Download presentation
Presentation is loading. Please wait.

1
Use of Chemotherapy plus a Monoclonal Antibody (Trastuzumab) against HER2 for Metastatic Breast Cancer That Overexpresses HER2 Dennis J. Slamon, M.D., Ph.D., Brian Leyland-Jones, M.D., Steven Shak, M.D., Hank Fuchs, M.D., Virginia Paton, Pharm.D., Alex Bajamonde, Ph.D., Thomas Fleming, Ph.D., Wolfgang Eiermann, M.D., Janet Wolter, M.D., Mark Pegram, M.D., Jose Baselga, M.D., and Larry Norton, M.D. NEJM. Volume 344:783-792, March 15, 2001, Number 11

2
The Facts HER2neu: amplified in 25-30% of malignant breast CA F w/ breast CA that overexpress HER2 – Aggressive disease with significantly shortened disease-free survival and overall survival Lab studies: amplification of HER2 has a direct role in the pathogenesis of these cancers; therapeutic drug development

3
Trastuzumab Trastuzumab was noted to inhibit tumor growth when used alone – synergistic when used in combination with Cisplatin, carboplatin, docetaxel and ionizing radiation – additive effects when used with Doxorubicin, cyclophosphamide, methotrexate and paclitaxel

4
Clinical Question Is there a significant difference in the time to disease progression, incidence of adverse effects, rates and duration of responses, time to treatment failure and overall survival of female patients (ages 25-77, with breast CA that overexpressed HER2) that underwent chemotherapy alone and chemotherapy w/ trastuzumab?
 that underwent chemotherapy alone and chemotherapy w/ trastuzumab")
5
The Objective of the Study The objective of the study is to compare the time to disease progression, incidence of adverse effects, rates and duration of responses, time to treatment failure and overall survival of female patients (ages 25-77, with breast CA that overexpressed HER2) that underwent chemotherapy alone and chemotherapy w/ trastuzumab.
 that underwent chemotherapy alone and chemotherapy w/ trastuzumab.")
6
Main Outcome Measures End points – Time to disease progression – Incidence of adverse effects – Rates and the duration of responses – Time to treatment failure – Overall survival

7
Methodology

8
Patients Women with progressive metastatic breast cancer that overexpressed HER2 who had not previously received chemotherapy for metastatic disease were eligible for the study. The level of expression of HER2 was determined by immunohistochemical analysis in a central laboratory. Only patients who had weak-to-moderate staining of the entire tumor-cell membrane for HER2 (referred to as a score of 2+) or more than moderate staining (referred to as a score of 3+) in more than 10 percent of tumor cells on immunohistochemical analysis were eligible for the study.
 or more than moderate staining (referred to as a score of 3+) in more than 10 percent of tumor cells on immunohistochemical analysis were eligible for the study..")
9
Excluded Women with: – Bilateral breast cancer – Untreated brain metastases – Osteoblastic bone metastases – Pleural effusion or ascites as the only evidence of disease – A second type of primary cancer, or a Karnofsky score of less than 60. – Pregnant – Received any type of investigational agent within 30 days before the study began.

10
Treatment: Chemotherapy Alone Consisted of an anthracycline: – Doxorubicin = 60 mg per square meter of body-surface area or – Epirubicin = 75 mg per square meter) Cyclophosphamide = 600 mg per square meter) for patients who had never before received an anthracycline, or Paclitaxel = 175 mg per square meter) for patients who had received adjuvant (postoperative) anthracycline. Administered once every three weeks for six cycles, and additional cycles were administered at the investigator's discretion. Chemotherapy Plus Trastuzumab Trastuzumab was administered intravenously in a loading dose of 4 mg per kilogram of body weight, followed by a dose of 2 mg per kilogram once a week, until there was evidence of disease progression.

11
Treatment On the detection of disease progression, patients were given the option of entering a nonrandomized, open-label study in which trastuzumab was administered at the same doses alone or in combination with other therapies. Sixty-six percent of such patients elected to do so

12
Efficacy Patients were evaluated for a response at weeks 8 and 20 and then at 12-week intervals by the members of an independent response-evaluation committee, who were unaware of the patients' treatment assignments. A complete response was defined as the disappearance of all tumor on the basis of radiographic evidence, visual inspection, or both. A partial response was defined as a decrease of more than 50 percent in the dimensions of all measurable lesions.

13
Efficacy Disease progression was defined as an increase of more than 25% in the dimensions of any measurable lesion. The primary study end point was the time to disease progression. Pre-specified secondary end points were the rate of objective response, the duration of a response, the time to treatment failure (a composite of disease progression, death, discontinuation of treatment, and the use of other types of antitumor therapy), and survival as of October 1999.
, and survival as of October")
14
Adverse Events Clinical assessments were performed at base line, at specified times, and at the time the patient was removed from the study by an independent cardiac evaluation committee whose members were unaware of patients' treatment assignments. Adverse events were classified as mild, moderate, or severe. Abnormalities in laboratory values were classified by the grading system of the World Health Organization and cardiac dysfunction by the criteria of the New York Heart Association.

15
Statistical Analysis Estimated that 450 patients would be needed in order for the study to detect at a power of 90 percent a 50 percent increase in the median time to disease progression, given a median time to progression of eight months in the subgroups receiving chemotherapy alone and a significance level of 0.05 with the use of a two-tailed log-rank test. All end points were analyzed according to the intention-to-treat principle. The primary analysis of all efficacy variables was performed on data pooled from both chemotherapy regimens.

16
Statistical Analysis Additional analyses were performed within each chemotherapy group. The time to the various end points was analyzed with the use of Kaplan–Meier methods, and a two-sided log-rank test was used to compare the groups. The rate of objective response was analyzed with the use of normal approximation methods; a two- sided chi-square test was used to compare the groups.

17
Results

18
469 patients enrolled between June 1995 and March 1997 – 5 patients were never treated – 2 declined treatment – 1 died before treatment was begun – 1 had disease progression at enrollment – 1 was enrolled inadvertently. chemotherapy plus trastuzumab - median time in the study was 40 weeks. chemotherapy alone – median time in study was 25 weeks – a reflection of the longer time to disease progression in the group that received combination treatment trastuzumab.

19
Baseline Characteristics of Patients

20
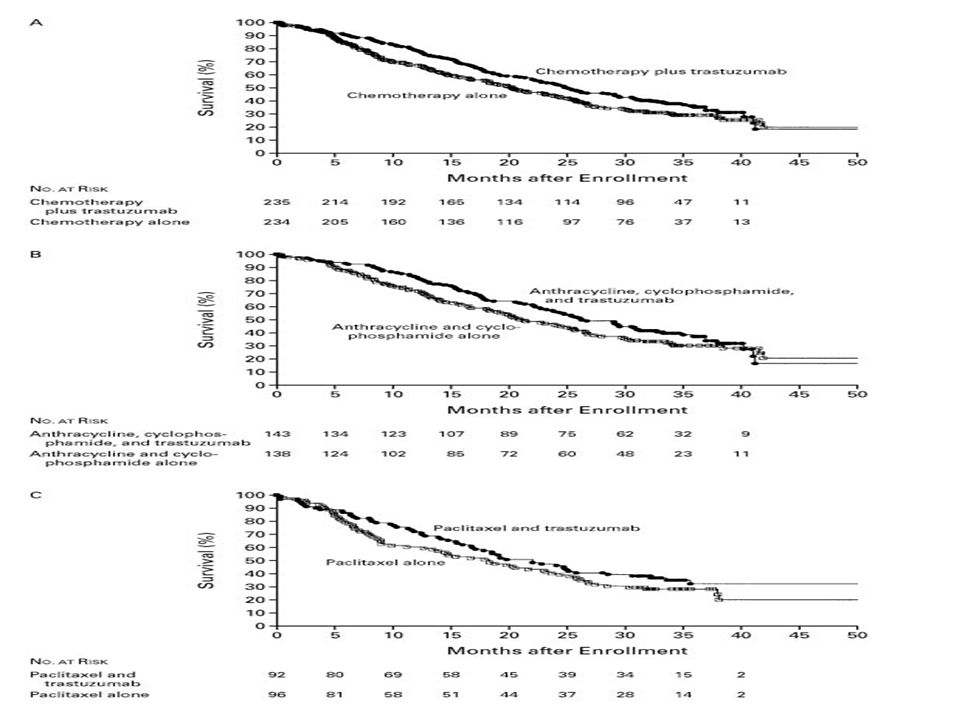
Efficacy Chemotherapy plus trastuzumab - median time to disease progression was 7.4 months – anthracycline, cyclophosphamide, and trastuzumab median time to progression 7.8 months – paclitaxel and trastuzumab median time to progression, 6.9 months Chemotherapy alone - median time to disease progression was 4.6 months. – 6.1 month median time progression in the subgroup given only anthracycline and cyclophosphamide – 3.0 months in the group given paclitaxel alone

21
Results of an Intention-to-Treat Analysis of the End Points

22
Results Chemotherapy plus trastuzumab compared to chemotherapy alone associated with: – a significantly higher rate of overall response (50 percent vs. 32 percent) – a longer duration of response (median 9.1 vs. 6.1 months) – a longer time to treatment failure (median, 6.9 vs. 4.5 months).
 – a longer duration of response (median 9.1 vs. 6.1 months) – a longer time to treatment failure (median, 6.9 vs. 4.5 months)..")
24
Results Chemotherapy plus trastuzumab also associated with a significantly lower rate of death at one year – (22 percent, as compared with 33 percent in the group given chemotherapy alone) The median survival was 25.1 months in the group given chemotherapy plus trastuzumab and 20.3 months in the group that received chemotherapy alone. – The calculation included patients in the group given chemotherapy alone who received open-label trastuzumab after the occurrence of disease progression. The risk of death was reduced by 18 to 20 percent in the subgroups given trastuzumab. The efficacy of trastuzumab was consistently observed in both subgroups who were given trastuzumab; however, patients with a score of 3+ for the overexpression of HER2 benefited to a greater degree from such treatment than those with a score of 2+.

26
Results: Deaths 314 patients had died – 149 in the groupgiven chemotherapy plus trastuzumab and 165 in the group givenchemotherapy alone – As of October 2009 95 percent of these deaths were attributedto progressive disease. Two deaths, both in patients who hadreceived an anthracycline, cyclophosphamide, and trastuzumab,were possibly related to trastuzumabtherapy – one patient diedof sepsis after 2 doses of trastuzumab – the second diedof hepatitis B–related hepatorenal syndrome after 11 dosesof trastuzumab.

27
Results: Adverse Events Approximately 25 percent of patients had chills, fever, or bothduring the initial infusion of trastuzumab. Slowing the infusionrate ameliorated these symptoms. No episodes of frank anaphylaxisoccurred, but one patient had moderate hypotension, and threehad mild bronchospasm, all of which resolved without treatment. Infection occurred in 47 percent of patients who were givenchemotherapy plus trastuzumab and in 29 percent of those treatedwith chemotherapy alone (Table 4).
..")
29
Results: Adverse Events These infections consistedof: – mild-to-moderate infections of the upper respiratory tract ( 72 percent% – catheter-related infections (9 %) – viral syndrome (3%) – other types of infections ( 16 %). The addition of trastuzumab to the chemotherapy regimen increasedthe frequency of leukopenia and anemia (Table 4). – These casesof cytopenia were mild to moderate in severity and did not necessitatethe discontinuation of trastuzumab or withdrawal from the study.
. – These casesof cytopenia were mild to moderate in severity and did not necessitatethe discontinuation of trastuzumab or withdrawal from the study..")
30
Results: Adverse Events Eighteen patients (15 in the subgroup givenan anthracycline, cyclophosphamide, and trastuzumab and 3 inthe subgroup given paclitaxel and trastuzumab) had clinicalsigns of cardiac dysfunction. Two additional adverse eventswere attributed to trastuzumab therapy: – embolic stroke asa possible complication of cardiac dysfunction – chest painafter 49 doses of trastuzumab and six cycles of an anthracyclineand cyclophosphamide

31
Results: Cardiotoxicity This review identified 63 patientswith symptomatic or asymptomatic cardiac dysfunction – 39 of143 patients had received an anthracycline, cyclophosphamide,and trastuzumab (accounting for 27 percent of this subgroup) – 11 of 135 had received an anthracycline and cyclophosphamidealone (incidence, 8 percent) – 12 of 91 had received paclitaxeland trastuzumab (incidence, 13 percent) – 1 of 95 had receivedpaclitaxel alone (incidence, 1 percent
 – 11 of 135 had received an anthracycline and cyclophosphamidealone (incidence, 8 percent) – 12 of 91 had received paclitaxeland trastuzumab (incidence, 13 percent) – 1 of 95 had receivedpaclitaxel alone (incidence, 1 percent")
32
Results: Cardiotoxicity Incidence of cardiac dysfunction of New York Heart Associationclass III or IV was highest among patients who had receivedan anthracycline, cyclophosphamide, and trastuzumab – 16 percent,as compared with 3 percent among patients who had received ananthracycline and cyclophosphamide alone, 2 percent among thosewho had received paclitaxel and trastuzumab, and 1 percent amongthose who had received paclitaxel alone

33
Results: Cardiotoxicity Of the 63 patients with cardiac dysfunction, 44 received standardmedical treatment. – The condition improved in 33 of these 44patients, did not change in 5, and worsened in 4. – Among the five patientswith persistent class III or IV cardiac dysfunction, three werein the group given an anthracycline, cyclophosphamide, and trastuzumab. Increasing age was the only base-line characteristic that wasa significant risk factor for cardiac dysfunction in patientswho were receiving the combination of an anthracycline, cyclophosphamide,and trastuzumab.

34
Discussion Trastuzumab-based combination therapy was effective; it reduced the relative risk of death by 20% at a median follow-up of 30 mos. Few studies of metastatic breast cancer have demonstrated a survival advantage of this magnitude in association with the addition of a single agent.

35
Discussion Particularly noteworthy is that 2/3 of patients who were initially assigned to receive chemotherapy alone began, after disease progression, to receive open-label trastuzumab alone or with chemotherapy. Such a crossover design would generally reduce the likelihood that a survival advantage would be found. Significant increases in the time to disease progression, the rates of response, the duration of responses, and the time to treatment failure were observed in both subgroups that were given chemotherapy plus trastuzumab

36
Toxic Effects Adverse effect: cardiac dysfunction Greater risk of cardiac dysfunction – concurrent tx w/ TZM, anthracycline, cyclophosphamide VS treatment with anthracycline, cyclophosphamide Drug discontinued in 18/235 patients (8%); patients initially received anthracycline, cyclophosphamide and TZM.
; patients initially received anthracycline, cyclophosphamide and TZM.")
37
Toxic Effects Continued use of trastuzumab did not cause further cardiac deterioration in most patients, and cardiac function improved in 75% of patients after the initiation of standard medical care Old age: significant risk factor for cardiac dysfunction. Mechanism of cardiotoxicity: unknown.

38
Can the results help me in caring for the patient? Yes

39
Will the reproducibility of the test and its interpretation be satisfactory in my setting ? Yes, however, the price of the drug has to be considered; it is very expensive and it might not be accessible to all patients here in our country

40
Are the results applicable to my patient ? Yes, the subjects of the study were female patients, ages 25-77, with breast CA that overexpressed HER2

41
Will the results change my management ? Yes, considering the efficacy of trastuzumab in improving overall survival, increasing time to disease progression, the rates of response, the duration of responses, and the time to treatment failure The incidence of adverse effects of the drug is minimal; benefits outweight risks

42
Resolution of the Problem Given the extremely poor prognosis of patients with HER2-(+) metastatic breast cancer, the cardiotoxicity of trastuzumab must be weighed against its potential clinical benefit. Risks will necessitate great caution in its use, especially when it is combined with an anthracycline

43
Resolution of the Problem Benefits outweigh risks Concurrent treatment with trastuzumab and first-line chemotherapy was associated with a significantly longer time to disease progression, a higher rate of response, a longer duration of response, and improved overall survival.

Similar presentations


 Phase III trial comparing AC (x4)taxane (x4) with taxane (x8) as adjuvant therapy for node-positive breast cancer: Results of N-SAS-BC02.>")



 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")


 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")

: a randomised phase 3 trial Speaker: 陳鴻明.>")



: ENESTnd Beyond One Year Larson.>")
 with Newly Diagnosed Multiple Myeloma (NDMM) Receiving Lenalidomide and Low-Dose Dexamethasone.>")
: investigational agents TTP = median time to disease progression OS = median overall survival.>")
>")
 in combination with hormone therapy for treatment of castration resistant prostate cancer.>")
>")
 upregulation Dose- and time-dependent upregulation of TP in human colon cancer xenografts 20 15 10 5 0 20 15 10 5 0 PaclitaxelDocetaxel.>")