Download presentation
Presentation is loading. Please wait.

1
Morning Report: Thursday, April 5 th

4
Bacterial meningitis is more common in the first month than at any other time in life Mortality rate has declined from 50% in the 1970s to 10-15% currently BUT, the morbidity rate is relatively unchanged Incidence 0.25-0.32/1000 live births Occurs in up to 15% of neonates with bacteremia

5
LBW (<2500g) Preterm birth (<37 wga) PROM Septic or traumatic delivery Fetal hypoxia Maternal peripartum infection Galactosemia Urinary tract abnormalities
 Preterm birth (<37 wga) PROM Septic or traumatic delivery Fetal hypoxia Maternal peripartum infection Galactosemia Urinary tract abnormalities")
6
Early-onset infections (first 3-6 days after birth) Reflect vertical transmission from maternal genital tract flora Late-onset infections (after first week of life) Suggest nosocomial or community acquisition (Maternal flora may still be a source)
 Reflect vertical transmission from maternal genital tract flora Late-onset infections (after first week of life) Suggest nosocomial or community acquisition (Maternal flora may still be a source)")
7
The “bugs” GBS E.Coli Other gram-negative bacilli Other gram positive organisms constitute a higher portion of disease burden among VLBW infants Enterococcus Coagulase-negative staphylococci S. aureus L. monocytogenes Alpha-hemolytic streptococci

8
Temperature instability (60%) Term infants: temp> 38C Preterm infants: temp< 36C Neurologic symptoms Irritability/ lethargy (60%) Poor tone Tremors/twitching/seizures (20-50%) Focal More common presentation in gram-negative meningitis Full fontanelle
 Term infants: temp> 38C Preterm infants: temp< 36C Neurologic symptoms Irritability/ lethargy (60%) Poor tone Tremors/twitching/seizures (20-50%) Focal More common presentation in gram-negative meningitis Full fontanelle")
9
Other Poor feeding/ vomiting (50%) Respiratory distress (33-50%) Apnea (10-30%) Diarrhea (20%)
 Respiratory distress (33-50%) Apnea (10-30%) Diarrhea (20%)")
10
Full septic work-up CBC BCx UA/ UCx (if > 6 days of age) LP Glucose Protein Cell count and differential Gram stain Culture
 LP Glucose Protein Cell count and differential Gram stain Culture")
12
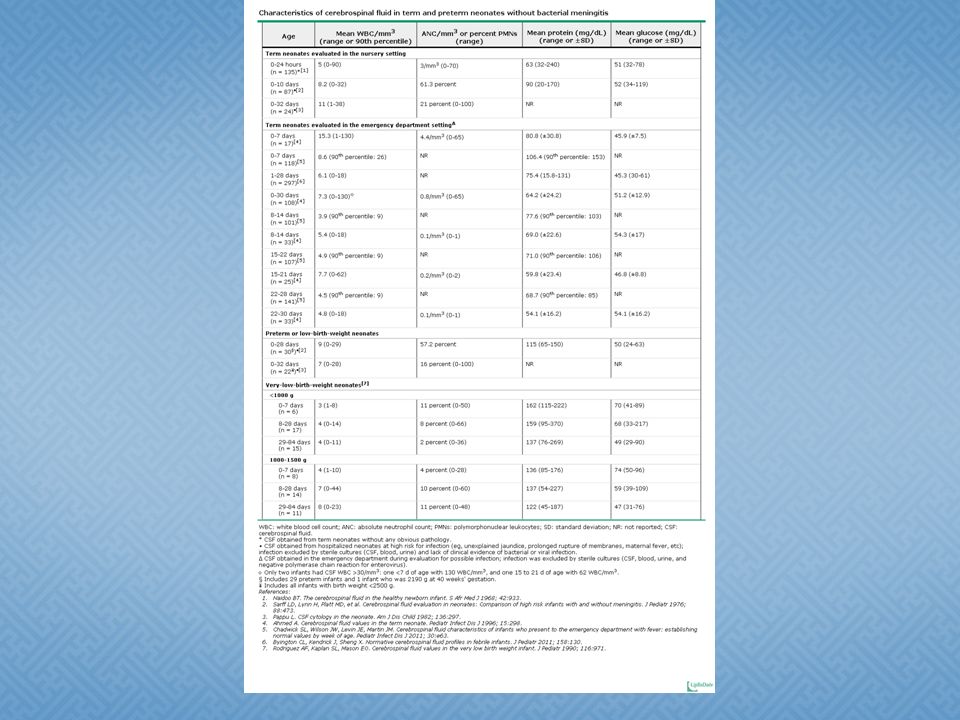
WBCProteinGlucose Term infant>1000 WBC/microL* Neutrophils >100 mg/dL<30 mg/dL Preterm infant>1000 WBC/microL* Neutrophils >150 mg/dL<20 mg/dL PEARLS OF CSF WISDOM : 1.CSF WBC ct may be lower with gram-positive organisms 2. In 20% of patients with culture-confirmed meningitis, the gram stain will be negative (especially with L. monocytogenes) 3.Adjustment of WBC in the setting of a traumatic LP can result in loss of sensitivity with only a marginal gain in specificity
 3.Adjustment of WBC in the setting of a traumatic LP can result in loss of sensitivity with only a marginal gain in specificity.")
13
CSF culture Negative cultures rely on cell count and protein LP was delayed until after antibiotic administration IAP

14
Empiric therapy Early-onset Ampicillin and gentamicin OR Ampicillin and cefotaxime OR If Listeria and Enterococcus are unlikely Ampicillin and gentamicin and cefotaxime If a gram-negative organism is strongly suspected Late-onset Non-hospitalized neonates Ampicillin and gentamicin OR Ampicillin and gentamicin and cefotaxime Hospitalized neonates Vancomycin, gentamicin, cefotaxime Vancomycin, ampicillin, gentamicin

15
Specific therapy GBS: Ampicillin or PCN+ Gentamicin sterility PCN G monotherapy Gram-negative enterics: Ampicillin (for amp- susceptible strains), Cefotaxime+ Gentamicin sterility 7-14 days of continued combination therapy Cefotaxime monotherapy Listeria: Ampicillin and Gentamicin Coagulase-negative staphylococci: Vancomycin
, Cefotaxime+ Gentamicin sterility 7-14 days of continued combination therapy Cefotaxime monotherapy Listeria: Ampicillin and Gentamicin Coagulase-negative staphylococci: Vancomycin")
16
Positive CSF culture Gram-positives (uncomplicated course): 14 days Gram-negatives: 21 days (minimum) Ventriculitis, abscess, multiple areas of infarction: up to 8 weeks
: 14 days Gram-negatives: 21 days (minimum) Ventriculitis, abscess, multiple areas of infarction: up to 8 weeks")
17
Acute Ventriculitis Abscess Infarction Hydrocephalus Subdural effusion Chronic Developmental delay (25%) Late-onset seizures (20%) CP (20%) Hearing loss (10%) Cortical blindness (<10%)
 Late-onset seizures (20%) CP (20%) Hearing loss (10%) Cortical blindness (<10%)")
18
Noon is free!!

Similar presentations






 –Physical exam findings unreliable –Immunologic.>")











 TB Fungal Chemical Parasitic ? Carcinomatous.>")
