Download presentation
Presentation is loading. Please wait.

1
Evaluation and Intervention for the Persistently Ill Schizophrenic Person S. Charles Schulz, M.D. Professor and Head, Department of Psychiatry scs@umn.edu Peter Milev, M.D., Ph.D. Assistant Professor, Department of Psychiatry Katherine Cornelius, B.S. Staff Member, Department of Psychiatry

2
Disclosure In the last year, Dr. Schulz has had financial relationships with the following companies: AstraZeneca – Investigator initiated grant Eli Lilly – Consultant; Investigator initiated grant NIMH – Clinical Scholar Training (Co- Investigator)
.")
3
Overview of Treatment Refractory Schizophrenia Significance Definitions Psychosocial Issues Initial Pharmacological Approaches Role of Augmenting Medications Clozapine Treatment – Alone and in Combination Conclusions

4
Significance and Prevalence of Treatment Refractory Schizophrenia Using criteria of significant symptoms after adequate trials of medications, non-response is estimated to be between 30-40%. The figure is lower in first episode samples. Treatment refractory illness is associated with patient and family suffering, increased aggressive behaviors and increased time in hospitals… Despite the high prevalence and impact, treatment refractory illness has not received appropriate attention in recent years.

5
Underutilization of Clozapine “Two clear antipsychotic trial failures warrant initiation of clozapine, and long delays in clozapine treatment should be avoided.” 1999 data from Novartis (manufacturer of clozapine) estimated 160,000…received a trial of clozapine… Using percentages of non-responders, it appears that only 25% of non-responders ever received clozapine. Moore, TA et al. (2007). The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia. J Clin Psychiatry. 68:1751-62.
. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia. J Clin Psychiatry. 68:")
6
Definitions of Non-Response Hirsch, SR and Weinberger D. (2003). Schizophrenia. Malden, Massachusetts: Blackwell Publishing.
. Schizophrenia. Malden, Massachusetts: Blackwell Publishing..")
7
Definition of Non-Response Beyond “Treatment of Last Resort” Remission in Schizophrenia – Criteria for response to treatment with objective measures over time “should support a positive, longer term approach…” Poor response in one area – e.g. aggression, suicidality Co-morbidity – e.g. depression, OCD Andreasen NC. et al. (2005). Remission in Schizophrenia: Proposed criteria and rationale for consensus. Am J Psychiatry. 162:441-9.
. Remission in Schizophrenia: Proposed criteria and rationale for consensus. Am J Psychiatry. 162:")
8
The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements The Schizophrenia Patient Outcomes Research Team (PORT) provides a summary of evidence based psychosocial treatment. This article updates the previous reports after the group’s examination by the literature The review led to identification of 8 recommendations: Assertive community treatment Supported Employment CBT Family based services Token economy Skills training Interventions for SA Interventions for weight Dixon LB. et al. (2010). The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophr Bull. 36:48-70.
. The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophr Bull. 36:")
9
Wykes, T. et al. (2008). Cognitive Behavior Therapy for Schizophrenia: Effect Sizes, Clinical Models and Methodological Rigor. Schizophr Bull. 34:523-537

10
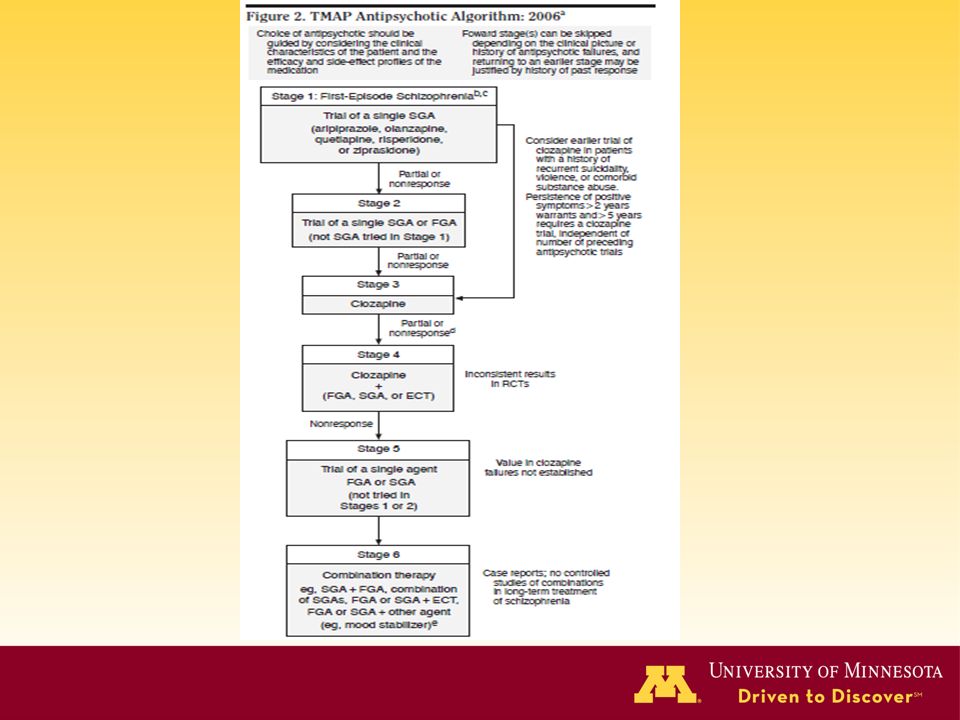
The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update Background: A panel met to examine evidence in pharmacologic treatment of schizophrenia to update and revise TMAP Method: Four questions were identified prior to the meeting – subgroups reviewed evidence. Results: The algorithm was updated along the following lines: 1.First-episode patients should be started on lower doses. 2.FGAs included in stages after first episode 3.Two trials of antipsychotic medications should proceed clozapine – earlier use may be considered for suicidality, co-morbid violence, or substance abuse. 4.Augmentation to clozapine may be considered. Conclusions: The authors note this framework is to augment decision making. Moore TA. et al. (2007). The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry. 68:1751-62
. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry. 68:")
12
Role of Augmenting Medications – Early Studies Empiric evidence for adding non-neuroleptic medications began in the 1970s with recently approved, lithium carbonate

13
Further Studies with Lithium

14
Four Cochrane Reviews of Non- Neuroleptics for Schizophrenia Lithium 1 – No evidence it works by itself. No superior efficacy for augmentation Valproate 2 – No evidence for efficacy by itself. Some suggestion of use in aggression and T.D. Benzodiazepines 3 – Randomized trials not sufficient to support use of benzodiazepines alone or as an augmenting agent. Short-term sedation seen. Carbamazepine 4 – Current evidence does not support use of carbamazepine either by itself or as an augmenting agent for schizophrenia. 1. Leucht S. et al. (2007). Lithium for schizophrenia. Cochrane Database Syst Rev. 18:CD003834. 2. Schwarz C. et al. (2008). Valproate for schizophrenia. Cochrane Database Syst Rev. 16:CD00028. 3. Volz A. et al. (2007). Benzodiazepines for schizophrenia. Cochrane Database Syst Rev. 24:CD006391. 4. Leucht S. et al. (2007). Carbamazepine for schizophrenia. Cochrane Database Syst Rev. 18:CD001258.
. Lithium for schizophrenia. Cochrane Database Syst Rev. 18:CD Schwarz C. et al. (2008). Valproate for schizophrenia. Cochrane Database Syst Rev. 16:CD Volz A. et al. (2007). Benzodiazepines for schizophrenia. Cochrane Database Syst Rev. 24:CD Leucht S. et al. (2007). Carbamazepine for schizophrenia. Cochrane Database Syst Rev. 18:CD")
15
Adding Lithium or Anticonvulsants to Antipsychotics for the Treatment of Schizophrenia: Useful strategy or Exercise in Futility High rates of patients with schizophrenia in NY Office of Mental Health receive lithium or anticonvulsants as adjunctive medications (50%). The author reviews recent augmenting strategy studies with lamotrigine and extended release divalproex which did not show a statistical advantage. Older studies examining carbamazepine, lithium, and topiramate were also discussed and little data supporting their use was noted. The author notes little support for the non- neuroleptic augmenting agents, yet goes on to discuss use. Citrome L. (2009). Adding Lithium or Anticonvulsants to Antipsychotics for the Treatment of Schizophrenia: Useful strategy or Exercise in Futility. J Clin Psychiatry. 70:932-3.
. Adding Lithium or Anticonvulsants to Antipsychotics for the Treatment of Schizophrenia: Useful strategy or Exercise in Futility. J Clin Psychiatry. 70:")
16
Adding Lithium or Anticonvulsants to Antipsychotics for the Treatment of Schizophrenia: Useful strategy or Exercise in Futility (Continued) “While this review indicates little evidence for the effectiveness of adjunctive mood stabilizers in most patients with schizophrenia, there may be individual patients who benefit from anticonvulsants or lithium. These are patients who appear to benefit when these agents are added, deteriorate when they are withdrawn, and improve again when they are reinstated, thus making the case for an “N of 1” efficacy trial.” Citrome L. (2009). Adding Lithium or Anticonvulsants to Antipsychotics for the Treatment of Schizophrenia: Useful strategy or Exercise in Futility. J Clin Psychiatry. 70:932-3.
. Adding Lithium or Anticonvulsants to Antipsychotics for the Treatment of Schizophrenia: Useful strategy or Exercise in Futility. J Clin Psychiatry. 70:")
17
Clozapine Treatment Kane et al. (1988) 1 – A “treatment of last resort” in which 30% of clozapine patients responded compared to 4% on chlorpromazine. Pickar et al. (1992) 2 – In a 16 week trial at NIMH- IRP, 38% response rate. Kane et al. (2001) 3 – This 29 week study reported a 60% response rate. 1. Kane, J. et al. (1988) Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry, 45, 789-796. 2. Pickar, D. et al. (1992) Clinical and biologic response to clozapine in patients with schizophrenia. Crossover comparison with fluphenazine. Arch Gen Psychiatry, 49, 345-353. 3. Kane, J. M. et al. (2001) Clozapine and haloperidol in moderately refractory schizophrenia: a 6-month randomized and double-blind comparison. Arch Gen Psychiatry, 58, 965-972.
 1 – A treatment of last resort in which 30% of clozapine patients responded compared to 4% on chlorpromazine. Pickar et al. (1992) 2 – In a 16 week trial at NIMH- IRP, 38% response rate. Kane et al. (2001) 3 – This 29 week study reported a 60% response rate. 1. Kane, J. et al. (1988) Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry, 45, Pickar, D. et al. (1992) Clinical and biologic response to clozapine in patients with schizophrenia. Crossover comparison with fluphenazine. Arch Gen Psychiatry, 49, Kane, J. M. et al. (2001) Clozapine and haloperidol in moderately refractory schizophrenia: a 6-month randomized and double-blind comparison. Arch Gen Psychiatry, 58,")
18
Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatment Objective: to assess next steps for schizophrenic patients who have an inadequate response to treatment with an antipsychotic medication (second generation meds). Methods: Patient with generally inadequate response were assigned to clozapine or an atypical antipsychotic medication Results: Time to discontinuation was longest for clozapine (10.5 months). PANSS scores were significantly lower at 3 months for clozapine than quetiapine or risperidone, but not olanzapine. Conclusion: Authors note that for patients who “failed to improve with an atypical antipsychotic, clozapine was more effective than switching to another newer atypical antipsychotic.” McEvoy J.P. (2006). Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatment. Am J Psychiatry. 163:600-10.
. PANSS scores were significantly lower at 3 months for clozapine than quetiapine or risperidone, but not olanzapine. Conclusion: Authors note that for patients who failed to improve with an atypical antipsychotic, clozapine was more effective than switching to another newer atypical antipsychotic. McEvoy J.P. (2006). Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatment. Am J Psychiatry. 163:")
19
Atypical antipsychotic agents in the treatment of violent patients with schizophrenia and schizoaffective disorder Objective: To examine clozapine, olanzapine and haloperidol in the treatment of assault and aggressive behavior in patients with schizophrenia/schizoaffective disorder. Design: A randomized and double-blind trial of the 3 medications in 110 subjects. Aggressive events and symptoms were measured. Results: Clozapine was better than olanzapine and haloperidol in reducing number and severity of assaults and in reducing overall aggression. The medications were similar in effect on PANSS scores. Olanzapine was superior to haloperidol. Conclusions: The authors note clozapine to be more effective in reducing aggression. They note this was separate from treating psychosis or sedation. Karkowski MI. et al. (2006). Atypical antipsychotic agents in the treatment of violent patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry. 63:622-9.
. Atypical antipsychotic agents in the treatment of violent patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry. 63:")
20
Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Background: Authors note that 50% of schizophrenic or schizoaffective patients attempt suicide and 10% die of suicide. Early studies suggest clozapine may help. Method: A double-blind comparison of clozapine v. olanzapine was conducted in 980 patients who were considered at risk for suicide. Patients were seen frequently and equally. Objective rating scales were used. Results: There was less suicidal behavior in clozapine treated patients (p=0.03). Other measures were also significant for clozapine treatment. Very few patients completed suicide (5 on clozapine; 3 on olanzapine). Conclusions: The authors note that use of clozapine “should lead to a significant reduction in suicidal behavior.” Meltzer HY. et al. (2003). Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry. 60:82-91.
. Other measures were also significant for clozapine treatment. Very few patients completed suicide (5 on clozapine; 3 on olanzapine). Conclusions: The authors note that use of clozapine should lead to a significant reduction in suicidal behavior. Meltzer HY. et al. (2003). Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry. 60:")
21
The efficacy of lamotrigine in clozapine- resistant schizophrenia: A systematic review and meta-analysis Background: Authors note that clozapine is a treatment of choice for non-response and that there is frequent poly-pharmacy. They examined the use of lamotrigine in clozapine-resistant patients Results: Five studies of lamotrigine added to clozapine were identified. A total of 161 patients were identified. Lamotrigine was superior to placebo in primary outcome (p<0.001) as well as positive and negative symptoms. Conclusions: The authors concluded that the augmentation strategy may be effective for clozapine resistant schizoprhenia. Tiihonen J. et al. (2009). The efficacy of lamotrigine in clozapine-resistant schizophrenia: A systematic review and meta-analysis. Schizophrenia Research. 109:10-4.
 as well as positive and negative symptoms. Conclusions: The authors concluded that the augmentation strategy may be effective for clozapine resistant schizoprhenia. Tiihonen J. et al. (2009). The efficacy of lamotrigine in clozapine-resistant schizophrenia: A systematic review and meta-analysis. Schizophrenia Research. 109:")
22
11-year Follow-up of Mortality in Patients with Schizophrenia: A Population-based Cohort Study Background: To examine the effect of antipsychotic medications on mortality using a nationwide registry. Methods: Mortality in 66,881 patients was compared to total population (5.2 million) and then assessed for medication exposure during 1996-2006. Results: Use of second generation antipsychotics rose from 13% to 64% during the study period. The gap in mortality did not raise (1996, 25 years; 2006, 22.5 years). Of the second generation medications compared to perphenazine, the lowest mortality was seen for clozapine (p=0.0045). Longer term treatment with any medication led to lower mortality. Interpretation: Longer-term treatment with antipsychotics lead to lower mortality. Examination of clozapine use should be examined. Tiihonen J. et al. (2009). 11-year Follow-up of Mortality in Patients with Schizophrenia: A Population-based Cohort Study. Lancet. 374:620-7.
 and then assessed for medication exposure during Results: Use of second generation antipsychotics rose from 13% to 64% during the study period. The gap in mortality did not raise (1996, 25 years; 2006, 22.5 years). Of the second generation medications compared to perphenazine, the lowest mortality was seen for clozapine (p=0.0045). Longer term treatment with any medication led to lower mortality. Interpretation: Longer-term treatment with antipsychotics lead to lower mortality. Examination of clozapine use should be examined. Tiihonen J. et al. (2009). 11-year Follow-up of Mortality in Patients with Schizophrenia: A Population-based Cohort Study. Lancet. 374:")
23
A randomized controlled trial of cognitive- behavioral therapy for persistent symptoms in schizophrenia resistant to medication Background: Early evidence of CBT in drug-refractory positive symptoms in schizophrenia. Methods: Patients assigned to CBT designed for schizophrenia versus “befriending” over 9 months with a 9 month follow-up. Results: Ninety patients were entered with an average of 19 sessions. There were no difference during the treatment periods – both groups improved. In the following 9 months, the CBT group continued to improve. Conclusions: The authors indicate CBT’s usefulness in this patient group. Sensky T. et al. (2000). A randomized controlled trial of cognitive-behavioral therapy for persistent symptoms in schizophrenia resistant to medication. Arch Gen Psychiatry. 57:165-72.
. A randomized controlled trial of cognitive-behavioral therapy for persistent symptoms in schizophrenia resistant to medication. Arch Gen Psychiatry. 57:")
24
Conclusions Treatment-refractory schizophrenia remains a significant issue in psychiatry along with expansion of the definition. However, research appears to have plateaued in recent years. Of the number of interventions tested over the last 30 years, clozapine stands out, but appears to be underutilized. Numerous psychosocial treatments benefit patients with schizophrenia and should be considered in both initial stages of illness and in those who are treatment-refractory. Refocus on this important group of patients – assessment, comprehensive treatment and new strategies is needed.

Similar presentations
 Countries: Challenges and opportunities Treating Schizophrenia in Low And Middle Income (LAMI) Countries:>")











 and low (>")






