Download presentation
Presentation is loading. Please wait.

1
Inflammatory Muscle Disease ד"ר סוהיל אעמר ראומטולוגיה – הדסה הר הצופים

2
Classification of IMD Adult Polymyositis (PM)
Adult Dermatomyositis (DM)
")
3
Bohan & Peter CRITERIA 1-MUSCLE WEAKNESS 2-ENZYMES 3-EDT=EMG
4-MUSCLE BIOPSY all for PM 5-TYPICAL RASH for DM

4
Classification of IMD Adult Polymyositis Adult Dermatomyositis
Childhood Dermatomyositis Poly/Dermato-myositis associated with malignancy Poly/Dermato-myositis associated with Connective Tissue Disease Inclusion Body myositis Amyopathic Dermatomyositis

5
EPIDEMIOLOGY Annual Incidence: 2-10 case /million
Peak age : and years old Female: Male ratio: 3:1 total 1:1 childhood DM 10:1 PM/DM assoc. CTD Black: White (USA): :1
: 4:1.")
6
CLINICAL MANIFESTATIONS
Weakness of muscles -shoulder girdle - pelvic girdle - neck flexors Myalgia is minimal Constitutional symptoms-fatigue, fever…

7
CLINICAL MANIFESTATIONS
Rheumatic: arthralgia/arthritis 20-70% Pulmonary: interstitial lung disease 10% GIT: esophageal dysmotility 10-30% Cardiac: conduction blocks and arrhythmia Vascular: Raynaud’s phenomenon 20-40% Skin : Rash, livedo reticularis

9
RAYNAUD’S PHENOMENON

10
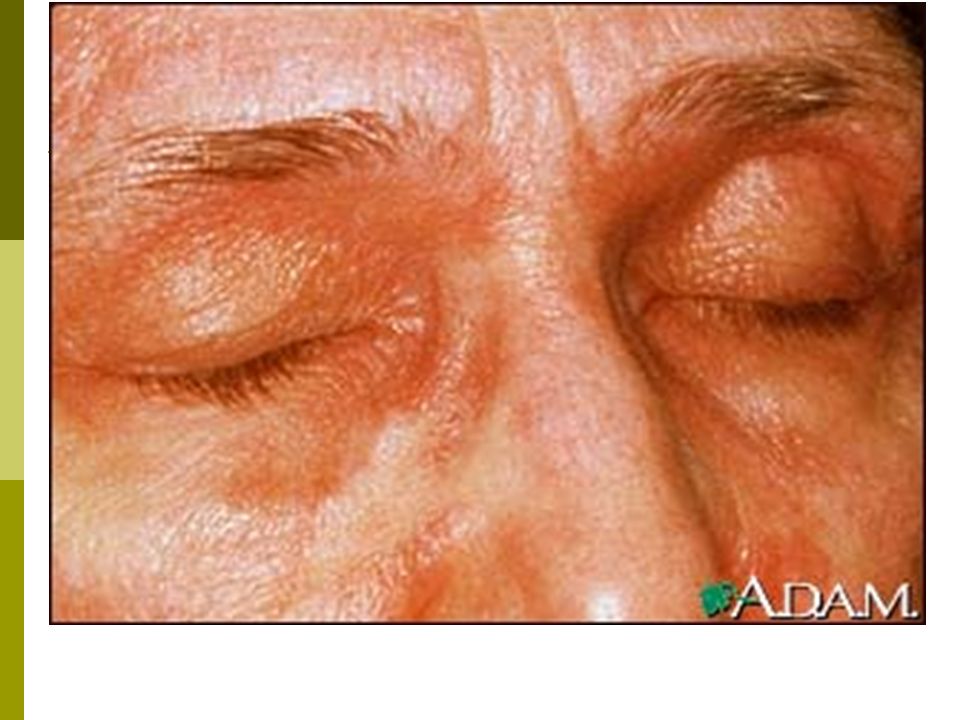
DERMATOLOGIC-SKIN RASH
DERMATOMYOSITIS:- HELIOTROPE RASH: purple /erythematous rash affecting eyelids,periorbital edema +/- malar, forehead and nasolabial folds LIVEDO RETICULARIS- cutis marmorata like

12
Heliotrope Rash

13
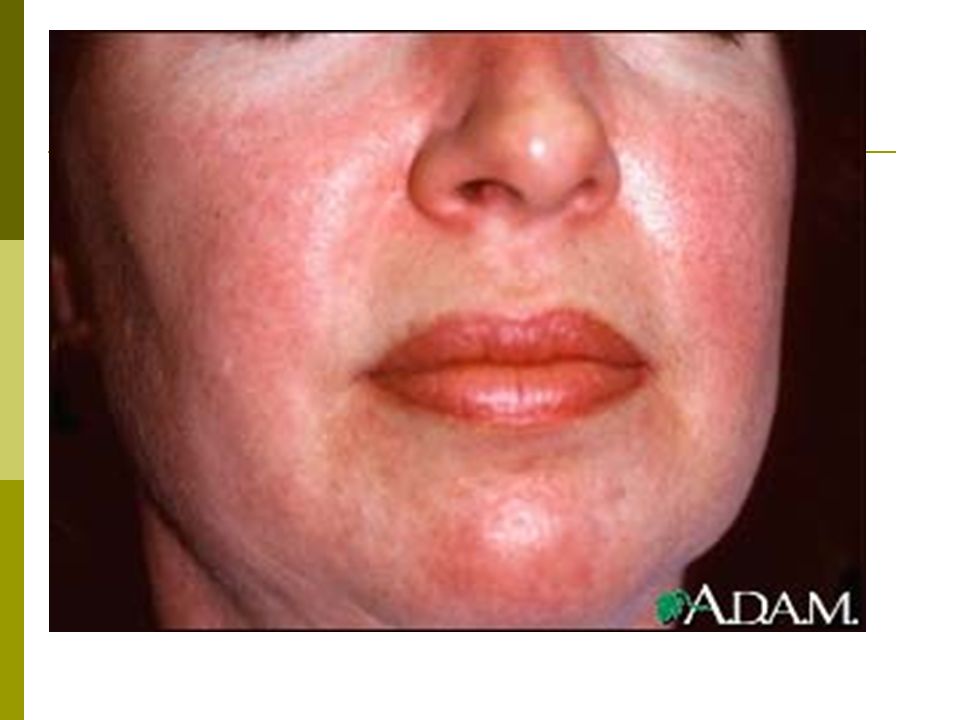
DERMATOLOGIC-SKIN RASH
GOTTRON’S PAPULES: Purple /erythematous raised lesions over knuckles and extensor regions V-SIGN : Erythematous rash over anterior chest and neck. (photosensitivity)
")
19
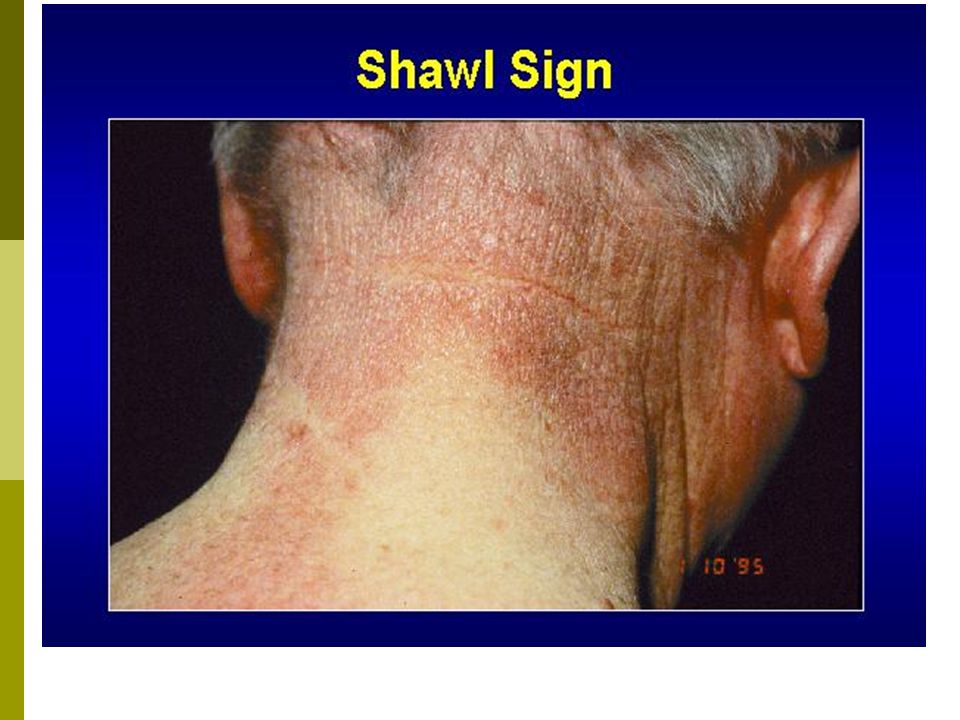
DERMATOLOGIC-SKIN RASH
SHAWL-SIGN: Erythematous rash over the shoulders, upper back and proximal arms HOSTLER SIGN: Erythema over lateral thigh NAILFOLD PATHOLOGY : Cuticular overgrowth and dilated capillary loops

21
PM/DM

23
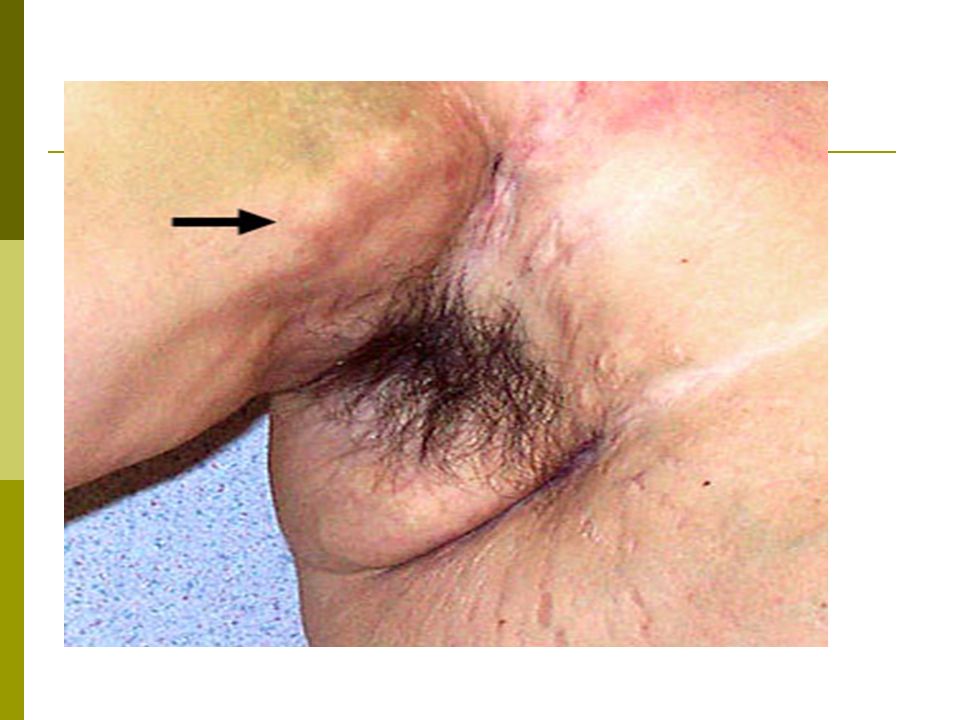
DERMATOLOGIC-SKIN RASH
MECHANIC’S HANDS: Cracking/fissuring the finger pads CALCINOSIS: Subcutaneous calcifications ( exclusive in childhood dermatomyositis)
")
28
DM -childhood

29
DIFFERENTIAL DIAGNOSIS
-MYOPATHY- DRUG/TOXIN -NEURO-MUSCULAR -ENDOCRINE DISEASE -INFECTIOUS MYOSITIS -METABOLIC STORAGE MYOPATHIES -MITOCHONDRIAL MYOPATHY -OTHERS

30
CRITERIA 1-MUSCLE WEAKNESS 2-ENZYMES 3-EDT=EMG 4-MUSCLE BIOPSY

31
DIAGNOSTIC CRITERIA 1. PROXIMAL MOTOR WEAKNESS:
symmetric, proximal muscles 2. HIGH SERUM MUSCLE ENZYMES: CPK, aldolase, myoglobin, AST, ALT, LDH

32
DIAGNOSTIC CRITERIA 3. EDT= electro-diagnostic tests PM/DM
NEUROPATHIC DISORDER PM/DM -Poly-phasic action potentials -long duration -large amplitude -short duration -low amplitude EMG abnormal normal NCV

33
DIAGNOSTIC CRITERIA 4. MUSCLE BIOPSY:
biopsy a clinically weak muscle, contralateral to an abnormal muscle ( by EDT), MRI directed. a. Perivascular and endomysial inflammation CD8+ T cells in PM, CD8+, CD4+ T and B cells in DM b. Muscle fiber necrosis and regeneration
, MRI directed. a. Perivascular and endomysial inflammation. CD8+ T cells in PM, CD8+, CD4+ T and B cells in DM. b. Muscle fiber necrosis and regeneration.")
34
LABORATORY TESTS HIGH MUSCLE ENZYMES:- CPK ELEVATED ESR , CRP:- 50%
POSITIVE ANA: % AUTOANTIBODIES:- anti- RNP (MCTD) anti-PM/Scl (OVERLAP)
 anti-PM/Scl (OVERLAP)")
35
Myositis-specific AUTOANTIBODIES
ANTI Jo-1 part of ANTI SYNTHETASE Ab’s Antibodies to the antigen- Aminoacyl-tRNA synthetase, in 20-50% of PM>>DM ANTI SRP = anti signal recognition particle In 5% of PM ANTI Mi-2 in 10% of DM.

36
ANTI-SYNTHETASE SYNDROME
associated with anti-Jo1 antibodies with acute onset of PM>> DM disease. Associated with ILD %, deforming and non-erosive arthritis, Mechanic’s hands and Raynaud’s phenomenon

37
Myositis-specific AUTOANTIBODIES
Steroid response prognosis HLA Clinical association prevalence Ab’s moderate DR3 Anti-synthetase syndrome 20-50% (PM) Anti-Jo-1 poor bad (cardiac) DR5 Severe PM 5% Anti-SRP good DR7 Classical DM 5-10% (DM) Anti-Mi-2
 Anti-Jo-1. poor. bad. (cardiac) DR5. Severe PM. 5% Anti-SRP. good. DR7. Classical DM. 5-10% (DM) Anti-Mi-2.")
38
INFLAMMATORY MUSCLE DISEASE
1.Adult Polymyositis 2.Adult Dermatomyositis 3.Childhood Dermatomyositis 4.Poly/Dermato-myositis associated with Connective Tissue Disease 5.Poly/Dermato-myositis associated with malignancy 6.Inclusion Body myositis 7.Amyopathic Dermatomyositis

39
Poly/Dermato-myositis associated with malignancy
Associated neoplasms present within the first 2 years of PM/DM followup In PM- 10 % In DM- 15 % Reports of: carcinoma-lung, stomach, ovary lymphoma Routine screening in DM

40
Inclusion Body myositis (IBM)
POLYMYOSITIS M>>F age >50 F>M all ages Demography Prox. And distal proximal Muscle involved Asymmetric Lower >upper Symmetric Legs=arms Neuropathy Cardiac, lung, joints Extra-muscular Myopathic/ neuropathic myopathic EMG

41
Inclusion Body myositis (IBM)
POLYMYOSITIS CD8+ T cells, red-rimmed vacuoles with beta amyloid CD8+ T cells infiltrate Muscle Biopsy ANA= rare ANA=frequent Auto-antibodies no yes Myositis-specific antibodies frequent Response to therapy

42
IMD-PROGNOSIS 5-YEAR SURVIVAL IS AROUND 85% IN PM, DM, PM/DM ASSOC. CTD. MUCH LOWER IN PM/DM ASSOC. MALIGNANCY. Anti-Mi2 Ab’s in DM – better 5-Y-S ,>90% Anti-Jo1 positive decrease 5-Y-S to 65% Anti-SRP Ab’s worsens 5-Y-S to 30%

43
גורמי הרעת פרוגנוזה ב- IMD
גיל מבוגר עיכוב באיבחון עיכוב במתן טיפול סטרואידלי ואימונוספרסיבי ממאירות מעורבות אברים פנימיים IBM חוסר תגובה ראשונית לטיפול נוכחות נוגדנים מריעים פרוגנוזה

44
INFLAMMATORY MUSCLE DISEASE
TREATMENT: 1. STEROIDS 2. IMMUNOSUPPRESSIVE AGENTS: methotrexate, azathioprine, cytoxan, cellcept 3. IMMUNOMODULATORY AGENTS: IVIG, Plasmapheresis 4. REHABILITATION

45
מחלות שריר דלקתיות- טיפול
טיפולים ביולוגים ? נוגדי TNF Anti CD 20 IL-6 antagonist

46
Cytokines in Inflammation
IL-1Ra IL-10 sTNFR IL-1b TNFa Pro-inflammatory Anti-inflammatory

47
Synthesis and Function of TNF
Soluble TNF Macrophage or Activated T Cell Receptor-Bound TNF Transmembrane TNF TNF is a cell-surface protein produced by cells of the immune system (macrophages and activated T cells). It is a central cytokine that plays a major role in the innate immune response and is able to trigger an inflammatory cascade through the induction of secondary mediators. Activated TNF binds to one of 2 receptors, TNF-R1 and TNF-R2. Once TNF is bound to its receptors, mediators are activated (AP-1 and NFB) that induce increased vascular permeability, resulting in an acute inflammatory response. Signal Induction TNF Receptor Target Cell
. It is a central cytokine that plays a major role in the innate immune response and is able to trigger an inflammatory cascade through the induction of secondary mediators. Activated TNF binds to one of 2 receptors, TNF-R1 and TNF-R2. Once TNF is bound to its receptors, mediators are activated (AP-1 and NFB) that induce increased vascular permeability, resulting in an acute inflammatory response. Signal Induction. TNF Receptor. Target Cell.")
48
Inhibition of Cytokines
Normal interaction Neutralization of cytokines Inflammatory cytokine Monoclonal antibody Cytokine receptor Soluble receptor Inflammatory signal No signal Activation of anti-inflammatory pathways Receptor blockade Monoclonal antibody Inhibition of Cytokines Cytokines exert their damaging effects by binding to specific receptors, and there are several potential approaches that can be employed to block these effects. Cytokines can be neutralized through the use of antibodies or soluble receptors. With this approach, the cytokine never reaches the receptor on the cell of interest. This avenue for treatment of RA has been taken with soluble TNF- receptor fusion proteins, soluble IL receptors, monoclonal antibodies against TNF-, and monoclonal antibodies against IL-6. Receptor antagonists or antibodies can bind to cytokine receptors on cells and prevent cytokines from binding. This blocks their actions on the cell in question. This approach to treatment of RA has been taken with recombinant IL-1Ra and an antibody against the IL-6 receptor. Administration of anti-inflammatory cytokines can inhibit expression of inflammatory cytokines. This approach has been taken with IL-4 and IL-10. Choy EHS, Panayi GS. Cytokine pathways and joint inflammation in rheumatoid arthritis. N Engl J Med. 2001;344: Anti-inflammatory cytokine Receptor antagonist Suppression of inflammatory cytokines No signal Adapted with permission from Choy EHS, Panayi GS. N Engl J Med. 2001;344: Copyright © 2001 Massachusetts Medical Society. All rights reserved. 48

49
Humira- The first fully human antiTNFa
Chimeric Humanized Fully Human Humanized Antibody 95% Human Fully Human Antibody 100% Human Chimeric Antibody 70% Human Mouse Human 49

50
אנטי TNF ETANERCEPT= Enbrel REMICADE= Infliximab HUMIRA= Adalimumab
מחלות שריר דלקתיות אנטי TNF ETANERCEPT= Enbrel REMICADE= Infliximab HUMIRA= Adalimumab

52
Research & treatment IMD

53
מרכז רפואי הדסה - הר הצופים
מחלות שריר דלקתיות דר' סוהיל אעמר Suhail Aamar MD, MSc. מומחה בריאומטולוגיה מרכז רפואי הדסה - הר הצופים נובמבר 2013

Similar presentations












>")


>")
 Chronic inflammation of striated muscle (myositis) Characteristic cutaneous features Variety of systemic complications.>")












