Download presentation
Presentation is loading. Please wait.

1
Brain Attack! Stroke is a “Brain Attack.” Stroke happens in the brain not the heart Stroke is an emergency. Call 911 for emergency treatment. Secondary Stroke Prevention Gregory T. Gardziola, D.O Director Cerebrovascular Disease Greenville Health Systems Greenville, South Carolina

2
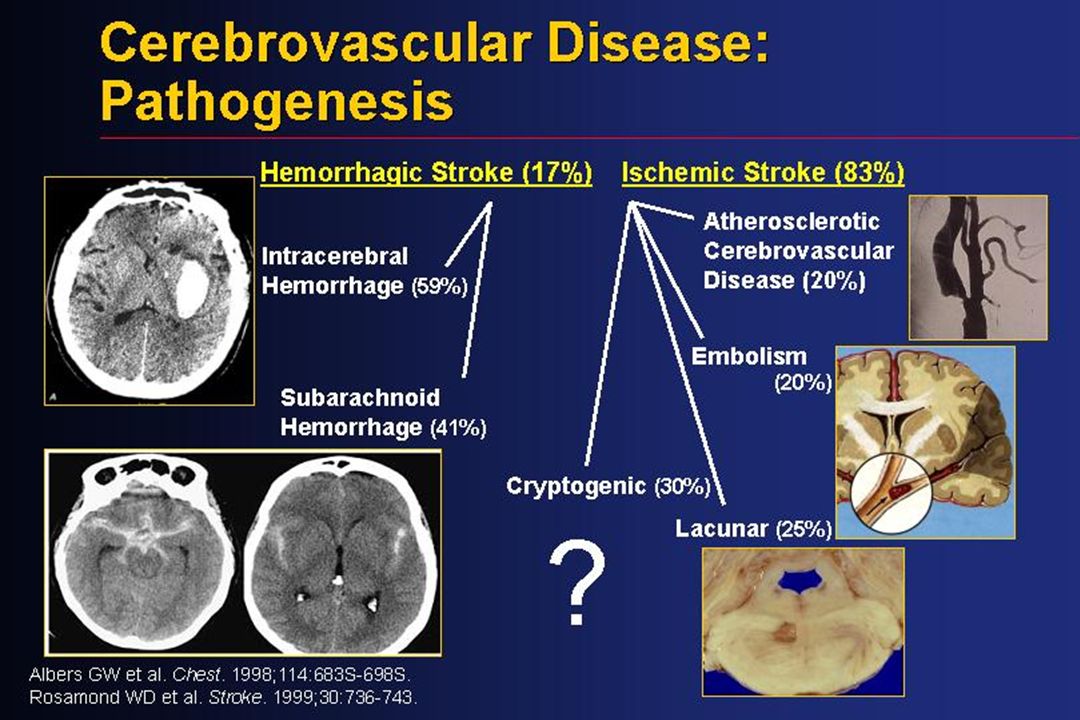
What is a Stroke? Ischemic Stroke – Blockage of a blood vessel resulting in death of brain tissue Ischemic Stroke – Blockage of a blood vessel resulting in death of brain tissue Transient Ischemic Attack – transient blockage of a vessel that results in no permanent damage Transient Ischemic Attack – transient blockage of a vessel that results in no permanent damage Hemorrhagic Stroke – blood outside a vessel Hemorrhagic Stroke – blood outside a vessel

4
Stroke Subtypes ICH 13% SAH 13% Lacunar 19% Thromboembolic 6% Cardioembolic 14% Other 3% Unknown 32% Ischemic 71% Hemorrhagic 26% Data from NINCDS Stroke Data Bank: Foulkes et al. Stroke. 1988;19:547.

5
Stroke Epidemiology > 700,000 new or recurrent strokes occur per year > 700,000 new or recurrent strokes occur per year ~ 4 million Americans are living with neurologic deficits due to stroke ~ 4 million Americans are living with neurologic deficits due to stroke Risk and mortality increase with age Risk and mortality increase with age Risk differs among races and ethnic populations Risk differs among races and ethnic populations Risk is higher in the southeastern U.S. than elsewhere Risk is higher in the southeastern U.S. than elsewhere

6
The High Socioeconomic Cost of Stroke Morbidity and Mortality A leading cause of serious, long-term disability 1 A leading cause of serious, long-term disability 1 700,000 new or recurrent strokes occur per year in the US 1,2 700,000 new or recurrent strokes occur per year in the US 1,2 The third leading cause of death in the US, stroke accounted for 167,661 deaths in 2002 1 ; second leading cause worldwide 3 The third leading cause of death in the US, stroke accounted for 167,661 deaths in 2002 1 ; second leading cause worldwide 3 Economic Impact Total direct and indirect costs exceed $51 billion annually 1 Total direct and indirect costs exceed $51 billion annually 1 Per stroke, the cost of care and treatment exceeds $44,000 and the cost of lost productivity approaches $29,000 1,2 Per stroke, the cost of care and treatment exceeds $44,000 and the cost of lost productivity approaches $29,000 1,2 1 American Heart Association, Heart Disease and Stroke Statistics – 2003 Update. 2 Broderick J, et al. Stroke. 1998; 29:415-421.

7
Risk Factors for Stroke: Non-modifiable Age Age Gender Gender Race-Ethnicity Race-Ethnicity Genetics Genetics

8
Stroke Risk Factors Age – doubles per decade over 55 years Age – doubles per decade over 55 years Sex – 24-30% greater in men Sex – 24-30% greater in men Race Race 2.4 fold increase in African Americans 2.4 fold increase in African Americans 2.0 fold increase in Hispanics 2.0 fold increase in Hispanics Increase among Chinese Increase among Chinese Heredity – 1.9 fold increase in first degree relatives Heredity – 1.9 fold increase in first degree relatives

9
Inroduction 24-30% greater in men 24-30% greater in men 2.4 fold increase in African Americans 2.4 fold increase in African Americans 2.0 increase in Hispanics 2.0 increase in Hispanics

10
Modifiable Risk Factors For Stroke Smoking Smoking Diet Diet Alcohol Alcohol Exercise Exercise

13
Contribution of Selected Risk Factors to Stroke Incidence Hypertension 3.0– 5.0 25 – 56 Cardiac disease2.0 – 4.0 10 – 20 Atrial fibrillation 5.0 – 18.0 1 – 2 Diabetes mellitus 1.5 – 3.0 4 – 8 Cigarette smoking 1.5 – 3.0 20 – 40 Heavy alcohol use 1.0 – 4.0 5 – 30 Adapted from Sacco. In: Gorelick and Alter (eds). Handbook of Neuroepidemiology. New York: Marcel Dekker, Inc; 1994:87, with data from Feinberg. Curr Opin Neurol. 1996;9:46; Gorelick. Stroke. 1994;25:222. Risk FactorRR Prevalence (%)
. Handbook of Neuroepidemiology. New York: Marcel Dekker, Inc; 1994:87, with data from Feinberg. Curr Opin Neurol. 1996;9:46; Gorelick. Stroke. 1994;25:222. Risk FactorRR Prevalence (%).")
15
Hypertension Affects 50 million people in the US Affects 50 million people in the US BP of 140/90 or greater BP of 140/90 or greater Prehypertension 120-139/80-89 Prehypertension 120-139/80-89 Causes shear forces predisposing to atheroma formation and athersosclerosis Causes shear forces predisposing to atheroma formation and athersosclerosis 38% fewer strokes in patients with 10-12 mmHg SBP decrease and 5-6 mmHG DBP reduction 38% fewer strokes in patients with 10-12 mmHg SBP decrease and 5-6 mmHG DBP reduction

16
Hypertension PROGRESS Trial 6105 patients, recent stroke or TIA 6105 patients, recent stroke or TIA Perindopril +/- indapamide or placebo Perindopril +/- indapamide or placebo 28% stroke risk reduction with a mean 9/4 mmHg reduction in the perindopril treated group during 4 years of follow up 28% stroke risk reduction with a mean 9/4 mmHg reduction in the perindopril treated group during 4 years of follow up

17
Hypertension HOPE Trial HOPE Trial 9297 patients with high cardiovascular risk, 1013 with stroke or TIA 9297 patients with high cardiovascular risk, 1013 with stroke or TIA Randomized to ramapril 10 mg/day or placebo Randomized to ramapril 10 mg/day or placebo 32% RRR for stroke with a mean of 3/2 BP reduction over 5 years of followup 32% RRR for stroke with a mean of 3/2 BP reduction over 5 years of followup

18
Hypertension LIFE Trial LIFE Trial 9193 patients with hypertension and LVH 9193 patients with hypertension and LVH Losartan50-100 mg/day or atenolol Losartan50-100 mg/day or atenolol All received HCTZ 12.5-25 mg/day All received HCTZ 12.5-25 mg/day 25% hazard reduction in stroke, no difference in mean BP reduction 25% hazard reduction in stroke, no difference in mean BP reduction

19
Effect of Blood Pressure Control on Incidence of Stroke 6 mm Hg decrease in diastolic blood pressure Antihypertensive stepped- care drug treatment of isolated systolic hypertension Blood pressure reduction in the elderly 40% reduction in incidence of stroke 36% reduction in incidence of stroke 47% reduction in incidence of stroke Adapted from: MacMahon S. Clin Exp Hyperten[A]. 1989;A11. Adapted from: SHEP Cooperative Research Group. JAMA. 1991;265.

20
Original Article High-Dose Atorvastatin after Stroke or Transient Ischemic Attack The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators N Engl J Med Volume 355(6):549-559 August 10, 2006
 Investigators N Engl J Med Volume 355(6): August 10, 2006")
21
Study Overview In this five-year placebo-controlled trial involving patients who had a recent stroke or transient ischemic attack and baseline low-density lipoprotein cholesterol levels of 100 to 190 mg per deciliter (3 to 5 mmol per liter), atorvastatin (80 mg daily) resulted in an absolute reduction in nonfatal or fatal stroke of 2.2 percent and of major cardiovascular events of 3.5 percent In this five-year placebo-controlled trial involving patients who had a recent stroke or transient ischemic attack and baseline low-density lipoprotein cholesterol levels of 100 to 190 mg per deciliter (3 to 5 mmol per liter), atorvastatin (80 mg daily) resulted in an absolute reduction in nonfatal or fatal stroke of 2.2 percent and of major cardiovascular events of 3.5 percent
, atorvastatin (80 mg daily) resulted in an absolute reduction in nonfatal or fatal stroke of 2.2 percent and of major cardiovascular events of 3.5 percent In this five-year placebo-controlled trial involving patients who had a recent stroke or transient ischemic attack and baseline low-density lipoprotein cholesterol levels of 100 to 190 mg per deciliter (3 to 5 mmol per liter), atorvastatin (80 mg daily) resulted in an absolute reduction in nonfatal or fatal stroke of 2.2 percent and of major cardiovascular events of 3.5 percent")
22
Baseline Characteristics of the Patients The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. N Engl J Med 2006;355:549-559

23
Kaplan-Meier Curves for Stroke and TIA The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. N Engl J Med 2006;355:549-559

24
Incidence of Adverse Events and Elevated Laboratory Values The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. N Engl J Med 2006;355:549-559

25
Conclusion In patients with recent stroke or TIA and without known coronary heart disease, 80 mg of atorvastatin per day reduced the overall incidence of strokes and of cardiovascular events, despite a small increase in the incidence of hemorrhagic stroke In patients with recent stroke or TIA and without known coronary heart disease, 80 mg of atorvastatin per day reduced the overall incidence of strokes and of cardiovascular events, despite a small increase in the incidence of hemorrhagic stroke

26
Cigarette Smoking Contributes to over 400,000 deaths related to vascular disease Contributes to over 400,000 deaths related to vascular disease Overall stroke risk increase of 50% over nonsmokers Overall stroke risk increase of 50% over nonsmokers Endothelial damage predisposing to atherosclerosis Endothelial damage predisposing to atherosclerosis Enhanced platelet aggregation, increased fibrinogen, vasoconstriction Enhanced platelet aggregation, increased fibrinogen, vasoconstriction

27
Lightwood JM, Glantz SA. Circulation. 1997;96:1089-1096. Benefits of Smoking Cessation 150200250050100 0 1 2 3 4 Estimated Relative Risk of Stroke Months

28
Exercise May decrease stroke risk by lowering blood pressure, increasing HDL cholesterol, promot weight reduction, help manage blood sugars May decrease stroke risk by lowering blood pressure, increasing HDL cholesterol, promot weight reduction, help manage blood sugars Exercise at least 30 minutes per day Exercise at least 30 minutes per day Dose response for intensity and duration Dose response for intensity and duration 63% odds reduction for stroke with regular exercise 63% odds reduction for stroke with regular exercise

29
Matching for Age, Gender, and Race and Adjusting for HTN, DM, PVD, Smoking, Cardiac Disease, Obesity, Heavy Alcohol, Activities Limited for Medical Reasons, Education Sacco RL et al. Stroke. 1998;29:380-387. Physical Activity and Ischemic Stroke— Northern Manhattan Stroke Study Odds Ratio Physical Activity 0.38 1.0

30
Gorelick, PB. Stroke Prevention. Arch Neurol. 1995;52:347-355. Stroke Prevention: How Many Strokes in the United States Can Be Prevented? 050,000100,000150,000200,000250,000 Number of Strokes Prevented 23,500 47,000 61,500 100,000 246,500 Heavy alcohol use Atrial fibrillation Cigarettes Cholesterol Hypertension

32
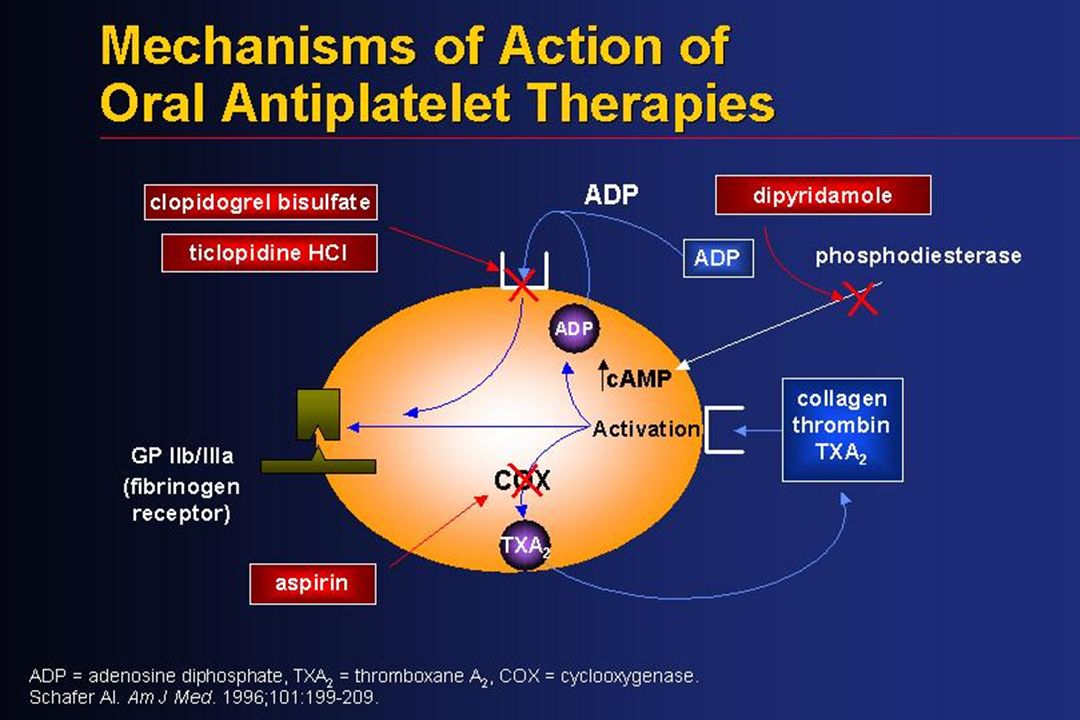
Mechanisms of Action of Antiplatelet Agents Aspirin Ticlopidine/ Clopidogrel Dipyridamole Inhibition of platelet activation and aggregation Block ADP receptors Inhibits cyclooxygenase and thromboxane A 2 Increases plasma adenosine Inhibits platelet phosphodiesterase

34
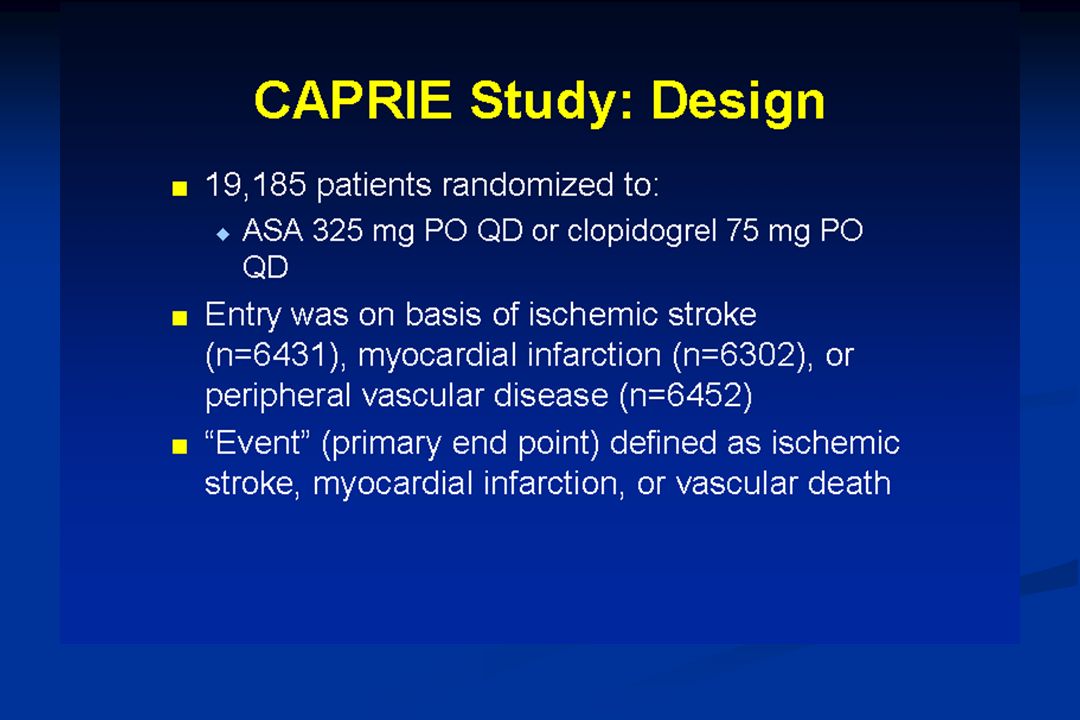
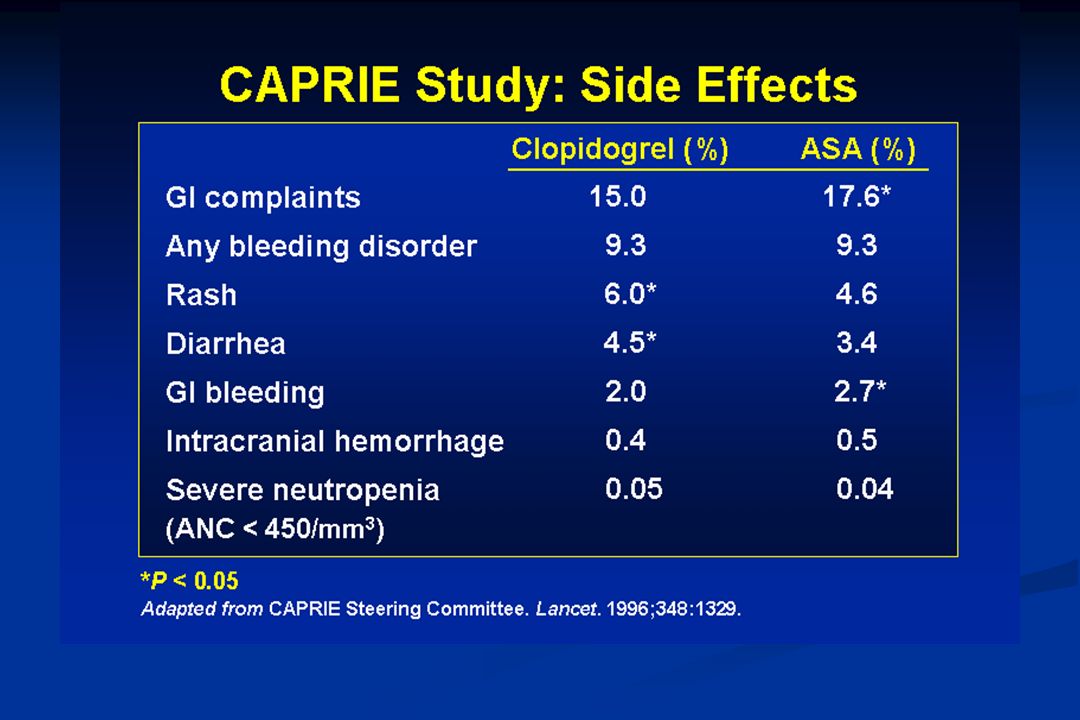
CAPRIE

36
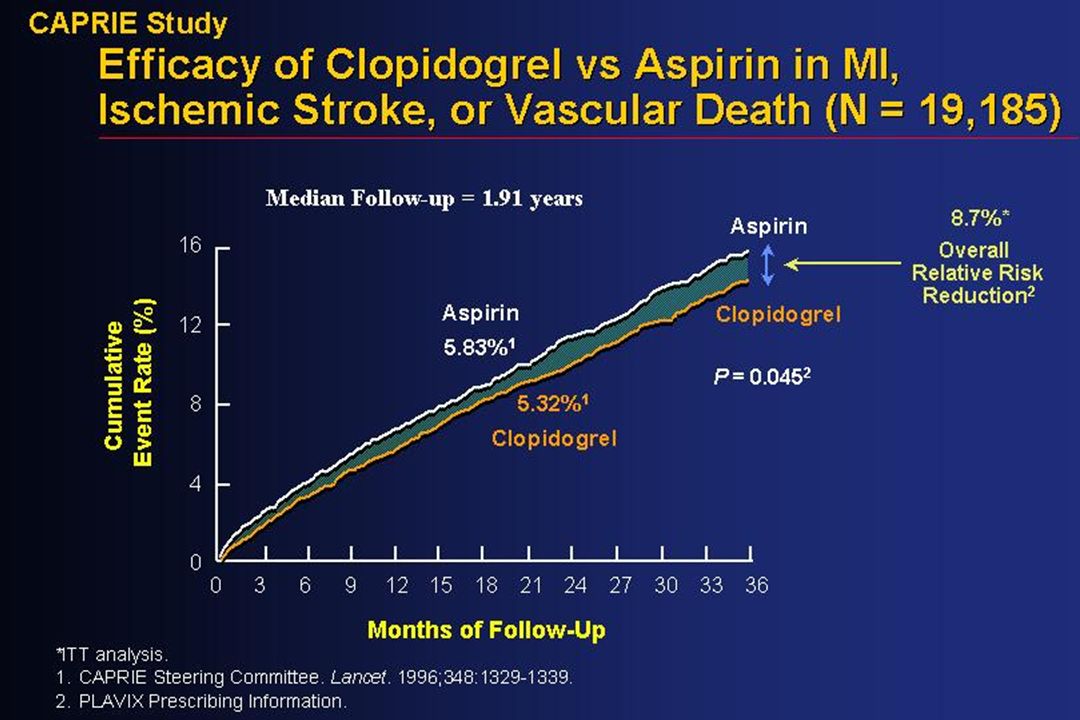
CAPRIE Study: Efficacy* † 2-year study, N = 19,185, endpoint incidence calculated per year. ‡ P < 0.05 Endpoint † Stroke Stroke, MI, or vascular death RRR Stroke Patients 8.0% 7.3% MI Patients –1.0% –3.7% PAD Patients 1.2% 23.8% ‡ Total 6.1% 8.7% ‡ CAPRIE Steering Committee. Lancet. 1996;348:1329. * Clopidogrel (75 mg qd) vs ASA (325 mg qd).
 vs ASA (325 mg qd)..")
39
ESPS 2

40
ESPS-2: The Second European Stroke Prevention Study Tested efficacy of ASA/ER-DP for secondary stroke prevention Tested efficacy of ASA/ER-DP for secondary stroke prevention Addressed clinical questions Addressed clinical questions Does low-dose ASA prevent stroke? Does low-dose ASA prevent stroke? Does ER-DP prevent stroke? Does ER-DP prevent stroke? Is ASA/ER-DP superior to ASA alone? To ER-DP alone? Is ASA/ER-DP superior to ASA alone? To ER-DP alone? Is ASA/ER-DP well tolerated? Is ASA/ER-DP well tolerated? The ESPS-2 Group. J Neurol Sci. 1997;151:S3. Diener et al. J Neurol Sci. 1996;143:1.

41
ESPS-2: Endpoints Primary endpoints Stroke (any type, fatal or nonfatal) Stroke (any type, fatal or nonfatal) Death from any cause Death from any cause Selected secondary endpoint Ischemic events (stroke, MI, or sudden death) Ischemic events (stroke, MI, or sudden death)
 Stroke (any type, fatal or nonfatal) Death from any cause Death from any cause Selected secondary endpoint Ischemic events (stroke, MI, or sudden death) Ischemic events (stroke, MI, or sudden death)")
42
ESPS-2: Treatment Arms N = 6,602 Placebo (n = 1,649) ER-DP 200 mg bid (n = 1,654) ASA 25 mg bid (n = 1,649) ASA/ER-DP 25 mg ASA/ 200 mg ER-DP bid (n = 1,650)
 ER-DP 200 mg bid (n = 1,654) ASA 25 mg bid (n = 1,649) ASA/ER-DP 25 mg ASA/ 200 mg ER-DP bid (n = 1,650)")
43
ESPS 2: Effects on Stroke—Relative Risk Reduction (Pairwise Comparisons) ER-DP = Extended-Release Dipyridamole ASA = Acetylsalicylic Acid RRR = Relative Risk Reduction 15 ESPS 2 Group. J Neurol Sci. 1997; 151(suppl):S1-S77. 37.0% P < 0.001 16.3% P = 0.039 18.1% P = 0.013 23.1% P = 0.006 0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 30.0% 35.0% 40.0% RRR ASA/ER-DP vs. Placebo ER-DP vs. Placebo ASA vs. Placebo ASA/ER-DP vs. ASA
:S1-S % P < % P = % P = % P = % 5.0% 10.0% 15.0% 20.0% 25.0% 30.0% 35.0% 40.0% RRR ASA/ER-DP vs. Placebo ER-DP vs. Placebo ASA vs. Placebo ASA/ER-DP vs. ASA.")
44
ESPS 2: Adverse Events (Percent within each group) ER-DP = Extended-Release Dipyridamole ASA = Acetylsalicylic Acid Treatment groupDyspepsiaGI BleedingHeadache ASA/ER-DP Placebo ASA ER-DP 18.4 16.7 18.1 17.4 4.1 2.1 3.2 2.2 39.2 32.9 33.8 38.3 *Not statistically different from aspirin * 19 Aggrenox ® (aspirin/extended-release dipyridamole) 25 mg/200 mg capsules product information, Boehringer Ingelheim Pharmaceuticals, Inc.
 ER-DP = Extended-Release Dipyridamole ASA = Acetylsalicylic Acid Treatment groupDyspepsiaGI BleedingHeadache ASA/ER-DP Placebo ASA ER-DP *Not statistically different from aspirin * 19 Aggrenox ® (aspirin/extended-release dipyridamole) 25 mg/200 mg capsules product information, Boehringer Ingelheim Pharmaceuticals, Inc.")
45
ESPS 2: Safety Severe or Fatal Bleeding ASA 20 (1.2%) ER-DP 6 (0.4%) ERDP+ASA 27 (1.6%) Placebo 7 (0.4%) n.s. ER-DP = Extended-Release Dipyridamole ASA = Acetylsalicylic Acid 15 ESPS 2 Group. J Neurol Sci. 1997; 151(suppl):S1-S77.
:S1-S77..")
46
MATCH

47
To be eligible for the study the patient must : 1) Have experienced a TIA or IS within the last 3 months (randomization as soon as possible after the qualifying event) and 2) Have at least 1 additional vascular risk factor within the previous 3 yrs previous IS previous MI angina pectoris symptomatic PAD diabetes mellitus and 3) Meet no exclusion criteria Diener H-C et al on behalf of the MATCH Investigators. Cerebrovasc Dis. 2004;17:253-261. PLAVIX backup slide. MATCH Inclusion Criteria

48
The following patients were excluded from the MATCH trial if they met any of the following criteria: Age < 40 years Age < 40 years Severe co-morbid conditions Severe co-morbid conditions At risk of increased bleeding At risk of increased bleeding Scheduled for major surgery or vascular surgery Scheduled for major surgery or vascular surgery Have a contraindication for ASA or clopidogrel Have a contraindication for ASA or clopidogrel Diener H-C et al on behalf of the MATCH Investigators. Cerebrovasc Dis. 2004;17:253-261. PLAVIX backup slide. MATCH Exclusion Criteria

49
MATCH Primary Endpoint RRR = 6.4% p=.244

50
MATCH p< 0.001

51
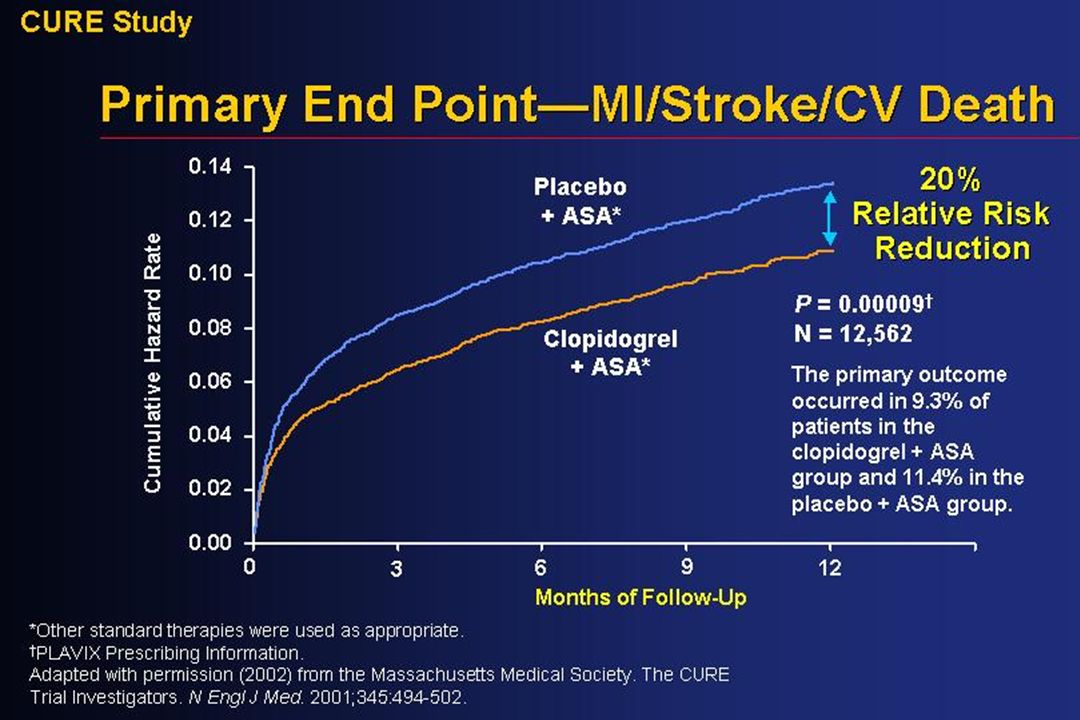
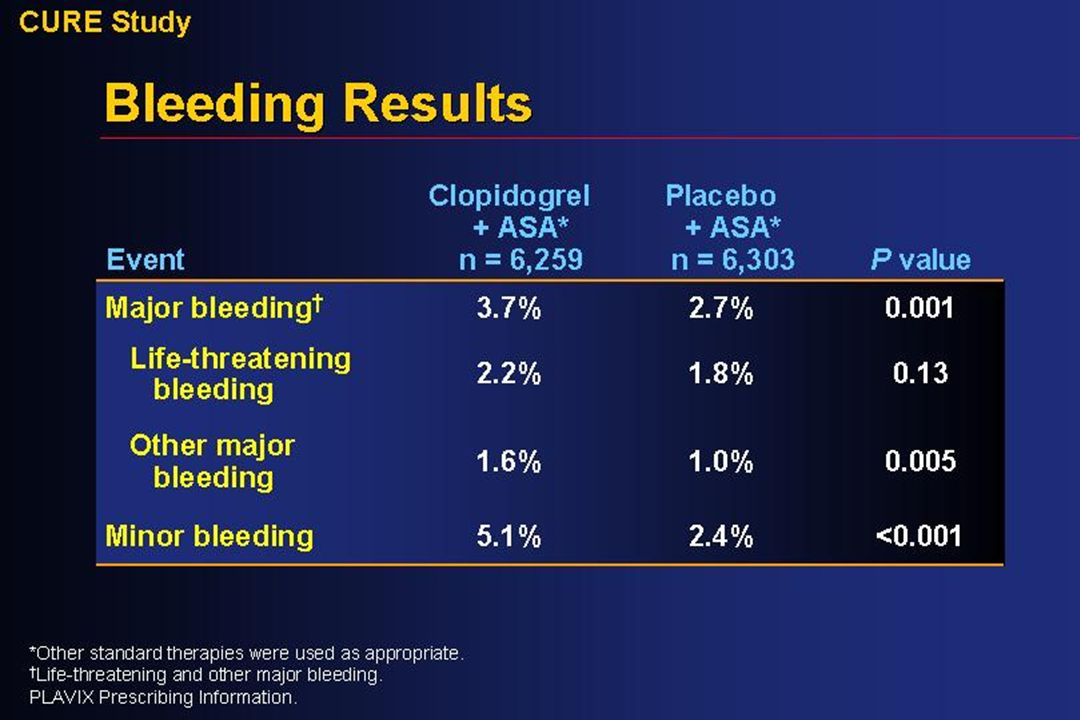
Clopidogrel in Unstable Angina to Prevent Recurrent Events Study CURE

57
Original Article Aspirin and Extended-Release Dipyridamole versus Clopidogrel for Recurrent Stroke Ralph L. Sacco, M.D., Hans-Christoph Diener, M.D., Ph.D., Salim Yusuf, M.B., B.S., D.Phil., Daniel Cotton, M.S., Stephanie Ôunpuu, Ph.D., William A. Lawton, B.A., Yuko Palesch, Ph.D., Reneé H. Martin, Ph.D., Gregory W. Albers, M.D., Philip Bath, F.R.C.P., Natan Bornstein, M.D., Bernard P.L. Chan, M.D., Sien-Tsong Chen, M.D., Luis Cunha, M.D., Ph.D., Björn Dahlöf, M.D., Ph.D., Jacques De Keyser, M.D., Ph.D., Geoffrey A. Donnan, M.D., Conrado Estol, M.D., Ph.D., Philip Gorelick, M.D., Vivian Gu, M.D., Karin Hermansson, D.M.Sc., Lutz Hilbrich, M.D., Markku Kaste, M.D., Ph.D., Chuanzhen Lu, M.D., Thomas Machnig, M.D., Prem Pais, M.D., Robin Roberts, M.Tech., Veronika Skvortsova, M.D., Philip Teal, M.D., Danilo Toni, M.D., Cam VanderMaelen, Ph.D., Thor Voigt, M.D., Michael Weber, M.D., Byung-Woo Yoon, M.D., Ph.D., for the PRoFESS Study Group N Engl J Med Volume 359(12):1238-1251 September 18, 2008
: September 18,")
58
Study Overview In this large clinical trial, aspirin plus extended- release dipyridamole was found to have an efficacy similar to that of clopidogrel in the prevention of recurrent stroke In this large clinical trial, aspirin plus extended- release dipyridamole was found to have an efficacy similar to that of clopidogrel in the prevention of recurrent stroke However, aspirin plus extended-release dipyridamole resulted in more bleeding, including intracranial bleeding However, aspirin plus extended-release dipyridamole resulted in more bleeding, including intracranial bleeding The results will help guide therapy for secondary stroke prevention The results will help guide therapy for secondary stroke prevention

59
Kaplan-Meier Estimates of the Cumulative Probability of Primary and Secondary Outcomes, According to Treatment Group Sacco RL et al. N Engl J Med 2008;359:1238-1251

60
Hazard Ratios for Primary, Secondary, and Key Tertiary Efficacy and Safety Outcomes Sacco RL et al. N Engl J Med 2008;359:1238-1251

61
Hazard Ratios for the Primary Outcome of First Recurrence of Stroke, According to Prespecified and Post Hoc Baseline Characteristics Sacco RL et al. N Engl J Med 2008;359:1238-1251

62
Conclusion The trial did not meet the predefined criteria for noninferiority but showed similar rates of recurrent stroke with ASA-ERDP and with clopidogrel The trial did not meet the predefined criteria for noninferiority but showed similar rates of recurrent stroke with ASA-ERDP and with clopidogrel There is no evidence that either of the two treatments was superior to the other in the prevention of recurrent stroke There is no evidence that either of the two treatments was superior to the other in the prevention of recurrent stroke

63
Original Article Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke Werner Hacke, M.D., Markku Kaste, M.D., Erich Bluhmki, Ph.D., Miroslav Brozman, M.D., Antoni Dávalos, M.D., Donata Guidetti, M.D., Vincent Larrue, M.D., Kennedy R. Lees, M.D., Zakaria Medeghri, M.D., Thomas Machnig, M.D., Dietmar Schneider, M.D., Rüdiger von Kummer, M.D., Nils Wahlgren, M.D., Danilo Toni, M.D., for the ECASS Investigators N Engl J Med Volume 359(13):1317-1329 September 25, 2008
: September 25,")
64
Study Overview Intravenous thrombolysis with alteplase improves the outcomes after acute stroke when alteplase is given within 3 hours after the onset of symptoms Intravenous thrombolysis with alteplase improves the outcomes after acute stroke when alteplase is given within 3 hours after the onset of symptoms In this randomized trial involving patients who presented between 3 and 4.5 hours after the onset of stroke, clinical outcomes were modestly better in patients treated with alteplase than in patients given placebo (favorable outcome in 52% vs. 45% of patients) In this randomized trial involving patients who presented between 3 and 4.5 hours after the onset of stroke, clinical outcomes were modestly better in patients treated with alteplase than in patients given placebo (favorable outcome in 52% vs. 45% of patients)
 In this randomized trial involving patients who presented between 3 and 4.5 hours after the onset of stroke, clinical outcomes were modestly better in patients treated with alteplase than in patients given placebo (favorable outcome in 52% vs. 45% of patients).")
65
Numbers of Patients Who Were Enrolled, Randomly Assigned to a Study Group, and Included in the Per-Protocol Population Hacke W et al. N Engl J Med 2008;359:1317-1329

66
Demographic and Baseline Characteristics of the Patients Hacke W et al. N Engl J Med 2008;359:1317-1329

67
Major Inclusion and Exclusion Criteria Hacke W et al. N Engl J Med 2008;359:1317-1329

68
Odds Ratios for Primary End Point and Secondary End Point, Including Components, in the Intention-to-Treat and Per-Protocol Populations at 90 Days Hacke W et al. N Engl J Med 2008;359:1317-1329

69
Conclusion As compared with placebo, intravenous alteplase administered between 3 and 4.5 hours after the onset of symptoms significantly improved clinical outcomes in patients with acute ischemic stroke; alteplase was more frequently associated with symptomatic intracranial hemorrhage As compared with placebo, intravenous alteplase administered between 3 and 4.5 hours after the onset of symptoms significantly improved clinical outcomes in patients with acute ischemic stroke; alteplase was more frequently associated with symptomatic intracranial hemorrhage

70
In Summary Stroke is a heterogenous disorder with multiple risk factors Stroke is a heterogenous disorder with multiple risk factors Risk factor modification can have significant impact on stroke risk reduction. This can be prescriptive or lifestyle changes or a combination Risk factor modification can have significant impact on stroke risk reduction. This can be prescriptive or lifestyle changes or a combination Stroke identification is important if we wish to treat stroke acutely Stroke identification is important if we wish to treat stroke acutely

71
Thank You

Similar presentations




>")












>")



