applicable Has the patient received oral corticosteroids for asthma within the past 12 months. Yes No Has the patient been seen by an allergist or pulmonologist during the last 12 months for assistance with asthma management due to severity of illness. Yes No Referred this visit.")
24
Key Learnings Change is difficult Change requires motivators that are not always the obvious ones (this is true of patients as it is true of medical staff) To manage a population with chronic disease, a more comprehensive approach needs to be taken
 To manage a population with chronic disease, a more comprehensive approach needs to be taken")
25
Barriers and Successes Majority of practice physicians now engaged Development of SmartSet templates for use in EMR Increased use of written asthma plans Increased use of stepwise approach to therapy Increased patient satisfaction/ comfort level with asthma care at home

26
Barriers and Successes Delayed engagement to project and differential start among physicians Non-universal use of SmartSet templates among physicians/ patient sets/ visit type “Easy” way not always the “consistent” way Time required for each visit

27
Future Plans Increase functionality of current patient lists Engage MDs, RNs, MAs, PSRs in maintaining patient lists Determine staff workflow to increase compliance with protocols (ie, standing orders) Monitor MD use of protocols (chart review?) Engage RNs who provide nurse triage to use action plans Engage other staff in asthma education Patient survey of engagement/ satisfaction
 Monitor MD use of protocols (chart review ) Engage RNs who provide nurse triage to use action plans Engage other staff in asthma education Patient survey of engagement/ satisfaction")
28
Scheduled asthma patients identified daily (well visit, asthma follow-up visit) by nurse leader; list generated and note attached to appointment schedule Identified asthma patient arrives; MA /LPN rooms patient and hands parent/patient asthma patient questionnaire; MA/LPN attaches provider questionnaire to visit slip for MD; MA/LPN drops in Asthma SmartSet Parent/ patient completes questionnaire and hands form to MD; ensuing discussion based on answers to both questionnaires Management decision- making collaboratively between MD and patient based on NHLBI guidelines Pre-Office Visit During Office Visit Post Visit Activities Nurse Leader compiles encounter forms and assures completeness Nurse leader enters patient data into EQIPP bi-weekly and files paper forms; Each MD reviews run charts regularly; Monthly meeting to discuss progress and plan changes; Chart review to monitor use of protocols Proposed Changes to Office Work Flow – CCF Marymount/Independence Patient identified with asthma not previously noted (acute visit, add-on visit, new diagnosis of asthma); MA hands patient questionnaire; MA/LPN drops in Asthma SmartSet Other pre-work preparations: MA /LPN stocks each room with asthma encounter forms MA/LPN ensures available spacers Each patient room stocked with education materials / terminal has links to asthma education Change in patient’s plan of care: Asthma action plan updated & copy provided Spirometry ordered if indicated Rx escripted; spacer provided Pertinent written asthma materials provided Flu vaccination provided as appropriate Follow up in 2-4 weeks Consults ordered as needed No change in patient’s plan of care: Asthma action plan copy provided Spirometry ordered if indicated Refills escripted; spacer use confirmed Pertinent written asthma materials provided Flu vaccination provided as appropriate Routine follow up MA /LPN carries out orders; MA/LPN/RN provides/ reinforces asthma education ; Patient checks out; PSR schedules appropriate consults and follow-up MD/ MA hands completed forms to Nurse Leader Nurse leader and MD review asthma registry to determine patients who need follow-up Nurse/ MA/ LPN/ PSR conduct phone follow-up; Appointments scheduled; Nurse may start encounter form based on phone interview
 by nurse leader; list generated and note attached to appointment schedule Identified asthma patient arrives; MA /LPN rooms patient and hands parent/patient asthma patient questionnaire; MA/LPN attaches provider questionnaire to visit slip for MD; MA/LPN drops in Asthma SmartSet Parent/ patient completes questionnaire and hands form to MD; ensuing discussion based on answers to both questionnaires Management decision- making collaboratively between MD and patient based on NHLBI guidelines Pre-Office Visit During Office Visit Post Visit Activities Nurse Leader compiles encounter forms and assures completeness Nurse leader enters patient data into EQIPP bi-weekly and files paper forms; Each MD reviews run charts regularly; Monthly meeting to discuss progress and plan changes; Chart review to monitor use of protocols Proposed Changes to Office Work Flow – CCF Marymount/Independence Patient identified with asthma not previously noted (acute visit, add-on visit, new diagnosis of asthma); MA hands patient questionnaire; MA/LPN drops in Asthma SmartSet Other pre-work preparations: MA /LPN stocks each room with asthma encounter forms MA/LPN ensures available spacers Each patient room stocked with education materials / terminal has links to asthma education Change in patient’s plan of care: Asthma action plan updated & copy provided Spirometry ordered if indicated Rx escripted; spacer provided Pertinent written asthma materials provided Flu vaccination provided as appropriate Follow up in 2-4 weeks Consults ordered as needed No change in patient’s plan of care: Asthma action plan copy provided Spirometry ordered if indicated Refills escripted; spacer use confirmed Pertinent written asthma materials provided Flu vaccination provided as appropriate Routine follow up MA /LPN carries out orders; MA/LPN/RN provides/ reinforces asthma education ; Patient checks out; PSR schedules appropriate consults and follow-up MD/ MA hands completed forms to Nurse Leader Nurse leader and MD review asthma registry to determine patients who need follow-up Nurse/ MA/ LPN/ PSR conduct phone follow-up; Appointments scheduled; Nurse may start encounter form based on phone interview")
Similar presentations


 Asthma.>")

 Asthma Pilot Project Team Progress Presentation State Name: Alabama Practice Name: Dothan Pediatric Clinic Team Members:>")

 Asthma Pilot Project Team Progress Presentation State Name: Ohio Practice Name : Locust Pediatric Care Group Team Members:>")






 Asthma Pilot Project Team Progress Presentation State Name: Alabama Practice Name: Partners in Pediatrics, LLC.>")


 Asthma Pilot Project Team Progress Presentation State Name: Oregon Practice Name:PHMG-Barger Pediatrics Team Members: Lorna.>")
 Michael A. Ross, MD FAAP American Academy.>")
 Asthma Pilot Project Team Progress Presentation Oregon Oregon Hillsboro Pediatric Clinic, LLC Hillsboro Pediatric Clinic,>")
 Asthma Pilot Project Team Progress Presentation State Name: Alabama Practice: Charles Henderson Child Health Center Team.>")